This document summarizes the results of a global survey on community perspectives regarding task-shifting of HIV services from doctors to nurses and community health workers. The survey received responses from over 1000 people in 122 countries. While most respondents supported task-shifting if nurses and health workers received proper training, their views differed on which specific tasks should be shifted. Respondents identified lack of training, inadequate pay, and unsupportive policies as barriers to effective task-shifting. The survey provided insights into community acceptance of task-shifting but had limitations due to its online format and non-random sampling.
Community perspectives on task-shifting/ sharing: a multi-country survey to inform WHO consolidated ARV guidelines
1. PRESENTED AT IAS 2013 – KUALA LUMPUR, MALAYSIA
Introduction
• With 33 million people living with HIV globally and a shortage of human resources for health, there has been
an interest in shifting selected tasks from specialized to less specialized health workers. In several settings,
decentralizationofHIVservicesmayentailengaginglessspecializedcadresofhealthworkerstoprovideservices
at community-level. Building on lessons learned from past and current community-based interventions, task-
shifting/sharing can potentially expand access and retention in HIV care. However, community perceptions
regardingnursesandcommunityhealthworkers(CHW)providingHIVcareandtreatmentremainundocumented.
• This consultation was conducted to understand community perspectives on task-shifting/sharing and to inform
the development of the 2013WHO Consolidated Guidelines on the Use ofAntiretroviral Drugs forTreating and
Preventing HIV Infection.
•Perceptions Task-Shifting/Sharing
One-third (33%, n=366) of all respondents (n=1088) answered the questions on task-shifting/sharing.1
For the following questions,no significant differences were observed,on perception of task shifting/sharing,
based on country’s income status, HIV status, or gender of respondents.
Who?
If nurses and CHWs receive adequate training and regular supervision and updating,they should be allowed
to provide HIV care and treatment services to people living with HIV who are stable and do not require a
doctor’s consultation.
• Which tasks?
Although the majority of respondents supported task-shifting/sharing to nurses and CHWs, there were
differences regarding which specific tasks should be shifted
Methods
Between November and December 2012, the International HIV/AIDSAlliance and the Global Network of People
Living with HIV conducted a global community consultation, reaching 122 countries, using an online E-Survey
(available inArabic, Chinese, English, French, Spanish, and Russian).
With regards to task-shifting/sharing the survey asked the following questions:
• ‘If provided with adequate training, regular supervision, and updating, should nurses provide HIV care and
treatment services to people living with HIV who are stable and do not require a doctors’ consultation?’
• ‘Ifprovidedwithadequatetraining,regularsupervision,andupdating,shouldcommunityhealthworkers(CHW)
provide HIV care and treatment services to people living with HIV who are stable and do not require a doctors’
consultation?’
Results
• E-Survey Participant Characteristics
There were 1088 e-survey respondents from low (21%), middle (59%), and high (20%) income countries. Of the
791 who reported gender,38% were female,61% were male,and 1% were transgender.Median age range was
35-44 years old (n=280). Of the 864 who reported their HIV status, 50% self-reported as being a person living
with HIV (n=431). Of the 489 who identified with a key population, 45% were men who have sex with men
(n=220), 6% were people who use injecting drugs (n=28), 6% were sex workers (n=30), 16% were pregnant
women (n=80), and 9% were refugees or migrants (n=42).
Gitau Mburu1
, Amy Hsieh2
, Mala Ram1
, Christopher Mallouris3
, Masaya Kato1
, Eyerusalem Negussie4
, Cadi Irvine3
1
International HIV/AIDS Alliance; 2
Global Network of People Living with HIV; 3
Social Justice 4 All; 4
World Health Organization
COMMUNITY PERSPECTIVES ON TASK-SHIFTING/
SHARING: A MULTI-COUNTRY SURVEY TO INFORM
WHO CONSOLIDATED ARV GUIDELINES
Box 1. Definitions
Task-shifting shifting involves the rational redistribution of tasks among health
workforce teams. Specific tasks are moved, where appropriate, from highly qualified
health workers to health workers with shorter training and fewer qualifications in order
to make more efficient use of the available human resources for health.
Task-sharing is another term used to emphasize sharing of clinical tasks among teams
of different cadres of health workers.Both emphasize the need for training and continued
educational support of all cadres of health workers in order for them to undertake the
tasks they are to perform.
Source: Task shifting: rational redistribution of tasks among health workforce
teams: global recommendations and guidelines. WHO, UNAIDS, PEPFAR. 2008
(http://www.who.int/healthsystems/TTR-TaskShifting.pdf, accessed 11 June
2013).
10-19 20-24 25-34 35-44 45-54 55-56 65+
1,1%
6,1%
30,0%
30,0%
21,5%
7,6%
1,9%
Figure1. Respondent Self-Reported Age Figure 2. Respondent Country Income Status
High
21%
Middle
58%
Low
21%
(according to World Bank definitions)
Figure3. Task-shifting/sharing to Nurses
(n=365)
Figure4. Task-shifting/sharing to CHWs
(n=367)
OTHER
19%
NO
6% YES
75%
OTHER
11%
NO
18%
YES
71%
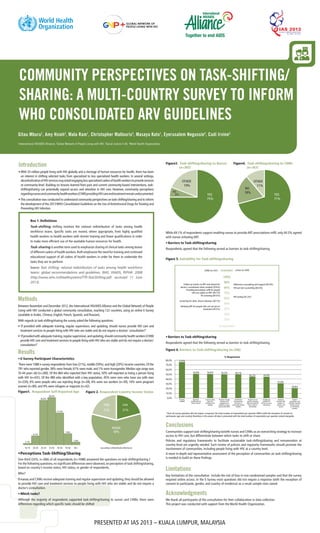
Figure 5. Suitability for Task-shifting/sharing
100%
90%
80%
70%
60%
50%
40%
30%
20%
AGREEMENT
DISAGREEMENT
Follow up checks on ART and referral for
doctor’s consultation when needed (78.6%)
Providing prescription refill for people
who are stable on ART. (69.1%)
TB screening (64.5%)
Screening for other chronic diseases (58.1%)
Initiating ART for people who are not yet on
treatment (44.5%)
Adherence counselling and support (85.9%)
HIV pre-test counselling (83.6%)
HIV testing (67.2%)
nurses (n=356)CHWs (n=351)
• Barriers to Task-shifting/sharing
Respondents agreed that the following served as barriers to task-shifting/sharing.
Figure 6. Barriers to Task-shifting/sharing (n=346)
80,0%
70,0%
60,0%
50,0%
40,0%
30,0%
20,0%
10,0%
0,0%
75,6%
50,9% 50,6% 50,3% 49,7%
45,2% 44,9%
31,0%
20,8%
% Responents
Training
needed
Need for
certification for
those trained
Country policy
does not
facilitate task
shifting
Need to change
policies and
regulations to
authorize nurses
to prescribe ARVs
Insufficient
remuneration
of nurses or
community health
workers
People are not
used to receiving
ARV prescriptions
from nurses or
community
Inadequate
systems for
doctor to nurse
mentoring
Imalance
between the
number of
doctors and
nurses
Gender
preception and
relations towards
female nurses
or community
workers
1
Since all survey questions did not require a response, the total number of respondents per question differs (with the exception of consent to
participate, age, and country) therefore, in this poster all data is presented with the total number of respondents per question stated alongside.
Conclusions
Communities support task-shifting/sharing to/with nurses and CHWs as an overarching strategy to increase
access to HIV care, but differentiate between which tasks to shift or share.
Policies and regulatory frameworks to facilitate sustainable task-shifting/sharing and remuneration at
country-level are urgently needed. Such review of policies and regularity frameworks should promote the
involvement of communities, including people living with HIV, at a country level.
A more in-depth and representative assessment of the perception of communities on task-shifting/sharing
is needed to build on these findings.
While 69.1% of respondents support enabling nurses to provide ART prescriptions refill, only 44.5% agreed
with nurses initiating ART.
• Barriers to Task-shifting/sharing
Respondents agreed that the following served as barriers to task-shifting/sharing.
Limitations
Key limitations of the consultation include the risk of bias in non-randomised samples and that the survey
required online access. In the E-Survey most questions did not require a response (with the exception of
consent to participate, gender, and country of residence) as a result sample sizes varied.
Acknowledgments
We thank all participants of the consultation for their collaboration in data collection.
This project was conducted with support from the World Health Organization.