Global Nomads Mobile Health Blueprint Paper
•
1 gefällt mir•1,102 views

Stanford University Mobile Health Without Borders Final Project Report Paper on Global Nomads Mobile Health Issues

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (10)
Andere mochten auch
Andere mochten auch (15)
Ähnlich wie Global Nomads Mobile Health Blueprint Paper
Ähnlich wie Global Nomads Mobile Health Blueprint Paper (20)
Mehr von Dr. Carsten Weerth BSc (University of Glasgow) LLM MA
Mehr von Dr. Carsten Weerth BSc (University of Glasgow) LLM MA (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Global Nomads Mobile Health Blueprint Paper
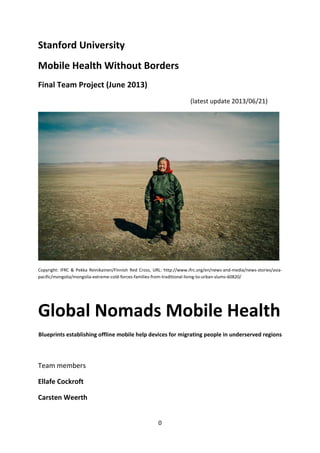
- 1. 0 Stanford University Mobile Health Without Borders Final Team Project (June 2013) (latest update 2014/10/29) Copyright: IFRC & Pekka Reinikainen/Finnish Red Cross, URL: http://www.ifrc.org/en/news-and-media/news-stories/asia-pacific/ mongolia/mongolia-extreme-cold-forces-families-from-traditional-living-to-urban-slums-60820/ Global Nomads Mobile Health Blueprints establishing offline mobile help devices for migrating people in underserved regions Team members Ellafe Cockroft Carsten Weerth
- 2. 1 Dedication This Global Nomads Mobile Health Project has been created on top of the shoulders of giants. It aims at pooling available information on mobile devices and apps available for offline help for nomadic people and their smart phones around the globe. We are strongly depending on the fabulous material which has been developed before. We are thankful for Stanford School of Medicine enabling a wider range of students and scholars to participate in the experience of further education by collaboration by help of inventive learning environments such as URL: http://www.venture-lab.org. We are in particular thankful to Dr. Eric Leroux and Prof. Dr. Homero Rivas. We would also like to thank the IFRC for the use of the picture of the nomad woman.
- 3. Abstract of the Global Nomads Mobile Health Project The Global Nomads Mobile Health Project aims at developing Mobile Health Devices that help pastoral nomads around the globe to enhance their information on health issues, nutrition, childbirth and overall chances for health care in underserved regions. These blueprints are investigating the problem, describing the current solutions, brainstorm possible mHealth solutions and present a business model for implementation. We suggest to pool available information in a Global Nomads Mobile Health Blueprint Paper. Furthermore we suggest to pool and create new helpful apps for smarts phones which are in use off-line. These apps should aim to help with nutrition, childbirth, newborn health issues, etc. They should be distributed by help of microSD-Cards. Since many nomads are illiterate we suggest establishing an icon or cartoon based smart phone app with much video content. 2 Keywords Apps, App, non-profit, nomads, UN, NGOs, mHealth, WHO, Smart Phones, Solar Panels, illiterate people, microSD-card, Millennium Development Goals, Energy Supply, Child Mortality, Education, Midwives, Mortality. The Online version of this Blueprints Paper is available under URL: http://globalnomadsmobilehealth.weebly.com/ This Global Nomads Mobile Health Blueprint Paper is available under URL: http://de.slideshare.net/Sternaugen/global-nomads-mobilehealthpaperblueprint
- 4. 3 Table of Contents Dedication Abstract Project Summary Prologue A. Choosen scenario 1. Economic and socio-cultural scenario 2. Nomadic lifeforms 3. Nomads, nomadic lifestyle and basic health issues 4. Who cares for nomads? 5. Millennium Development Goals B. Current approaches for nomadic people 1. Current problems 2. Possible mHealth approaches 3. Existing technology a. Energy supply b. Existing apps 4. Our solution C. Possible Business Models D. Project result E. Advice for a Local Approach F. Conclusion References About the authors and team members
- 5. 4 Project Summary The Global Nomads Mobile Health Project aims at developing Mobile Health Devices that help pastoral nomads around the globe to enhance their information on health issues, nutrition, childbirth and overall few chances for health care in underserved regions. These blueprints are investigating the problem, describing the current solutions, brainstorm possible mHealth solutions and present a business model for implementation. We are not inventing everything new. We are standing on the shoulders of giants and building on top of their outstanding work and performance. We are trying to pool important and useful data so that it is easily available and usable for nomadic communities.
- 6. 5 Prologue The topic of this Global Nomads Mobile Health Project came into our mind after reading the story in the February 2013 issue of National Geographic Magazine (Finkel, 2013). It covers the story of the Kyrgyz nomads in Northern Afghanistan. Child mortality is very high and the health status for mothers and young children is rather bad. However smart phones are in use (off grid) and solar power is available so these devices could be used in order to make the health burden lighter. Finkel reports about a couple that had 11 children out of which 10 died and only one made it to the age of five. Then it also passed away (Finkel, 2013, p. 93/94). The childhood mortality is tremendously high. They are living in the so called Wakhan Corridor of Northern Afghanistan which lies between Tajikistan and Pakistan. They are making a living about 4,700 m (14,000 feet) above the sea… There are no roads, there is no hospital, there is no doctor, and there is no government to help… The education level is only basic: the 1,100 population has only a rudimentary education however they are using smart cell phones [smart phones] for listening to music and taking pictures (Finkel, 2013, p. 94). Their leader (a Khan) is aged 32 and has never learned to read or write (FInkel, 2013, p. 94). The basic currency of their people is a sheep – one cell phone costs one sheep, a yak costs about 10 sheep, a high-quality horse 50 sheep and a bride is about 100 sheep (Finkel, 2013, p. 95). Community health workers are an apt and good instrument promoted by the WHO, but these are not working with this nomadic people. The basic primary care as was postulated by the Alma Ata Declaration of the WHO (WHO, 1979) is not in place with many pastoral nomadic people in Africa or Central Asia… The Millennium Development Goals (UN, 2000 and WHO, 2000) will not be met if these nomadic populations will receive basic primary health care… One of the problems is the high rate of illiteracy under these nomads. So it was an unique option for this Stanford School of Medicine class to pick this situation and crate a Mobile Health solution for a problem that is widespread two years before the Millennium Development Goals are hitting their deadline…
- 7. 6 A.Choosen scenario 1. Economic and socio-cultural scenario Health is of basic importance for the success of individuals, families, clans and tribes and societies as a whole. When nutrition or clean water is not sufficient, the humans suffer. Women are malnourished, the death rate of childbearing women is high and the rate of child death is even higher. Without proper health care many parts of the society are very much affected: the individuals, families, clans and tribes but also employers, the community and the state itself. When basic infrastructure is lacking (no roads, no hospital or doctors) life is harsh and humans are carving a life from earth – the main goal is survival. Such societies are interested in clean water, proper nutrition, and save harvests. A higher wealth, roads and development, continuous health care, emerging economies and incentives are high aims for the least developed societies as well as social rest and peace. When conflicts arise over the simple ingredients of life, civil unrest and war are abundant… Mobile Health might help to ease the demand for simple help in underserved regions. When mobile smart phones are in use and the required (solar) power is provided, simple apps can help to give advice in questions of sanitation, first aid and child birth. The mHealth app should be easy and straightforward, preferably easy to use and understand, possibly without language for illiterate people. 2. Nomadic life forms Nomadic people are living in all continents, however they are differing in hunter-gatherers and pastoral nomads (Anon., 1995), see picture 1. This project is mostly concerned with the pastoral nomads in central Asia and also a little bit with the nomads in central and eastern Africa. A general description of the pastoral nomadic life form is available (Yanjisurin, 2012).
- 8. Picture 1: The distribution of nomadic people around the globe 7 Picture from Anon., NewIntJ, 1995 3. Nomads, nomadic lifestyle and basic health issues The Word Nomad derives from Greek word for ‘pasture’: nomos (Anon, NewIntJ, 1995). These pastoral nomads move with their households in search of pasture for their animals. In the mid 1990ies there were an estimated 30-40 million of them in the world (Anon, NewIntJ, 1995). Livestock in these tribes is central to their livelihood and the basis of their culture. Their movement is seasonal, linked to rainfall and the availability of good forage for their animals (Anon, NewIntJ, 1995). Picture from Anon., NewIntJ, 1995 Statistical data is available for the nomads of Mongolia (Open Society Forum, 2004, p. 9): “Statistical data show that herders lack opportunities for accessing education and health care services. According to 2000-2002 data, maternal mortality in rural areas is double that of urban areas, infant mortality is 46% higher, and the mortality rate of children of under-5’s
- 9. is 39% greater. In the majority of soums and bags children’s foreign language knowledge and computer literacy level is extremely poor, there is a lack of teaching staff, and more than 40% of the total of 329 soums do not have a link to the central electrical grid. The issue of eliminating the existing backlog of education and health care services problems is still unresolved.“ 8 4. Who cares for nomads? Nomads are often migrating over borders. The governments of the countries should care for the nomads but they are often not caring. Nomads are not residents and therefore it often is difficult to enforce laws or collect taxes. Hospitals are not available and normal approaches adopted by the WHO – such as community health workers regularly visiting the people – are not applicable because of the migrations. Possible stakeholders for nomads health promotion are the governments but also official international organizations such as WHO, UNO, UNICEF, FAO or NGOs such as LIFE-Net (Local Livestock for Empowerment of Rural People) or physicians without borders. 5. Millennium Development Goals The United Nations announced Millennium Development Goals in 2000 which were aiming at eight targets by 2015 (WHO, 2000 and UN, 2000): 1. Eradicate extreme poverty and hunger 2. Achieve universal primary education 3. Promote Gender equality and empower women 4. Reduce Child Mortality 5. Improve Maternal Health 6. Combant HIV/Aids, Malaria and other diseases 7. Ensure environmental sustainability 8. Gobal Partnership for Development These goals should also be reachable for nomadic people. Our project covers the MDG No. 2, 3, 4, 5 and in Africa also No. 6.
- 10. 9 B. Current approaches for nomadic people 1. Current problems Current problems are: - Access to primary health services, - High childhood mortality, - Basic education levels (if at all), - Illiteracy, - Malnutrition of mothers, - Malnutrition of newborn infants, - Lacking knowledge of basic medical help in special situations, - Lacking help for easily diagnosed medical problems, - No community health workers, - No safe and continuous clean water supply. Needs of Pastoralist Nomads: Daily life is devoted to caring after their livestock – watching over, milking, shearing or combing animals. Health issues include 1. Education and Behavior change. Nomads neglect their health and consider livestock and animal breeding more important. 2. Health services in provinces of poor quality. Shortage of educated doctors in the province. The ratio of patients is very high compared to the number of available doctors. Furthermore, hospitals and health centers do not have modern medical equipment. One example for what is done now for nomadic children in Uganda: Orphanage for children http://www.theuapo.org/downloads/Spring_2007_Newsletter.pdf The nomads are coping somehow but the death rates are high. Nomadic people have their own approaches to medicine such as the traditional Mongolian medicine which was created thousands of years ago. Some governments are trying to settle nomadic people permanently such as the Mongolian nomads in China (Myadar, 2009 and IFRC, 2013).
- 11. 10 What do these nomads need? Education, knowledge, self-care ability, medicine – Our solution: a stand-alone mHealth device on their smart phone. 2. Possible mHealth approaches Nomads are using mobile phones for their leisure (Finkel, 2013). They could be provided with mobile cartoon apps which educate the user for emergency cases (first aid), educate for breastfeeding or deliver short videos for whatever topic. Theses apps could be distributed on microSD-cards by governments, international organizations or NGOs for free and stand-alone use. 3. Existing technology a. Energy supply Energy supply for mobile devices is available and in widespread use, e.g. with the Kyrgyz nomads in Northern Afghanistan (Finkel, 2013). Many different companies are offering solar panels for charging mobile phones (see Google search: Google Pictures “Solar panel mobile phones”). b. Existing apps Many useful apps exist already such as first aid apps, apps about health information issues, videos on nutrition and malnutrition, videos for breastfeeding. 4. Our solution Existing apps for smart phones could be pooled on microSD-cards. Desirable is the creation of a cartoon-based new app that is tailored to the needs and requirements of nomadic people. Due to its cartoon-basis it can be applied in many countries (in Central Asia or Africa).
- 12. C. Possible Business Models 1. Freemium: One way would be a mix of free and paid content. 2. CrowdSource Business Model: Have product or service and crowd partners fund the first 11 prototypes. 3. Non-profit Business Model: governments, public funds or NGOs are going to fund the project. Non-profit Business Model: non-profits can map out 2 business models, the Donor Model or the Beneficiary Model. 1. Donor Model canvas is a donor-oriented value proposition on the revenue side. Even though Donors do not receive the products or services that nonprofits offer, donor groups of people have needs and wants, even if what is received is a positive feeling of accom-plishment. It is a win-win situation and an exchange occurs when the nonprofits with value-propositions matches with the right donor segment. 2. Beneficiary Model is created to fill a social mission that cannot be fulfilled by for-profit organizations. The value added to society needs to be unique or done more efficiently than that of the for-profit world, or else would compete for income in a market where products or services to those that are giving money cannot be provided, while competitors provide them and fill a social mission. The value proposition can be called a "Mission Offering" relevant to the Global Nomadic beneficiary segments. Each beneficiary segment is identified for each segment to work with either 1 or 2 non-profit models: 1. Distribution Channels interaction with beneficiaries. 2. Beneficiary Relationships type and level of relationships 3. Impact Metrics quantifiable measures of impact to beneficiary-oriented value; 4. Key Resources essential assets needed to create beneficiary-oriented value. 5. Key Activities create and capture beneficiary-oriented value i.e. impact; 6. Key Partners network leverage Beneficiary Model with added connections, resources or activities. These may be specific donors, but in general they are people or organizations needed to acquire and/or create value for beneficiaries. 7. Cost Structure costs essential to creating value for beneficiaries. The two sides of the Nonprofit Business Model Canvas are not mutually exclusive. Resources on the donor side may have to be shared with the beneficiary side and vice-versa. They form under one organization, but they have two different focuses: value for revenue or value for impact. We opt for a beneficiary non-profit business model since the governments, international organizations or NGOs should be in charge of delivering mobile health to nomadic people. Possible stakeholders and donors will be approached after the deadline for this project – 2013/06/23.
- 13. 12 D. Project result The Global Nomads Mobile Health Project results in a blueprint paper that is downloadable for further project work for free in the internet and a free website which consists of the same content online. For the blueprints see URL: http://de.slideshare.net/Sternaugen/global-nomads-mobile-healthpaperblueprint For the webpage see URL: www.globalnomadsmobilehealth.weebly.com E. Advice for a Local Approach Set up a local process that is suitable, sustainable and tailored to the needs, demands and resources of the nomadic community in question: Setting up local nomads mobile health guidelines based on this Global Nomads Mobile Health Blueprint paper. Performing a local approach: Survey the area Preassessment Research what health issues are there and weather there are systematic solutions in place. Are doctors available? Are community health workers serving the people? Find out what the nomadic people already know. Identify key community leaders. Identify the mobile and energy sources available. Our solution: Existing apps for smart phones could be pooled on microSD-cards. Desirable is the creation of a cartoon-based new app that is tailored to the needs and requirements of nomadic people. Due to its cartoon-basis it can be applied in many countries (in Central Asia or Africa). It should also contain many video sequences. It should be distributed by help of microSD-Cards.
- 14. 13 F. Conclusion About the use of theses Global Nomads Mobile Health Blueprints: - Make this information available to your community. Either directly in English, or translate it when adequate. - Make sure your nomadic community, your people and their children are aware of their health issues and the way smart phones can help in these issues. - Stakeholders should pool available apps on microSD-cards. - Apps should preferably be cartoon-based and video based so that illiterate people can understand the message. - When necessary apps e.g. for childbirth, midwives, sanitation, etc. are not available, stakeholders should ensure the creation of such easy-to-use apps for free. - Stakeholders should try to deliver and distribute the necessary apps on microSD-cards. - Desirable is the creation of a cartoon-based new app that is tailored to the needs and requirements of nomadic people. Due to its cartoon-basis it can be applied in many countries (in Central Asia or Africa). Possible stakeholders for global nomads health promotion are the governments but also official international organizations such as WHO, UNO, UNICEF, FAO or NGOs such as LIFE-Net (Local Livestock for Empowerment of Rural People), the International Federation of Red Cross and Red Crescent Societies or doctors without borders but also scientific organizations such as UNESCO or National Geographic Society.
- 15. 14 References Anonymus, 1995. Nomads – the Facts, The New International Magazine, Issue 266, April 1995, URL: http://newint.org/features/1995/04/05/facts/ Beall, C. and Goldstein, M., 1993. Past becoming future for Mongolian nomads National Geographic Magazine, May 1993. Bold, S. Brief History and Development of Traditional Mongolian Medicine, URL: http://- www.wipo.int/edocs/mdocs/tk/en/wipo_iptk_bkk_09/wipo_iptk_bkk_09_topic6_1.pdf Finkel, Michael, 2013. Stranded on the Roof of the World, National Geographic Magazine, February 2013, pp. 84-111, URL: http://ngm.nationalgeographic.com/2013/02/wakhan-corridor/ finkel-text Goldstein, M. and Beall, C., The Remote World of Tibet’s Nomads, URL: http://www.cwru.edu/affil/tibet/booksAndPapers/Remote%20World%20of%20Tibet%27s% 20Nomads.html Goldstein, M. C. and Beall, C. M., 2002. Changing patterns of Tibetan nomadic pastoralism. In: Human Biology of Pastoral Populations, Leonard and Crawford (eds.). Cambridge University Press, 131-150. International Federation of Red Cross and Red Crescent Societies, 2013. URL: http://www.ifrc.org/en/news-and-media/news-stories/asia-pacific/mongolia/mongolia-extreme- cold-forces-families-from-traditional-living-to-urban-slums-60820/ Kradin, N., N. 2004. Nomadic Empires in Evolutionary Perspective. In Alternatives of Social Evolution. Ed. by N.N. Kradin, A.V. Korotayev, D. Bondarenko, V. de Munck, and P.K. Wason (p. 274-288). Vladivostok: Far Eastern Branch of the Russian Academy of Sciences; reprinted in: The Early State, its Alternatives and Analogues. Ed. by L. Grinin et al. (р. 501-524). Volgograd: Uchitel', 2004. Kradin, N. N., 2002. Nomadism, Evolution, and World-Systems: Pastoral Societies in Theories of Historical Development. Journal of World-System Research 8: 368-388.
- 16. Kradin, N. N. 2003. Nomadic Empires: Origins, Rise, Decline. Nomadic Pathways in Social Evolution. Ed. by N.N. Kradin, Dmitri Bondarenko, and T. Barfield (p. 73-87). Moscow: Center for Civilizational Studies, Russian Academy of Sciences. Kradin, N. N. 2006. Cultural Complexity of Pastoral Nomads. World Cultures 15: 171-189. Leder, S., 2005. Nomadic and Settled People in Steppe Landscapes and within Statehood, Scientia Halensis 1/05, p. 19-22, URL: http://www.nomadsed.de/en/nomaden-sesshafte/- 15 introduction/ Leonard, W. R. and Crawford, M. H. (Eds.), 2002. Human Biology of Pastoral Populations. Cambridge University Press. Myadar, O., 2009. Nomads in a Fenced Land: Land Reform in Post-Socialist Mongolia, Asian- Pacific Law & Policy Journal, 11(1), pp. 161-201. Open Society Forum, 2004. The Future of Nomadic Pastoralism in Mongolia, URL: http://www.forum.mn/res_mat/Book-english.pdf UN, 2000. Millennium Development Goals, URL: http://www.un.org/millenniumgoals/ Vigo, J., 2005. 'Nomadic Sexualities and Nationalities: Postcolonial Performative Words and Visual Texts'. Inscriptions in the Sand Famagusta: Eastern Mediterranean University Press, 2005. Wikipedia, 2013, URL: https://en.wikipedia.org/wiki/Nomad WHO, 1978. Alma-Ata Declaration on Primary Care, International Conference on Primary Health Care, Alma-Ata, USSR, 6-12 September 1978. WHO, 2000. Millennium Development Goals, URL: http://www.who.int/topics/millennium_- development_goals/en/ Yanjisurin, G., 2012. The Last Nomads, Red Rocks Community College, URL: http://www.rrcc.edu/claro/pdfs/2011-2012/thelastnomadsFINAL.pdf
- 17. 16 About the authors and team members Ellafe Cockroft, BS, PhD Ellafe A. Kiamco was born and raised in Silliman University Philippines. After receiving a B.S. in chemistry, awarded a teaching assistantship to pursue graduate studies in chemistry at the University of Missouri-Kansas City where she received her PhD. Furthermore received an United Board for Higher Education in Asia scholarship. She presented her dissertation "Polymeric Liquid Crystals" at International Liquid Crystal Conference in Stockholm Sweden. She worked in the semiconductor industry in Silicon Valley, involved in technology transfers and consulting in Taiwan and Singapore for LCD devices and modules for aircraft applica-tions. Married with children working in biomedical engineering industry in the San Francisco Bay Area and computer science in Tampa, Florida. Currently Adjunct Chemistry Professor of Broward College teaching online and face to face courses. Her motivation for mHealth and Stanford's MOOC courses comes from the desire to inspire Sustainable Living in the "smart poor" third world countries. Her father who was the first Fulbright Scholar at Silliman University once told her that "Education is the best legacy" and that we can help create a sustainable future through education. By creating awareness and a real understanding of people’s habits through education can rewards be realized. Dr. Carsten Weerth, BSc, LLM (Com), MA, FLS, FZS, FRGS Carsten Weerth was born and raised in Bremen/Germany. He received a B.Sc. in cellular and molecular Biology from the University of Glasgow and went on to do studies in Economics and Law: PhD from the University of Oldenburg and LLM (Com) from the Universität des Saarlandes and a MA in Adult Teaching from the Technical University Kaiserslautern. He has been teaching Law and Economics at three different Universities including Jacobs University in Bremen. He is author of more than 10 books and has published more than 100 papers. His motivation for doing Stanford MOOCs are the various collaborations with scholars from all over the globe in order to tackle interesting and important topics. For Designing a New Learning Environment he created the TOP Tsunami Online Portal (tsunamionlineportal.- weebly.com) with his team and has currently done about 120 MOOCs in topics ranging from Astrobiology and Global Health to Vaccines at Universities from Brown over Caltech and MIT to the University of Edinburgh, Duke, Emory, Penn, Wesleyan, Harvard and Stanford. In 2014 he has been elected Fellow of the Linnean Society of London (FLS), Fellow of the Zoological Society of London (FZS) and Fellow of the Royal Geographical Society (FRGS). Currently he is working in Germany’s public service.