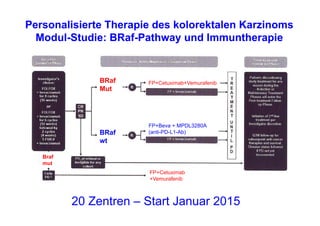
Das Dokument behandelt verschiedene Aspekte der Onkologie, einschließlich präventiver Ansätze, personalisierter Therapien und neuer Immuntherapien gegen Krebs. Es werden Ergebnisse von mehreren Studien zu Screening-Methoden und Behandlungsprotokollen vorgestellt, darunter der Vergleich von Rivaroxaban und Enoxaparin bei venösen Thromboembolien sowie Fortschritte in der Behandlung von Krebsarten wie Melanom und nicht-kleinzelligem Lungenkarzinom. Die Dokumentation spiegelt die Entwicklungen in der Krebsforschung und -therapie wider und betont die Bedeutung von individualisierten Behandlungsstrategien.