NEUROSURGICAL TENETS OF PITUITARY GLAND
•Als PPTX, PDF herunterladen•
12 gefällt mir•3,152 views

Pituitary tumor accounts for ~10% ICT. They are common in 3-4 decade and shows association with MEN I. About 5% of PT are invasive usually with giant tumor (>4cm). Tumor can be classified as functional (hormone secreting) or non functional. This slides details the algorithmic approach in management of pituitary tumors.

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie NEUROSURGICAL TENETS OF PITUITARY GLAND
Ähnlich wie NEUROSURGICAL TENETS OF PITUITARY GLAND (20)
Mehr von suresh Bishokarma
Mehr von suresh Bishokarma (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
NEUROSURGICAL TENETS OF PITUITARY GLAND
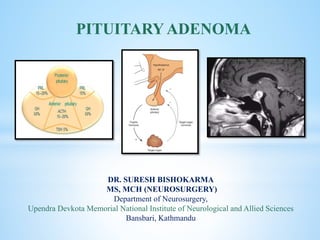
- 1. cka DR. SURESH BISHOKARMA MS, MCH (NEUROSURGERY) Department of Neurosurgery, Upendra Devkota Memorial National Institute of Neurological and Allied Sciences Bansbari, Kathmandu PITUITARY ADENOMA
- 2. Hermann Schloffer performed the first transsphenoidal resection of a pituitary tumor in 1907. Harvey Cushing popularized it in the two decades afterward. HISTORY
- 3. Two lobes: Adenohyophysis and Neurohypophysis. Normal AP diameter of pituitary gland: female of childbearing age (≈ 13–35 yrs): ≤11 mm, for all others normal is ≤9 mm. (Note: pituitary glands in adolescent girls may be physiologically enlarged (mean height: 8.2 ± 1.4 mm) as a result of hormonal stimulation of puberty. Anterior can be divided into the pars tuberalis (pars glandularis) and pars distalis (pars glandularis) that constitutes ~80% of the gland. The pars intermedia (the intermediate lobe) lies between the pars distalis and the pars tuberalis. Posterior lobe is connected to hypothalamus by stalk via median eminence and has high signal on T1WI (phospholipids). Absence of this “bright spot” often correlates with diabetes insipidus as may occur with autoimmune hypophysitis. INTRODUCTION
- 4. Development: 4th week: Primitive stomodeum and Neuroepithelium of hypothalamus toward sella. Vascular anatomy: Arterial supply: Ant. pituitary is supplied by superior hypophyseal artery. Post pituitary by SHA, IHA and infundibular artery. Capsule: McConnel (C4 branch) Portal venous plexus around the hypothalamopituitary complex for route of hormonal influence by hypothalamus Venous drainage by inferior hypophyseal vein. DEVELOPMENT AND VASCULARITY
- 5. Anterior pituitary (5 cells=6 hormone also folliculostellate (FS) cells). Posterior pituitary (2H) MSH is synthesized in AP and stored by intermediate lobe (aka intermedin). TSH producing tumor can itself elevate prolactin. Hormones in posterior pituitary is secreted in magnocellular neurosecretory cells of supraoptic and paraventricular nucleus of hypothalamus and carried via stalk along the infundibulum to store in PP ready to release TYPES OF CELLS IN ANTERIOR PITUITARY
- 6. Cellular Composition of gland
- 7. CLASSIFYING PITUITARY TUMOR Most common pituitary tumor is non-functional tumors
- 8. Accounts for ~10% ICT. 3-4 decade, MEN I. About 5% of PT are invasive. Giant >4cm. Epidemiology
- 9. 1. HORMONAL SYMPTOMS 2. MASS EFFECT 3. APOPLEXY 4. INCIDENTAL 1. Hormonal symptoms: Hypersecretion or hyposecretion. 68% of adenoma secrets hormones (Prl (48%)> GH (10%), ACTH (10%), TSH(1%). Underproduction: Mass effect by non functioning or functioning tumor (GH>Gonadotropins> TSH> ACTH). Chronic pan-hypopituitarism: Simmond’s cachexia 2. Mass effect: Chiasm: Bitemporal Hemianopia, decreased VA): Compression on the inferonasal fibers that decussate at the anterior and inferior aspect of the chiasm leads to superior temporal quadrantanopia, then bitemporal hemianopia. 3rd vent (HCP), Cavernous Sinus (CNs III-V2-3, VI palsy), Diplopia, proptosis, facial pain, Miosis. CSF rhinorrhea (Invasive) Hypothalamic involvement may produce: hypotension, thermal dysautoregulation, cardiac dysrhythmias, Respiratory pattern disturbances, Diabetes insipidus, altered mental status: lethargy, stupor or coma 3. Headache (raised intra sellar Pressure: diaphragm stretch, Hypothalmic encroachment (cluster) and ICP) CLINICAL PRESENTATION
- 10. MODIFIED HARDY’S CLASSIFICATION EXTENSION SYMMETRICAL Grade A: Suprasellar cistern only; Grade B: Recess of the third ventricle Grade C: Whole anterior third ventricle ASYMMETRICAL Grade D: Intracranial extradural Grade E: Extracranial extradural -Beneath cavernous sinus INVASION / SPREAD Floor of sella intact I: Sella normal or focally expanded; tumor ≤ 10mm II: Sella enlarged; tumor ≥ 10mm SPHENOID EXTENSION III: Localized perforation of sellar floor: IV :Diffuse destruction of sellar floor: DISTANT SPREAD V: Spread via CSF or blood-borne Anterior recess Displaced 3rd ventSuprasellar expansion Intradural extension Beneath cavernous (extradural extension)
- 11. A coronal view of cavernous sinus and adjacent structures. Three lines pass through supra and intracavernous parts of internal carotid artery (ICA): Medial line : connects the medial wall of ICAs Median line : crosses across the centers of ICAs Lateral line : touches the lateral wall of ICAs Grade 0 : Adenoma does not extend the medial carotid line Grade 1 : Adenoma crosses the medial line, but doesn't extend past the median line, or so-called "intercarotid" line Grade 2 : Tumor extends beyond the median line, but doesn't extend beyond the lateral line Grade 3 :Tumor extends beyond the lateral line Grade 4 : Tumor totally wraps around the intracavernous carotid artery CAVERNOUS INVOLVEMENT BY PITUITARY MACROADENOMA Micko et al (2015). Subdivided grade 3 into: 3A - the tumor extends to the lateral line superiorly (over ICA) 3B - the tumor extends to the lateral line inferiorly (under ICA) KNOSP CLASS
- 12. KNOSP’S CLASS OF CAVERNOUS INVASION
- 13. Microadenoma: <1cm diameter. 50% of pituitary tumors are <5mm at time of diagnosis. These may be difficult to find at the time of surgery. Macroadenomas: Tumors >1 cm diameter Giant adenoma: >4cm: Usually invasive. CLASSIFICATION: SIZE
- 14. HORMONE SECRETION AND FEEDBACK LOOP The level of end product maintains the negative feedback, except for the somatotrophs, where GHRH promotes GH release while somatostatin inhibits.
- 15. Adenoma of Lactotroph cells. Prolactin: Normal: Male: 2-18ng/ml, Female: 2-29 (pregnant (10-1=210ng/ml). Presentation: 50% of primary amenorrhoea, Amenorrhoea-galactorrhoea syndrome (Forbes-Albright). Prolactinoma: PRL> 200ng/ml Prolactinemia <200mg/ml: Physiological: stress, exercise, pregnancy, lactation, Stalk effect,infiltrating hypothalamic lesion, Drugs (Metoclopromide, estrogen, TCA, Ranitidine), Empty sella, post ictal, CRF, Cirrhosis. Prl >1000ng/ml (false low in giants adenoma due to hook effect on Radioimmunoassay). If >500ng/ml: surgery may address hyperprolactinoma, RCC, HCC, lymphoma, Algorithm: >500ng/ml start medical treatment then surgery once Prl is <500. Prolactin treatment for >1 year will render only 50% success rate of surgery due to fibrosis. PROLACTINOMA
- 16. Extremely high PRL levels may overwhelm the assay (the large numbers of PRL molecules prevent the formation of the necessary PRL-antibody-signal complexes for radioimmunoassay) and produce falsely low results. Have the lab perform several dilutions of the serum sample and re-run the PRL, especially in patients with clinical hyperprolactinemia Macroprolactinemia A situation where prolactin molecules polymerize and bind to immunoglobulins. Prolactin in this form has reduced biologically activity but produces a laboratory finding of hyperprolactinemia. HOOK EFFECT It will saturate the antibodies and fail to form the antibody sandwich complexes that are required for most radioimmunoassay. Excess hormone will be washed away with the labeled antibody, and the test result will be falsely low. These samples should be diluted to provide a more accurate PRL level.
- 17. Cushing diseases: Hypersecretion of ACTH. 50% have <5mm tumor. Lab: High serum cortisol and urinary cortisol or 17 hydroxycorticosteroid, Normal or elevated ACTH, Hypokalemic alkalosis, loss of diurnal variation, failure to suppression on low (1mg) dose dexamethasone, Low CRH. Acromegaly: Bony hypertrophy, Colonic polyposis, Cardiomegaly, DM, Multiple cranial nerve palsy, Carpel TS, GH, IGF-I. Medication: Octreotide, Pegvosement, bromocriptine, cabergoline, Pergolide. CUSHING’S DISEASE
- 18. Patients with a pituitary mass should undergo a complete neurologic and endocrinologic evaluation including a detailed history and physical examination to assess for signs or symptoms of hyper-secretory syndromes such as Cushing disease, hyper- prolactinemia, or acromegaly. Endocrinological testing is needed to determine hormonal function. Prolactin, FSH, LH, GH, insulin-like growth factor 1 (IGF-1), ACTH, cortisol, TSH, thyroxine, estradiol, and testosterone. Plain radiographs (cone down lateral view x ray): enlarged, round sella. and the sellar floor anatomy, pneumatisation of air sinus. High-resolution magnetic resonance imaging (MRI) with cuts through the sellar region is essential for surgical planning, as it will show the precise size and location of the lesion as well as its relationship with the chiasm, cavernous sinus, and other surrounding structures. 75% are low signal on T1WI, and high signal on T2WI (but 25%can behave in any way, including completely opposite to above). Enhancement is very time-dependent. if you are hunting for a microadenoma, then a dynamic MRI increases the chances that you might catch the tumor at a time when it enhances differentially from the gland. Imaging must be done with 5 minutes of contrast administration to see a discrete microadenoma. Initially, gadolinium enhances the normal pituitary (no blood brain barrier) but not the pituitary tumor. After ≈ 30 minutes, the tumor enhances about the same Dynamic MRI scans have been used to increase the sensitivity (contrast is injected while the MRI scanner is running). CT SCAN: Direct coronal or coronoal reconstruction thin cut axial computed tomography (CT): sphenoid sinus anatomy: Types: Sellar, Presellar, post sellar and conchal type (less pneumatised). Cerebral angiography to demonstrate parasellar carotid arteries and to R/O aneurysm as a possibility (if MRA not done/contraindicated); also assesses the ICA encasement. Calcium in pituitary usually signifies hemorrhage or infarction within tumor. Ophthalmological evaluation and Visual field charting (Perimetry) Nasal swab as a pre-operative antiseptic workup. WORK-UP
- 19. WORK UPA CASE OF ACROMEGALY SINGLE RANDOM BASAL GROWTH HORMONE LEVEL <5ng/ml >10ng/ml Normal Acromegaly Single random basal may not be reliable; pulsatile secretion pattern Sporadic peak >50ng/ml and as low as 37pg/ml: cant be used as diagnostic tool Oral Glucose suppression test measurement at 0,30,60,90,120 min after 75mg oral glucose load GH nadir: <1ng/ml GH nadir: >1ng/ml Also high in Liver diseases uncontrolled DM CRF Pituitary tumor: GHRH (+) RESPONSE Ectopic GH secreting tumor GHRH (-) RESPONSE IMAGING Acromegaly proven SPECT: Octreotide scan with 6.5mCi of Indium111 : scan after 4 & 24 hr: Hot spots 1. IGF-1 (Somatomedin-C) level: RECOMMENDED Excellent integrative marker of average GH secretion: Extremely sensitive for acromegaly. 1. Growth-hormone releasing hormone (GHRH) levels: Differentiate: pituitary cause V/S ectopic acromegaly . Oral glucose suppression test (OGST): less precise and more expensive than measuring IGF-1: useful than IGF-1 for monitoring initial response to therapy. Ruled out Stringent criteria for a cure or remission of acromegaly require: • Random GH less than 2.5 ng/ml, or • GH nadir after an oral glucose tolerance test of less than 1 ng/ml and • A normal age and gender- normalized IGF-1, with no clinical symptoms.
- 20. Primary work up to rule out Small cell lung ca, Pancreatic ca, pheochromocytoma, Medullary thyroid ca and thymoma. WORK UPA CASE OF CUSHING SYNDROME Not suppressed Suppressed in normal individuals 24hr urine 17-OHCS: <4mg/24hr Low dose (1mg) Dexamethasone suppression test or 2 day low dose test (0.5mg q 6hr ACTH independent ACTH Dependent High dose 8mg CRH or AVP Metyrapone Not suppressed ACTH unchanged ACTH unchanged Suppressed ACTH increased ACTH increasesd Serum Cortisol: <140 nmol/L Urinary free cortisol: <50 nmol/L Urinary 17-hydroxy cortiosteroid: <6.9 nmol/L 1. Assess the cortisol production in 24 hours in serum and urine ( Normal 24hr serum cortisol: 20-90ug/ml, Urinary 17-OHCS: >150ug/ml), cortisol < 1.8ug/dl: cushing is ruled out. Cortisol> 10 ug/dl: CS is probably present. 2. Assess sensitivity of HPA axis to negative feedback by glucocorticoids. 3. Assess ACTH dependency: • ACTH dependency diseases: Excess ACTH >>> Excess cortisol; • ACTH independent diseases: Excess cortisol, Low ACTH, HPA suppressed. 4. CRH and AVP are secretagogue and causes increased secretion of ACTH. 5. Metyrapone are cortisol synthesis inhibitors: Increased cortisol or urinary 17-OHCS. 6. If imaging is not conclusive of microadenoma: then adopt Inferior petrosal sinus sampling/ Cavernous venous sampling (more accurate but highly morbid than IPSS). Bilateral femoral catheter B/L IJV IPS; Simultaneous ACTH measurement after CRH stimulation. IPS: Peripheral ACTH: 2:1 (95% S; 100% S); 3:1: ( both 100%), Inter sinus gradient (>1.4) lateralize the lesion in 75%cases. Measure prolactin level too
- 21. 1. Rathke cleft cyst may appear similar to a cystic pituitary adenoma. 2. Tuberculum sellae meningioma may compress the chiasm: No enlargement of the sella. 3. Craniopharyngioma is more often a suprasellar lesion. 4. Metastasis to the sella: diabetes insipidus or extraocular muscle palsies 5. Internal carotid artery aneurysm may fill the sella: a flow void T2W MRI. 6. Sarcoid granuloma or tuberculoma: rare. Differentials
- 22. Medical Surgical Radiotherapy TREATMENT
- 24. Dopamine agonists (DA) unless there is unstable deficit. Debulk the tumor transsphenoidally and then rechallenge with DA therapy. For unstable deficit Non-responders PROLACTINOMAS Drug Dose Complication Remarks Bromocriptine semi-synthetic ergot alkaloid D1 & D2 agonist 1.25mg (PO/Vaginal) Adjust: 2-4wks for micro; 3-4 days for macroadenoma Check initial PRl level at 4 weeks. To shrink tumor: 7.5mg in 3 div dose x 6 months Reduces PRl level to <10% of pre- treatment values in most patients. Reduces size in 6-8wks in 75% patients GI symptoms, orthostatic hypotension, vasodilation,nasal congestion, psychiatry (depression), nightmare Shrinks and increases risk of CSF leak. Prolonged treatment with bromocriptine may reduce the chances of surgical cure by 50% if >1yr Pregnancy: 3.3%:congenital anomalies 11%: Spontaneous abortion rate = Normal population Cabergoline ergot alkaline derivative D2 agonist 0.25 mg PO twice weekly; increase by 0.25mg q 4 weeks (max 3mg/week); T1/2 60-100hrs Check initial PRl at 4 weeks Less than bromocriptine, can be given in pregnancy, Cardiovascular complication in high dose (10X dose in parkinsonism): Valvular heart diseases- Regurgitation due to valve fibrosis.( activates 5-HT2 B receptors which induces prolonged mitogenic effects in fibromyoblasts, which may lead to valvular fibroplasia Control of PRLand resumption of ovulatory cycles may be better than with bromocriptine. Contraindicated in eclampsia or pre-eclampsia, uncontrolled HTN
- 25. Long-term therapy with DA agonists has some cytocidal effect on pituitary tissue. 24 months therapy was associated with >95% recurrence rate Recent literature suggests a 20–30%chance of normoprolactinemia off medication in select patients. When to stop: Recommendations: If response to DA agonist is satisfactory, treat for 1–4 years (microadenomas: check prolactin yearly, macroadenomas are more likely to grow and should be checked more often). Microadenomas or macroadenomas that are no longer visible on MRI are candidates for DA agonist withdrawal. For microadenomas: discontinue the drug; For macroadenomas: slowly taper the drug then discontinue. Recurrence rate is highest during 1st year, check prolactin levels and clinical symptoms every 3 months during the 1st year. (0,3,6,9,12months). Long-term follow up is required, especially for macroadenomas. DISCONTINUING MEDICATIONS
- 26. Agents have been used pre-op in some cases to try to decrease tumor size for surgery. Bromocriptine: Size reduction in only ≈ 20% of patients. Octreotide reduces tumor volume in ≈ 10% of cases. Paucity of dopaminergic receptors on cell membranes in these tumors. Surgery and/or XRT are usually the initial treatment of choice for hormonally inactive tumor. Follow-up recommendations for medically managed hormonally inactive macroadenomas For asymptomatic microadenomas (<1 cm dia), recommend: F/U pituitary MRI at years 1, 2, 5 and ± 10 (can stop F/U after 10 and possibly 5 years if no growth). For tumors >1 cm, recommend: check visual fields, pituitary bloodwork (to R/O pituitary insu ciency) and pituitary MRI at years 0.5,1,2 &5, and any time symptoms develop. NON RESPONDERS
- 27. PROLACTIN LEVEL WITH DAAGONIST TREATMENT PRL LEVEL (NG/ML) RECOMMENDATION <20 Maintain 20–50 Reassess dose >50 Consider surgery
- 28. Asymptomatic: Do no harm: Observe An aggressive surgical approach is indicated with these tumors since the secretion product is harmful and effective medical adjuvants are lacking. Pre-treat invasive GH-secreting tumors with somatostatin analogue therapy before surgery to reduce surgical risks (general and cardiac). Elderly patients or tumors >4 cm diameter: Debulk tumor transsphenoidally and/or adjuvant therapy (XRT and/or medications) Young age and size <4 cm: Radical surgery (may utilize a cranio-orbito-zygomatic skull base approach; may be curative) Medical therapy: Patients not cured by surgery Cannot tolerate surgery (e.g. due to cardiomyopathy, severe hypertension, airway obstruction For recurrence after surgery or XRT XRT For failure of medical therapy. To buy time among surgical failure who are awaiting XRT GH levels decline very slowly after XRT. GH secreting tumor
- 30. Elderly patient: expectant management is an option, with intervention for signs of progression (radiographic or neurologic). Parasellar tumor and/or young age: Radical surgery (often not curative) Central tumor or elderly patient with progression: trans-sphenoidal tumor debulking and/or XRT and close follow up. Radiation therapy: Recurrent or residual tumor or in patients who cannot tolerate surgery. 1.6 to 2 Gy four or five times per week for 5 to 6 weeks, for a maximum dose of 45 to 50 Gy. Radiotherapy controls tumor growth in 80% to 98% of non- functioning tumors May be considered: Dopamine agonists, valproic acid, somatostatin analogues, rosiglitazone, and serotonin agonists. Non-functional adenomas
- 31. 1. SRS is generally able to use a higher radiation dose per fraction than is conventional radiation, and it usually results in earlier endocrine control and induction of remission. 2. Stereotactic radiosurgery uses only a single session deliver focused radiation to lesion with less radiation to surrounding structures. 3. Options of SRS: GKS, LINAC, Cyberknife, FSRT, Proton beam therapy. 4. The major concern from SRS is radiation damage to the visual pathways. 5. Reduced by limiting the radiation dose to the optic chiasm to less than 10 Gy 6. Not good candidates for SRS (may undergo FRST) a. Adenomas closer than 2 to 5 mm to the optic chiasm or or conventional radiation b. Larger than 30 mm in diameter. 7. Side effects: a. Hormone deficiencie:13% to 41 b. Neuropsychiatric changes : SRS << conventional radiotherapy. c. Radiation necrosis ~ 0.2%. d. Optic neuropathy occurs in 1.7%, e. Vascular changes in 6.3%, f. Neuropsychological changes in 0.7%, and g. Radiation-induced secondary malignancies in 0.8%. SRS in PT
- 32. Hypo secretion Assessment Therapy Corticosteroid Co-syntropin test to assess cortisol reserve Failure to achieve a peak cortisol level>18 mcg/dl Cortisol 20mg AM, 10mg PM Hypothyroid Should never be started before corticosteroid risk Adrenal crisis. Synthyroid 125mcg/d 3-4 weeks for euthyroid Testosterone Increase intratumor estradio and promote risk of tumor growth Only after stabilization of tumor HORMONE REPLACEMENT THERAPY Dys thyroidism T4 TSH TSH response to TRH Primary hypo Low or N Elevated Elevated Secondary Hypo Low Low or N Reduced Primary Hyper Elevated Subnormal NA Secondary Hyper Elevated Elevated or inappropriately normal NA
- 33. Rare (< 140 reports). Usually invasive and secretory (most common hormones: ACTH, PRL). Can metastasize, at which point prognosis is poor (66% 1-year mortality). Little improvement with further surgery, XRT, or chemotherapy. PITUITARY CARCINOMA
- 34. GOALS OF SURGERY Eliminate mass effect from the pituitary and surrounding structures To preserve or restore pituitary and visual function To resect enough of the lesion to prevent recurrence, and To obtain tissue for histopathology analysis. OPTIONS: Craniotomy:Pterional/ Cranioorbitozygomatic approach. Trans sphenoid: Sublabial/Transnasal microsurgical Transnasal endoscopic SURGERY
- 35. Thank you NATIONAL INSTITUTE OF NEUROLOGICAL AND ALLIED SCIENCES, BANSBARI, KATHMANDUUPENDRA DEVKOTA MEMORIAL NATIONAL INSTITUTE OF NEUROLOGICALAND ALLIED SCIENCES, BANSBARI, KATHMANDU
Hinweis der Redaktion
- Diabetes Insipidus: causes: Autoimmune hypophysitis, Hypothalamic glioma, Suprasellar GCT, Kallaman’s syndrome. Differential diagnosis for a thickened stalk: lymphoma, autoimmune hypophysitis, granulomatous disease, hypothalamic glioma and sometime adenoma.
- Modified Hard’s classification: Extension A to E (sellar, anterior recess, displacement of floor, intradural parasellar and beneath the cavernous (extradurally); Invasion I-V (<10mm, >10mm, perforation of sphenoid sinus, Destruction of sphenoid sinus and Distant mets)
- IGF-1 (somatomedin-C) level is the recommended initial test (testing for elevated: excellent integrative marker of average GH secretion): Extremely sensitive for acromegaly). Normal levels depend on age (peaking during puberty), gender, pubertal stage and lab. Growth hormone (GH): normal basal fasting level is <5 ng/ml. Checking a single random GH level may not be a reliable indicator and is therefore not recommended In patients with acromegaly, GH is usually >10 ng/ml but can be normal. Normal basal levels do not reliably distinguish normal patient from GH deficiency Furthermore, due to pulsatile secretion of GH, normal patients may have sporadic peaks up to 50 ng/ml. Acromegaly may be present even with GH levels as low as 37 pg/ml: random GH levels are not generally useful for diagnosing acromegaly. Oral glucose suppression test (OGST): less precise and more expensive than measuring IGF-1: useful than IGF-1 for monitoring initial response to therapy. GH levels are measured at 0, 30, 60, 90 &120 minutes after a 75 gm oral glucose load. If the GH nadir is not <1 ng/ml, the patient is acromegalic. GH suppression may also be absent with liver disease, uncontrolled DM &renal failure Growth-hormone releasing hormone (GHRH) levels: may help diagnose ectopic GH secretion in a patient with proven acromegaly with no evidence of pituitary tumor on imaging. If an extrapituitary source is suspected, chest and abdominal CT and/or MRI should also be obtained Cctreotide scan: SPECT imaging 4 and 24 hours after injection with 6.5 mCi of indium-111 OctreoScan, a somatostatin receptor imaging agent Neurohypophysis (posterior pituitary): deficits are rare with pituitary tumors Screening: check adequacy of ADH by demonstrating concentration of urine with water deprivation Further testing: measurement of serum ADH in response to infusion of hypertonic saline
- Assess the cortisol production in 24 hours in serum and urine ( Normal 24hr serum cortisol: 20-90ug/ml, Urinary 17-OHCS: >150ug/ml), cortisol < 1.8ug/dl: cushing is ruled out. Cortisol> 10 ug/dl: CS is probably present. Assess sensitivity of HPA axis to negative feedback by glucocorticoids. Assess ACTH dependency: ACTH dependency diseases: Excess ACTH>>> Excess cortisol; ACTH independent diseases: Excess cortisol, Low ACTH, HPA suppressed. CRH and AVP are secretagogue and causes increased secretion of ACTH. Metyrapone are cortisol synthesis inhibitors: Increased cortisol or urinary 17-OHCS. If imaging is not conclusive of microadenoma: then adopt Inferior petrosal sinus sampling/ Cavernous venous sampling (more accurate but highly morbid than IPSS). Bilateral femoral catheter B/L IJV IPS; Simultaneous ACTH measurement after CRH stimulation. IPS: Peripheral ACTH: 2:1 (95% S; 100% S); 3:1: ( both 100%), Inter sinus gradient (>1.4) lateralize the lesion in 75%cases. Measure prolactin level too.