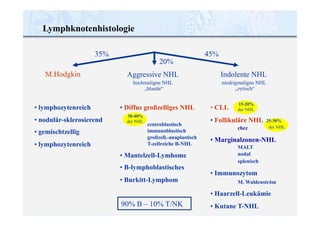
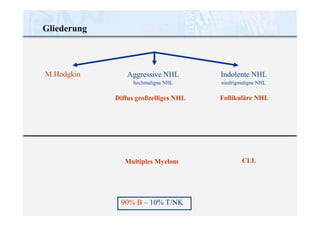
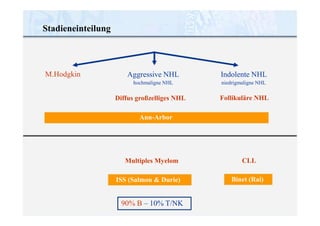
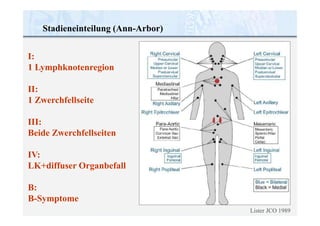
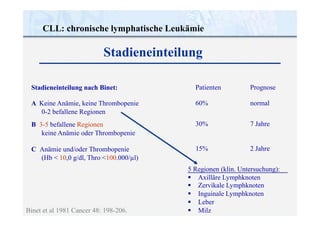
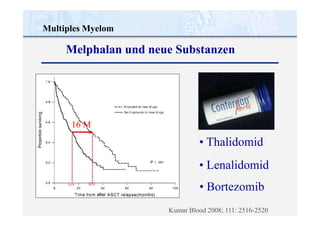
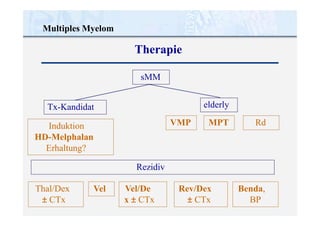
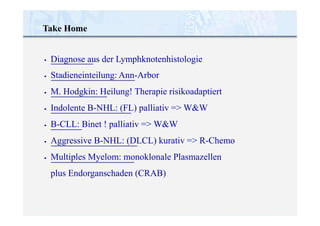
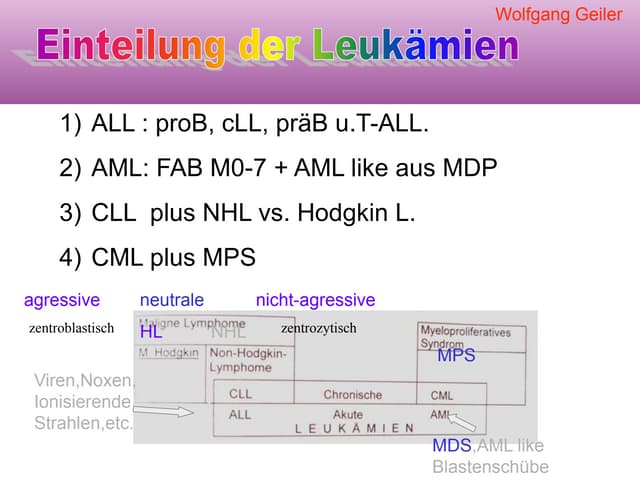
Das Dokument behandelt die Diagnostik und Therapie von malignen Lymphomen und Multiplem Myelom, insbesondere die Klassifikation und Stadieneinteilung dieser Erkrankungen sowie die entsprechenden Behandlungsstrategien. Es werden verschiedene Typen von Lymphomen, deren Prognosen und Behandlungsmöglichkeiten beschrieben, darunter sowohl kurative als auch palliative Ansätze, abhängig vom Stadium der Erkrankung. Zudem werden insbesondere die Einteilung nach Ann-Arbor für Hodgkin-Lymphom und die Binet-Klassifikation für chronische lymphatische Leukämie (CLL) erläutert.