Salient Features of India constitution especially power and functions
64040266-Liver-Patho-and-Eco.pdf
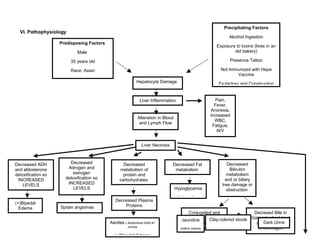
1. VI. Pathophysiology
inches
Predisposing Factors
Male
35 years old
Race: Asian
Hepatocyte Damage
Liver Inflammation Pain,
Fever,
Anorexia,
Increased
WBC,
Fatigue,
N/V
Alteration in Blood
and Lymph Flow
Liver Necrosis
Decreased ADH
and aldosterone
detoxification so
INCREASED
LEVELS
Decreased
Adrogen and
estrogen
detoxification so
INCREASED
LEVELS
Decreased
metabolism of
protein and
carbohydrates
Decreased Fat
metabolism
Decreased
Bilirubin
metabolism
and or biliary
tree damage or
obstruction
(+)Bipedal
Edema Spider angiomas
Decreased Plasma
Proteins
Ascites ( Abdominal Girth:41
inches
(+)Bipedal Edema
Hypoglycemia
Malnutrition
Conjugated and
unconjugated
hyperbilirubinemia
Decresed Bile in
Gatrointestinal tract
and Increased
Urobilinogen
Jaundice
(icteric sclera)
Dark Urine
Clay-colored stools
Precipitating Factors
Alcohol Ingestion
Exposure to toxins (lives in an
old bakery)
Presence Tattoo
Not Immunized with Hepa
Vaccine
Ex-factory and Construction
2. The specific cause of hepatic encephalopathy is unknown, but it
is characterized by elevations of ammonia levels in the blood and
cerebrospinal fluid (CSF). Ammonia is produced in the gastrointestinal
Liver Failure
Liver fibrosis and
scarring
Portal
Hypertension
Ascites
Spleenomegaly
Bleeding
Anemia
Thrombocytopenia
Delayed
Wound Healing
Infection
Inability to
metabolism
ammonia to urea
Hepatic
Encephalopathy
(+) Asterixis
Alteration in
sleep
Respiratory
Acidosis
Confusion to
hepatic coma
Precipitating
Factors
>Constipated for
2 weeks
Increase Serum
Ammonia level
And toxins
Accumulation of
Toxic substances in
the intestine
Toxins are absorbed
into the portal
venous flow
Toxins then
circulate at
elevated
concentrations in
the systemic blood
Reach the brain
through the blood-
brain barrier
Impair cerebral
function leading to
altered higher
functions and
consciousness
3. tract when protein is broken down by bacteria, by the liver, and in lesser amounts, by gastric juices and peripheral tissue metabolism. The
kidneys are another source of ammonia in the presence of hypokalemia. More recently implicated as a cause of encephalopathy are false
neurotransmitters, elevated mercaptans (organic chemical that contain sulfhyldryl radical formed when the oxygen of an alcohol molecule is
replaced by sulfur), phenol, and short-chain fatty acids.
Normally the liver converts ammonia into glutamine, which is stored in the liver and is later converted to urea and excreted through the
kidneys. Blood ammonia level rise when the liver cells are unable to perform this conversion. Failure of the liver to perform this function may
be due to liver cell damage and necrosis. It may also result from the shunting of blood from the portal venous system into the systemic,
venous circulation (bypassing the liver). In either case, as blood ammonia level rise, many unusual compounds begin to form.
Some of these compounds (e.g. octapamine) apparently act as false neurotransmitters in the CNS. Ammonia also is a CNS toxin,
affecting glial and nerve cells; it leads to altered CNS metabolism and function.
Any process that increases protein in the intestine, such as increased dietary protein or gastrointestinal bleeding, causes elevated
blood ammonia levels and possible manifestations of hepatic encephalopathy in clients with hepatocellular failure of have undergone
portosystemic shunt surgery.
(Black and Hawks, Medical-Surgical Nursing: Clinical Management for Positive Outcomes 8th
Edition, Vol. 1, Page 1166)
4. Ammonia
Entering the blood
stream
Converting
ammonia to urea
Muscle cells
Absorption GI tract
Liberation from
kidney
S/Sx: Edema,
bleeding
Increased ammonia
concentration in the blood
Brain dysfunction
S/Sx:
Motor disturbances, mental
changes
Damage
HEPATIC ENCEPHALOPATHY
>Incohere
nt
>Disorient
ed
>Slurred
speech
>Paresis
5. VII. Ecologic Model
A. Hypothesis
The host factors of the client have a significant effect to the client’s predisposition to hepatic encephalopathy
secondary to liver cirrhosis rather than environmental factors. Specifically the age, being a male and Asian, alcohol
ingestion, history of smoking, family history of alcohol drinkers, eating habits, elimination pattern, lifestyle habits and
stress.
B. Predisposing Factors
1. Host
Age:
35 years old
Sex:
Male- The difference in incidence between the sexes is more pronounced, with male-to-female ratios as
high as 8:1
Race:
Asian- Most commonly found among Asian persons, due to childhood infections with hepatitis B.
Nationality:
Filipino- The client belongs into a third world country where in incidence of high rates of infectious hepatitis
occur.
6. Behavior:
Alcohol Ingestion- The client ingest 1-2 bottles of alcoholic drinks once a week for about 15 years. The
primary risk for alcohol cirrhosis is alcohol ingestion, especially in the absence of proper nutrition. (Black and Hawks,
Medical-Surgical Nursing: Clinical Management for Positive Outcomes 8th
Edition, Vol. 1, Page 1147)
History of smoking- The client consumes half pack of cigarettes per day for about 15 years; he has stopped
just 1 year ago. The ingredients in the cigarettes affect everything from the internal functioning of the organs to the
efficiency of the body’s immune system. (http:quitsmoking.about.com/od/tobaccostatistics/a/cigarettesmoke.htm)
Eating Habits- The seldom eat vegetables before, he loves to eat adobo and sinigang na baboy. He prefers meat
viands than vegetables. He frequently eats street foods like “isaw”.
Elimination Pattern- Whenever he feels the urge to defecate or urinate he seldom attend to it immediately because of
the proximity of their comfort room, he is having a difficulty ambulating, because he feels weak. He has been constipated for 2
weeks prior admission.
Customs:
Lifestyle Habits
- Presence of tattoos-The tattoos was applied at home with Chinese ink.
- Lack of Hepa Vaccinations
Heredity:
7. Family history of alcohol drinkers-any client with a family history of alcoholism should avoid alcohol because
of the increase risk. (Black and Hawks, Medical-Surgical Nursing: Clinical Management for Positive Outcomes 8th
Edition, Vol. 1, Page 1147)
2. Agent
Chemical: Alcohol
3. Environment:
Physical: Exposure to toxins at their house (old bakery), and at the construction and factory place where he had
worked. Lives in a congested environment
Biologic: Response to alcohol exposure
Socio-economic: Lives in a congested environment, availability of alcohol
C. Ecologic Model
In many respects, alcohol can be considered the causal agent in alcohol psychiatric disorders because it must be present for
alcoholism to occur. However, the fact that most drinkers do not become alcoholics indicates that it is a necessary, but not sufficient
cause. Suitable conditions of the host and environment must also be present for disease to develop, and the concept that a number
of factors influence the occurrence of disease is referred to as multiple causation or multi-factorial causation. In the past, particularly
in the context of the epidemiology of infectious disease, a triangle has been used to illustrate relations between three factors that
contribute to the occurrence of disease, the agent or proximal cause of the disease, the host, and the environment. Increasingly, with
the study of chronic and mental disorders having a complex, multifactorial etiology, many epidemiologists have come to prefer
8. models in which the agent is considered part of the total environment. The wheel model –de-emphasizes the role of the agent and
stresses the multiplicity of interactions between the host and the environment.
The wheel model depicts the human host with his genetic makeup at its core; the surrounding environment is divided into
three sectors: biologic, social, and physical.
HOST
Family
Histor
y of
Alcoho
lism
Biological Environment Social Environment
Physical Environment
35 y/o
Asian
Ex-factory and
construction
worker
Alcohol
Ingestion
Eating
Habits
Elimination Pattern
Male
No
hepa
vaccine
tattoos
Response
to alcohol
exposure
Availabilty
of Alcohol
Lives in a congested
environment
Exposure to
toxins at their
house (old
bakery), and
work place
Lives in a congested
environment
9. D. Analysis
Cirrhosis is defined histologically as a diffuse hepatic process characterized by fibrosis and the conversion of
normal liver architecture into structurally abnormal nodules. The progression of liver injury to cirrhosis may occur over
weeks to years. Indeed, patients with hepatitis C may have chronic hepatitis for as long as 40 years before progressing to
cirrhosis. There are many causes of cirrhosis; they include chemicals (such as alcohol, fat, and certain medications),
viruses, toxic metals (such as iron and copper that accumulate in the liver as a result of genetic diseases), and
autoimmune liver disease in which the body's immune system attacks the liver.
The prevalence of liver disease is influenced by many factors, including genetic factors (e.g., predilection to alcohol
abuse, sex) and environmental factors (e.g., availability of alcohol, social acceptability of alcohol use, concomitant
hepatotoxic insults), and it is therefore difficult to define. In general, however, the risk of liver disease increases with the
quantity and duration of alcohol intake. Although necessary, excessive alcohol use is not sufficient to promote alcoholic
liver disease. Only one in five heavy drinkers develops alcoholic hepatitis, and one in four develops cirrhosis.
Hepatic encephalopathy, a challenging complication of advanced liver disease, occurs in approximately 30–45% of
patients with cirrhosis and 10–50% of patients with transjugular intrahepatic portosystemic shunt, while minimal hepatic
encephalopathy affects approximately 20–60% of patients with liver disease. (Poordad,F. 2006) Hepatic encephalopathy
is caused by disorders that affect the liver. These include disorders that reduce liver function (such as cirrhosis or
hepatitis) and conditions in which blood circulation does not enter the liver. The exact cause of hepatic encephalopathy is
unknown. Hepatic encephalopathy may be triggered by: dehydration, eating too much protein, electrolyte abnormalities
(especially a decrease in potassium) from vomiting, or from treatments such as paracentesis or taking diuretics ("water
pills"), bleeding from the intestines, stomach, or esophagus, infections, kidney problems, low oxygen levels in the body,
Shunt placement or complications (See: Transjugular intrahepatic portosystemic shunt ), surgery, use of medications that
suppress the central nervous system (such as barbiturates or benzodiazepine tranquilizers).Hepatic encephalopathy may
occur as an acute, potentially reversible disorder. Or it may occur as a chronic, progressive disorder that is associated
with chronic liver disease. (http://www.nlm.nih.gov/medlineplus/ency/article/000302.htm)
E. Conclusion and Recommendations
10. I therefore conclude that the host factors have a significant effect to the client’s predisposition to hepatic
encephalopathy secondary to liver cirrhosis. Since the client has already a liver cirrhosis and experienced hepatic
encephalopathy, prevention for further complications is the only one that can be provided and supported for the client.
However liver damage was not yet that clinically assessed in terms of laboratory diagnosis for its extensibility or severity to
be able to make necessary interventions for treatment and rehabilitation. Factors such as alcohol ingestion, application of
tattoo not aseptically, lack of hepa vaccination, presence of liver cirrhosis, eating habits-increase in protein intake,
elimination pattern-not attending urge to defecate are the factors that readily predisposes client to hepatic encephalopathy.
Since host factors consist of modifiable and non modifiable factors which synergized by the client’s environment to
predispose into a complication of liver disease, modifiable factors must then be addressed immediately, client must have
lifestyle modifications like abstinence from alcohol consumption and cigarette smoking.
We as nurses must continue facilitating patient to take less sodium and Protein intake, give medication as prescribe,
Encourage patient to have a clean and safe environment for faster recovery. Rationale: Clean and safe environment
promotes comfort and relaxation for faster recovery of the patient. Encourage the patient to be calm and maintain a
comfort position. Educate the patient and family the importance of proper medication administration and timing. Encourage
the client to inhale and exhale exercise. Rationale: To improve air gas exchange in the body. Encourage the patient to
have a low cholesterol, low sodium and low carbohydrate diet Rationale:For the blood volume not to increase resulting to
hypertension. Encourage the patient to continue praying and seek guidance from God Rationale:Strong faith to God helps
the patient spiritually to alleviate the condition with God's will.