
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Cementum in health and disease
Ähnlich wie Cementum in health and disease (20)
Mehr von Dr. Virshali Gupta
Mehr von Dr. Virshali Gupta (11)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Cementum in health and disease
- 2. CONTENTS INTRODUCTION DEFINITIONS DEVELOPMENT OF CEMENTUM PHYSICAL CHARACTERISTICS CHEMICAL CHARACTERISTICS CEMENTUM PROTEINS CLASSIFICATION CELLS FUNCTIONS RESORPTION AND REPAIR CEMENTUM IN PERIODONTAL DISEASE AGE CHANGES IN CEMENTUM ANOMALIES IN CEMENTUM CLINICAL CORRELATION REFERENCES 2/41
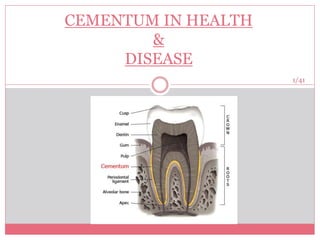
- 3. INTRODUCTION The periodontium consists of those tissues which surrounds & support the tooth & is composed of: gingiva, PDL, cementum & alveolar bone. Cementum was first demonstrated microscopically in 1853 by Frankel and Raschkow. The word cementum comes from the Latin word “cement” which means quarried stone. 3/41
- 4. DEFINITIONS Thin, calcified tissue of ectodermal origin covering the roots of the teeth in which embedded collagen fibers attach the teeth to alveolus. (GPT, 2004) Calcified, avascular mesenchymal tissue that forms the outer covering of the anatomic root. (Carranza 10th ed) Mineralized connective tissue that covers the roots of the teeth. (Listgarten 1st ed) 4/41
- 5. DEVELOPMENT OF CEMENTUM ( CEMENTOGENESIS) HERS derived from the inner & outer enamel epithelium induces secretion of enamel protein. Sends inductive signal to ectomesenchymal pulp cells to secrete pre-dentin by differentiating into odontoblasts HERS becomes interrupted Ectomesenchymal cells from the inner portion of the dental follicle come in contact with pre-dentin by differentiating into cementoblasts Cementoblasts lay down CEMENTUM 5/41
- 6. PHYSICAL CHARACTERISTICS Hardness- less than dentin. Colour- light yellow with dull surface & lighter than dentin. Thickness- variable. thinnest at CEJ (20-50 µm) thickest at apex (150-200 µm) Permeability- permeable. As age progress- cementum diminishes. 6/41
- 7. CHEMICAL CHARACTERISTICS Organic content and water - 50 – 55% Inorganic content - 45 – 50 % ORGANIC CONTENT • Collagen fibers embedded in an interfibrillar ground substance consisting of glycoproteins. • Types of collagen :- Type I, Type III, Type V, Type IX, Type XIV • Cementum proteins. 7/41
- 8. CEMENTUM PROTEINS GLYCOSAMINOGLYCANS: Proteoglycans creates the cemental incremental lines only in cellular cementum. Major GAGs: hyaluronic acid, dermatan sulfate, chondratin sulfate & keratan sulfate. Play major regulatory roles during cementum mineralization and are associated with initial phase of cementum formation. BONE SIALOPROTEIN & OSTEOPONTIN: Play a major role in filling spaces created during collagen assembly. Regulators of hydroxyapitite crystal nucleation and growth. Role in differentiation of cementoblast progenitor cells to cementoblasts. 8/41
- 9. Osteopontin regulates cell migration, differentiation & survival. Sialoprotein modulates the process of cementogenesis & is involved in the process of chemo attraction, adhesion & differentiation of precementoblasts. ALKALINE PHOSPHATASE: Play imp role in skeletal mineralization. Regulate tissue turnover & cell proliferation, differentiation, maturation. Major function: hydrolysis of inorganic pyrophosphate, a potent inhibitor of hydroxyapitite formation. Plays key biological role in the mineralization of bone & cementum. 9/41
- 10. CEMENTUM- SPECIFIC PROTEINS: CEMENTUM- DERIVED GROWTH FACTOR: Insulin- like growth factor-1 like molecule. Repair or regulate tissues. Ability of cell migration, adhesion, mitogenic activity & differentiation, essential for periodontal regeneration. Cementum has the potential to regulate the metabolism & turn over of surrounding tissues because of this growth factor. CEMENTUM ATTACHMENT PROTEIN (CAP): Promotes the attachment of gingival fibroblasts, endothelial cells & smooth muscle cells, but not oral sulcular epithelial cells . Capacity to direct cell migration of alveolar bone cells. Binds selectively to periodontal ligament cells and supports periodontal ligament cell attachment to root surfaces. 10/41
- 11. CEMENTUM PROTEIN-I : Synthesized by Hertwig’s epithelial root sheath cells. Play a role during the biomineralization process & is required for the synthesis of needle- like shape crystals. Present throughout the entire cementum surface, including the cementoid phase of acellular & cellular cementum, cementocytes & cells near blood vessels in the PDL. Associated with the regulation of sialoprotein expression in cementoblasts. 11/41
- 12. ENAMEL- ASSOCIATED PROTEINS IN CEMENTUM: Synthesized by Hertwig’s epithelial root sheath cells. Results in the formation of a cellular- like tissue or bone with the characteristics of cellular intrinsic fiber cementum. Functions: promotion of cell proliferation, differentiation & up-regulation of extracellular matrix production. Involved in root formation. 12/41
- 13. OSTEONECTIN Mainly secreted by osteoblasts (Gage et al; 1989). Important for mineralization process. Found in the PDL. OSTEOCALCIN Also k/as bone Gla protein as it contains -carboxyglutamic acid (Gla) residues. Mainly secreted by osteoblasts (Mariotti, 1993), regulate mineralization process, prevent hypercalcification of the cementum surface. 13/41
- 14. INORGANIC CONTENT Calcium & phosphate in the form of hydroxyapitite. Trace elements like Copper, Fluorine, Iron, Lead, Potassium, Silica, Sodium and Zinc in varying amounts. Cementum has the highest fluoride content. 14/41
- 15. CLASSIFICATION a) BASED ON LOCATION found on the root surface forms on the enamel covering the crown Coronal cementumRadicular cementum 15/41
- 16. b) PRESENCE/ ABSENCE OF CELLS ACELLULAR CEMENTUM CELLULAR CEMENTUM 1) Present on the cervical third or half of root. Present mainly on apical third of root. 2) Does not contain cells. Contain cells called cementocytes in individual spaces lacunae. 3) Formed before the tooth reaches the occlusal plane. Formed after the tooth reaches the occlusal plane. 4) More calcified Less calcified. 5) Sharpey’s fibers are main component which inserted at approximately right angles onto the root surface. Sharpey’s fibers occupy smaller portion & occupy other fibers that are arranged parallel to the root surface. 6) Rate of development is faster . Slow . 7) Incremental lines are wide apart. Closer. 16/41
- 17. C) ORIGIN OF MATRIX FIBERS EXTRINSIC FIBERS INTRINSIC FIBERS 1. Derived from PDL Derived from cementum. 2. Formed by fibroblast. Formed by cementoblast. 3. Run in same direction of the PDL principal fibers i.e. perpendicular or oblique to the root surface. Run parallel to the root surface and at right angles to the extrinsic fibers. 17/41
- 18. d) PRESENCE OF COLLAGEN FIBRILS FIBRILLAR CEMENTUM: Cementum with a matrix that contains well-defined fibrils of type I collagen. AFIBRILLAR CEMENTUM: Cementum that has a matrix devoid of detectable type I collagen fibrils. Instead, the matrix tends to have a fine, granular consistency. 18/41
- 19. e) SCHROEDER CLASSIFICATION (1986) 1. ACELLULAR AFIBRILLAR CEMENTUM (AAC): Consists of mineralized matrix. Contains neither cells nor fibers. Doesn’t have any function in tooth attachment. Formed by cementoblasts. Found in coronal cementum. Thickness : 1-15 µm. 2. ACELLULAR EXTRINSIC FIBER CEMENTUM (AEFC): Confined to coronal half of the root . Formed by fibroblast & cementoblasts. Thickness- 30-230 µm. Composed of densely packed bundles of sharpey’s fibers & lack cells. Only type of cementum seen in single rooted teeth. 19/41
- 20. 3. CELLULAR MIXED STRATIFIED CEMENTUM (CMSC): composed of extrinsic (sharpey’s ) & intrinsic fibers & contain cells. Co- product of fibroblasts & cementoblasts. appears in apical 3rd of roots, apices & furcation areas. Thickness- 100-1000 µm. 4. CELLULAR INTRINSIC FIBER CEMENTUM (CIFC): Contains cells & intrinsic collagen fibers. Formed by cementoblasts & fills the resorption lacunae. Very minor role in attachment. Seen in middle to apical 3rd & inter radicular cementum. 20/41
- 21. 5. HYALINE LAYER OF HOPEWELL-SMITH (INTERMEDIATE CEMENTUM) First layer of cementum is actually formed by the inner cells of the HERS and is deposited on the root’s surface. Deposition occurs before the HERS disintegrates. situated between the granular dentin layer of Tomes and the secondary cementum that is formed by the cementoblasts. 10 m thick. 21/41
- 22. CELLS OF CEMENTUM CEMENTOBLASTS CEMENTOCYTES CEMENTOCLASTS Originate from the ectomesenchymal cells in the dental follicle surrounding the developing tooth. Spider like cells incorporated into cellular cementum. Resemble osteoclasts. Synthesize collagen & protein polysaccharides. Lie in lacunae. Mononuclear cells, found on the surface of cementum. Have numerous mitochondria, a well- defined golgi apparatus & large amounts of granular endoplasmic reticulum. Cytoplasmic vol & density of cytoplasmic organelles is reduced when compared to cementoblasts. Role- Resorption & Repair. 22/41
- 24. CEMENTODENTINAL JUNCTION • The cementum is attached to the dentin firmly • CDJ is scalloped in deciduous teeth and is smooth in permanent teeth. • Sometimes cementum and dentin is separated by an intermediate layer. • Width appears to be stable even as age increases. • About 2-3 µm wide. 24/41
- 25. INCREMENTAL LINES OF CEMENTUM Referred to as “ Incremental lines of Salter”. Represent rhythmatic periodic deposition of cementum. Appear as dark lines running llel to root surface . Seen in both acellular & cellular cementum but more prominent in acellular cementum. Highly mineralised areas with less collagen & ground substance. 25/41
- 26. FUNCTIONS Attachment medium. Doesn't show resorption under masticatory or orthodontic forces. Forms seal. Repair. Maintenance of teeth. 26/41
- 27. CEMENTAL RESORPTION Permanent teeth don't undergo physiologic resorption as do primary teeth. Cementum resorption appears microscopically as bay like concavities in the root surface. The resorptive process may extend into the underlying dentin & even into the pulp, but is usually painless. Cementum resorption is not necessarily continuous & may alternate with periods of repair & deposition of new cementum. The newly formed cementum is demarcated from the root by a deep staining irregular line, termed as reversal line. LOCAL CONDITIONS trauma from occlusion Orthodontic movement Cysts Tumors pressure from malaligned erupting teeth. periapical disease periodontal disease. SYSTEMIC CONDITIONS Ca deficiency. Hypothyroidism. Paget’s disease. 27/41
- 28. REPAIR Process to heal the damage caused by resorption of cemental fracture. Requires the presence of viable connective tissue. ANATOMICAL FUNCTIONAL Generally occur when the degree of destruction is low. Occurs in cases of large cemental resorption or destruction. The root outline is re-establised as it was before cemental resorption. To maintain the width of periodontal ligament, the adjacent alveolar bone grows and takes the shape of defect following the root surface. This is done to improve the function of tooth 28/41
- 29. NORMAL FEATURES OF CEMENTUM Extensive variation in surface topography of cementum can be observed with scanning electron microscope (SEM). Resting cemental surfaces, where mineralization is more or less complete, exhibit low rounded projections k/as cemental mounts. Cemental surfaces with actively mineralizing fronts have numerous small openings. Represent unmineralized cores of openings. 29/41
- 30. CEMENTUM IN PERIODONTAL DISEASE Hurzeler & Zander: cementum apposition is less in periodontally involved teeth than in normal teeth. Cementum apposition decreases with advancing age in periodontally involved teeth. Gottlieb: areas of cemental resorption are frequently observed. 30/41
- 31. ROOT SURFACE WALL OF PERIODONTAL POCKET In normal cementum, the collagen fibers are embedded in the cementum. These fibers are destroyed in pathological pocket wall with the exposure of cementum. Collagen remnants of Sharpey’s fibers in cementum undergo degeneration creating a environment favorable for penetration of bacteria. The mineral content of exposed cementum increases. 31/41
- 32. CHANGES AFTER INSTRUMENTATION Firm scaling strokes used to remove sub gingival calculus, also remove a small amount of cementum resulting in some notching of root. NECROTIC CEMENTUM: Cementum exposed by apical migration of junctional epithelium is altered by exposure to sub gingival plaque within the pocket. May become hyper mineralized, demineralized or necrotic. 32/41
- 33. Lopez et al, 1980 necessary to remove all the diseased cementum exposed to the pocket to eliminate its potential for inducing inflammation. Nyman et al, 1986 intentional root cementum removal is not necessary for optimal postoperative healing. Removal of cementum during root planing process has been questioned due to possible sequelae of root sensitivity. Also, it is thought that cementum removal is not necessary to remove endotoxin because it is only weakly adherent to cementum. (Wilson & Kieser; 1988, Hughes & Smales, 1986, Smart, Wilson, Daves & Kieser, 1990) 33/41
- 34. AGE CHANGES IN CEMENTUM Smooth surface becomes irregular. Continuous deposition of cementum occurs with age in the apical area. Cementum resorption active for a period of time and then stops for cementum deposition creating - reversal lines. Resorption of root dentin occurs with aging which is covered by Cemental repair. 34/41
- 35. ANOMALIES IN CEMENTUM 1. CONCRESENCE Form of fusion which occurs after the root formation has been completed. Here the teeth are united by cementum only, as a result of traumatic injury or crowding of teeth with resumption of the interdental bone so that the two roots are in approximate contact and become fused by deposition of cementum between them. Concresence can occur before or after teeth have erupted and usually involves two teeth. 35/41
- 36. 2. CEMENTICLES Globular masses of cellular cementum less than 0.05mm in diameter which form within the periodontal ligament. May lie free within the periodontal ligament(free cementicles) or become fused to the radicular cemental surface(sessile or attached cementicles). Originate from degenerating cells or epithelial cell rests in the periodontal ligament. 36/41
- 37. 3.HYPERCEMENTOSIS (hyperplastic cementum) Abnormal thickening of cementum. May affect all teeth of the dentition, be confined to a single tooth or even effect only parts of one teeth. Localized hypercementosis may sometimes be observed in areas in which enamel drops have developed on the dentin. Such knob like projections are designated as excemetosis. The thickening of cementum is often observed on teeth that are not in function. 37/41
- 38. 4. ANKYLOSIS • Fusion of cementum and alveolar bone with obliteration of periodontal ligament • It occurs due to:- 1) Cemental resorption 2) Chronic periapical inflammation 3) Tooth replantation 4) Occlusal trauma 38/41
- 39. 5. CEMENTAL TEARS Detachment of a fragment of cementum from the root surface. Separation of cementum, may be complete with displacement of a fragment into the periodontal ligament or it may be incomplete with cementum fragment partially attached to the roots. Detached cementum, may be reunited to the root surface by new cementum or may be completely resorbed or may undergo partial resorption followed by addition of new layers. 39/41
- 40. CLINICAL CORRELATION Cellular cementum is similar to bone but has no nerves. Therefore it is non-sensitive to pain. Scaling produces no pain, but if cementum is removed, dentin is exposed causes sensitivity. Cementum is resistant to resorption especially in younger patients. Thus, orthodontic tooth movement causes alveolar bone resorption and not tooth root loss . 40/41
- 41. REFERENCES Carranza’s clinical periodontology 10th ed. Orbans oral histology and embryology. 12th edition. Listgarten 1st ed. International Journal of Scientific & Engineering Research, Volume 4, Issue 12, December-2013. The Cementum: Its Role In Periodontal Health and Disease: JOP, 1961. Dental cementum reviewed: development, structure, composition, regeneration and potential functions: Braz J Oral Sci. January/March 2005 - Vol.4 - Number 12. Development and general structure of the periodontium: Periodontology 2000, Vol. 24, 2000, 9–27. Cementum proteins: role in cementogenesis,biomineralization, periodontium formation and regeneration. Periodontology 2000, Vol. 67, 2015. 41/41
Hinweis der Redaktion
- Cementum formation occurs along the entire tooth. Hers- proliferation of ep cells located at the cervical loop of the enamel organ in the developing tooth
- Cementum consists of organic matter, inorg, and water. By vol, cementum contains 35% org materials, 45% inorg material & 20% water.
- 1.CONTAINS PROTEOGLYCANS. 2. because they are integral components of cell substraum attachment matrices and mediate attachment bw old and newly formed cementum. Because acellular cementum doesnot contains proteoglycans.3. because hers cells express this proteoglycans during root development 2..non collagenous proteins. Osteopontin is present within the pdl in mature teeth. Bone sialoprotein: bsp2 Phosphoglycoprotein containing up to 20% of sialic acid residues (Bilezikian et all 1996). Osteopontin: bsp1 1st identified in osteoblasts in 1986.
- Chemoattraction : unidirectional movement of a cell, in response to a chemical gradient of ligands…… alkaline phosphate:. Tissue non-specific alkaline phosphatase. Membrane bound glycoprotein enzyme. Expresses in most body sites during embryonic development but is confined to bone, kidney, liver & b- lymphocytes during adult lyf. Highly expresses in cells of pdl where they play role in phosphate metabolism n cementum formation particularly formatn of acellular cementum.
- 2.Mineralized tissues such as bone and dentin, are excellent reservoirs of growth factors. Cap: collagenous cementum derived protein , promote the adhesion and spreading of mesenchymal cell types, with osteoblasts & pdl fibroblasts showing better adhesion than gingival fibroblasts & keratinocytes. Cap play role in the cell selection process. Play regulatory role during cementum formation. Imp role in promoting the differentiation of putative cementoblast progenitors.
- osteonectin: Composed of a single polypeptide chain and has a strong affinity for calcium ions (Sage and Borstein, 1991) particularly strongly around the Sharpey’s fibers, at the attachment sites between the ligament, alveolar bone and the cementum…….. Osteocalcin: localised in cells lining cellular n acellular cementum. Also present in interradicular cells.
- The area where both extrinsic and intrinsic fibers is called mixed fiber cementum
- 1. Provides medium for attachment to the collagen fibers of the PDL. 2. Cementum is harder than alveolar bone & is avascular & doesn't show resorption under masticatory or orthodontic forces. 3. Covers the root surface, forms seal for open dentinal tubules. 4, Property of continuous deposition thus it repairs the damage such as fracture or resorption of root surface. 5. Aid in maintaining the teeth in functional occlusion if deposited at apical aspect especially in patients with chronic bruxism- passive eruption.
- CHANGES IN DISEASED CEMENTUM: Many Gram –ve bacteria have the ability to attach to Gram +ve bacteria in the cementum & epithelial cells (Slots & Genco, 1984).
- Minerals inc: ca, mg, p, f