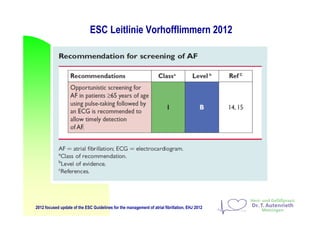
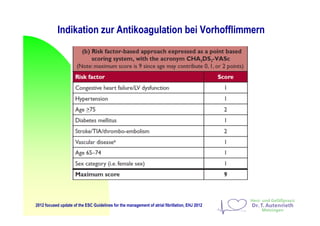
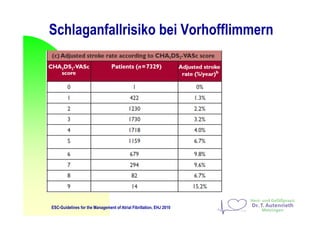
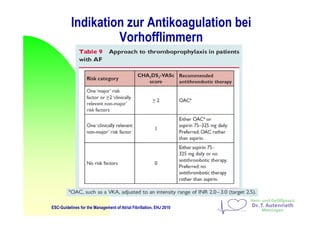
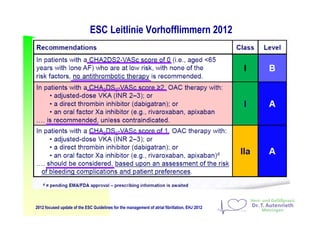
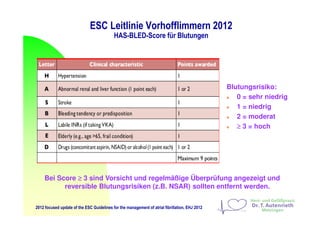
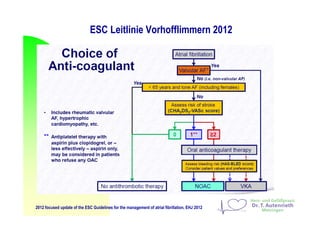
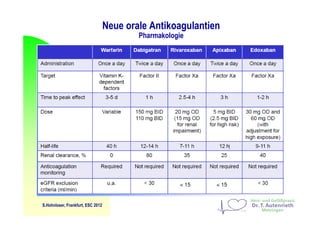
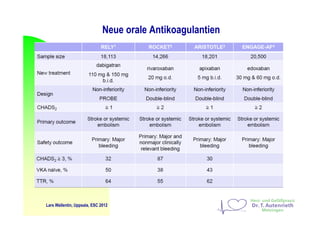
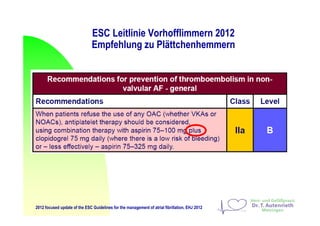
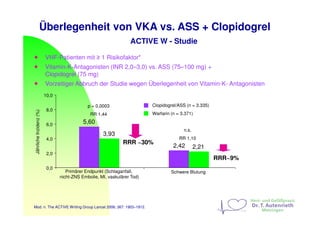
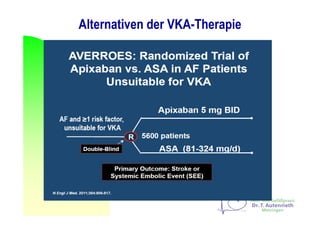
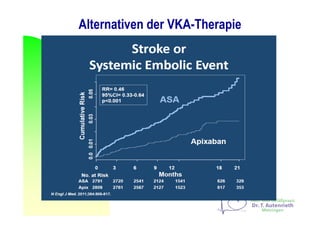
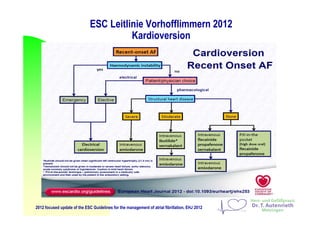
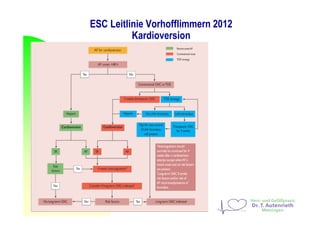
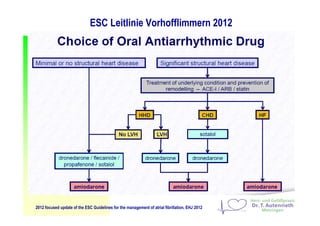
Vorhofflimmern ist die häufigste Herzrhythmusstörung, die mehr als 1,8 Millionen Menschen in Deutschland betrifft, wobei das Risiko mit dem Alter steigt. Die ESC-Leitlinien 2012 geben klare Empfehlungen zur Antikoagulation bei Vorhofflimmern zur Schlaganfallprävention sowie zur Behandlung und zum Management, einschließlich der Verwendung neuer oraler Antikoagulantien. Es werden auch aktuelle Daten zur Effektivität und Sicherheit dieser Behandlungen sowie zu antidotalen Therapien präsentiert.