Good Stuff Happens in 1:1 Meetings: Why you need them and how to do them well
Schuckit alcoholism (1) psychology A2 addiction
1. M. Thérèse Southgate, MD, Section Coordinator
Genetics and the Risk for Alcoholism
Marc A. Schuckit, MD
The importance of genetic factors in alcoholism is supported by the
familial nature of this disorder, the significantly higher concordance rate in
identical than in fraternal twins, and the fourfold higher risk for children of
alcoholics, even when adopted out at birth. Based on this evidence, the
search is under way to identify possible genetically influenced factors that
might contribute to the alcoholism risk. Studies of populations at high risk for
the future development of alcoholism (eg, sons of alcoholics) have revealed
a probable decreased intensity of reaction to modest doses of ethanol, a
possible decreased amplitude of the P300 wave of the event-related
potential, and a possible decreased amount of g=a-waveactivity on the
background cortical electroencephalogram. The implications of these and
other findings and their impact on the practice of medicine are explored.
(JAMA 1985;254:2614-2617)
ALCOHOLISM afflicts 10% of adult
men and 3% to 5% of adult women at
some time during their lives, with an
even higher rate among patients
attending medical clinics.12 This arti¬
cle reviews studies evaluating genetic
factors that might contribute to the
risk for this prevalent disorder.
The importance of genetics in the
vulnerability toward alcoholism is
supported by evidence from family,
twin, and adoption studies in humans.
First, the familial nature of alcohol¬
ism (ie, the way it occurs in families)
has been documented for more than
100 years.1 The risk appears to
increase with the number of alcoholic
relatives and the closeness of the
genetic relationship. However, many
familial factors are not genetically
influenced.
The second approach, studies of
twins, takes advantage of an experi¬
ment of nature. Twin pairs are born
at the same time and are likely to
experience major childhood events
(eg, death of a parent) at the same
age. Therefore, if childhood environ¬
ment is important in the development
of alcoholism, the risk should be
elevated in the twin of an alcoholic,
no matter what type of twinship is
involved. However, there are two
types of twins; identical, who share
100% of their genes, and fraternal,
who share only 50% (the same as any
two full siblings). As a result, if
alcoholism is genetically influenced,
the risk for the identical twin of an
alcoholic should be significantly high¬
er than the risk for a fraternal twin.
While there is some debate,4 the
majority of studies demonstrate a
concordance of 60% or higher for the
identical twin of an alcoholic but a
risk of only 30% or less if the rela¬
tionship is fraternal.5
The most impressive evidence sup¬
porting the importance of genetic
factors in alcoholism comes from
adoption-type studies. Investigations
from different countries using a vari¬
ety of methods have demonstrated
that adopted-away children of alco¬
holics are at four times higher risk
for this disorder than controls.*"8 Once
the influence of a biological alcoholic
parent is considered, being reared by
an alcoholic does not seem to add to
the risk, and children of nonalcoholics
raised by alcoholics do not appear to
have an enhanced rate of this prob¬
lem.
RESEARCH APPROACHES WITH
POPULATIONS AT HIGH RISK
FOR ALCOHOLISM
In response to these findings, a
number of laboratories have begun to
ask how the genetic risk might be
mediated.8 One promising approach
has been to evaluate nonalcoholic
close relatives of alcoholics, limiting
the study to men who are young
enough to have not entered the major
age of risk for alcoholism—ie, popula¬
tions at high future risk are observed.
The assets of this research design
include the almost inexhaustible
number of potential subjects, the
large number of families investigated
so that numerous factors might be
determined, and the ability to observe
individuals at high risk before alco¬
holism actually develops.
In most studies of populations at
high risk, potential subjects are
males who have an alcoholic family
member (usually a first-degree rela¬
tive and most frequently the father).
Some investigators have chosen to
evaluate male children in the preteen
or early teen years, thus increasing
the probability that subjects are
naive to the effects of ethanol. These
young men are often chosen from
among families of alcoholics attend¬
ing an alcoholic treatment program
or from teenaged subjects identified
because of police problems.9" Other
investigations have focused on older
groups to avoid the long lag time
between evaluation and the actual
development of alcoholism (should
follow-up studies be planned). This
also maximizes the opportunity to
observe potentially important inter¬
actions between the genetic predispo¬
sition and adaptations to ethanol over
years of modest drinking. Men are
chosen for most studies because
responses to an ethanol challenge
might be affected by the phase of the
From the Department of Psychiatry, University of
California at San Diego School of Medicine, and the
Alcohol Research Center, San Diego Veterans
Administration Medical Center.
Reprint requests to Department of Psychiatry,
San Diego Veterans Administration Medical Center,
3350 La Jolla Village Dr, San Diego, CA 92161 (Dr
Schuckit).
Downloaded from jama.ama-assn.org at Mt Sinai School Of Medicine on April 23, 2012
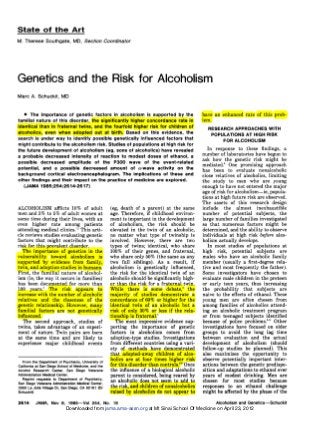
2. After Ethanol Ingestion, min
Fig 1.—Mean self-ratings on a 0 (none) to 36 (great) scale for drug
effect after placebo and after 0.75 mL/kg of ethanol for 23 matched
pairs with positive (close circles) and negative (open circles) family
histories. Bars indicate SEs. After 0.75 mL/kg, using a two-factor,
mixed-model, repeated-measures analysis of variance in which sub¬
jects were nested with respect to the between factor (family history)
and crossed with respect to the within factor (time), the differences
between family groups were significant (F=5.99, 1,44 df, P<.02).
(Figure reproduced from Archives of General Psychiatry 1984;
41:879-884.)
5
Baseline 140 170 240
After Ethanol Ingestion, min
Fig 2.—Percent increase in body sway or standing steadiness
following 0.75 mL/kg of ethanol for 23 matched pairs with positive
(close circles) and negative (open circles) family histories. Bars
indicate SEs. Using the same statistical approach as in Fig 1, after
0.75 mL/kg of ethanol the two family groups differed significantly
(F=3.84, 3,197 df, P=.01). (Figure reproduced from Archives of
General Psychiatry 1985;42:375-379.)
menstrual cycle or the type of birth
control pills being consumed by
women.
My own laboratory chose to sample
21- to 25-year-old male students and
staff at a university who responded to
a mailed questionnaire. After exclud¬
ing those persons who have serious
alcohol- or drug-related life problems
or major medical or phychiatric dis¬
orders, those drinking but nonalco¬
holic young men who report a close
alcoholic relative are placed in the
family history-positive or high-risk
group. Each man with a positive
family history is matched on de¬
mography (age, sex, religion, race,
educational level, etc), drinking histo¬
ry, and height-to-weight ratio with an
individual in the family history-nega¬
tive (low-risk) group for alcoholism.
In my work, matched high- and
low-risk men are then individually
brought to the laboratory three times,
where raters blind to the family his¬
tory measure personality attributes,
cognitive and psychomotor func¬
tioning, and some electroencephalo-graphic
(EEG) parameters. After
these baseline procedures have been
completed, subjects are administered
one of three beverages; placebo, 0.75
mL/kg of ethanol, or 1.1 mL/kg of
ethanol (roughly the equivalent of
about three and six drinks, respec¬
tively), with active doses consumed
over ten minutes as a 20% by volume
solution in a sugar-free carbonated
beverage. Subjects are then observed
over the subsequent four hours.
SOME RESULTS OF STUDIES OF
HIGH-RISK POPULATIONS
This section briefly reviews results
from some studies of populations at
high risk for alcoholism. While I
emphasize my own work, relevant
data from different laboratories are
also included. The results relate to
differences between high- and low-risk
groups in both baseline function¬
ing and in response to an ethanol
challenge.
Three possible differences between
the high- and low-risk groups stand
out as a result of these studies of
groups at elevated risk. Sons of alco¬
holics appear to show less intense
responses to modest ethanol doses,
demonstrate lower amplitudes of a
brain wave that might measure selec¬
tive attention, and may have different
characteristics of brain a rhythms.
Other interesting and potentially im¬
portant results are also reviewed in
the following paragraphs.
A Decreased Intensity of
Response to Ethanol
The risk of developing alcohol-related
problems might increase if a
person were relatively less able to
estimate how intoxicated he was
becoming at a modest blood alcohol
concentration.12 This could make it
more difficult to learn when to stop
drinking; ie, when a few more drinks
will result in drunkenness. To test the
possibility that this might relate to
the future alcoholism risk, in my own
and other laboratories men in highl¬
and low-risk groups have been admin¬
istered a series of subjective, cogni-tive/
psychomotor, and biological
tests before and after beverage alco¬
hol consumption.
Before consuming a test drink, the
two family history groups had similar
expectations of what ethanol was
likely to do to them.13 u Also, the blood
alcohol concentrations achieved fol¬
lowing the two active ethanol chal¬
lenges were identical for the two
family groups, indicating similar pat¬
terns of absorption, distribution, and
metabolism of ethanol."" High-risk
and low-risk group members have
also shown parallel changes on most
measures of intoxication following
Downloaded from jama.ama-assn.org at Mt Sinai School Of Medicine on April 23, 2012
3. placebo. Thus, any family history
group differences on the intensity of
acute reaction to ethanol are unlikely
to reflect levels of expectancy, placebo
response, or differences in blood alco¬
hol concentrations.
The first indication that high- and
low-risk groups might differ signifi¬
cantly in their actual reaction to
ethanol came from self-reports of
levels of intoxication following chal¬
lenges. Even after partialing out the
subjects' feelings after drinking pla¬
cebo, three studies in my own labora¬
tory and two additional investiga¬
tions have shown that the group with
a positive family history for alcohol¬
ism report significantly less subjec¬
tive intoxication after drinking than
the group with a negative family
history.13 " These data are exemplified
in Fig 1, which shows the significant
differences in the two groups after
the lower ethanol challenge (0.75 mL/
kg). A similar trend was also
observed after achieving higher blood
alcohol concentrations (eg, after 1.1
mL/kg of ethanol), but the group
differences were not as marked.
Aspects of cognitive and psychomo-tor
test performance as well as some
biological reactions after drinking
parallel the subjective levels of intox¬
ication. In my laboratory, subjects
with a positive family history demon¬
strated significantly less increase in
the amount of ethanol induced body
sway or static ataxia (a modified
Romberg sign) than those in the
low-risk group (Fig 2); again, there
was a greater differential following
the lower ethanol dose." Further bol¬
stering these results, preliminary
data showed a greater decrement in
performance on a number of cognitive
and psychomotor tests (eg, a divided-attention
task, the Trail Making Test,
etc) in the low-risk group, as well as
more intense changes in two hor¬
mones known to react to an acute
ethanol challenge, cortisol and prolac-tin.
1718
In summary, there is consistent
evidence that those in the high-risk
group demonstrate significantly less
intense reactions to modest doses of
ethanol than those in the low-risk
group. It may be that they are feeling
less ethanol effect at the blood alco¬
hol concentrations at which most peo¬
ple make a decision to stop drinking.
Electrophysiological Measures
Two additional promising areas of
research involve EEG differences be¬
tween the high- and low-risk groups.
First, brain-stem auditory event-related
potentials (ERPs) are com-puter-
averaged brain waves mea¬
sured by exposing subjects to a train
of regular stimuli (eg, clicks or
flashes of light) as they are asked to
discern a randomly occurring unusual
stimulus.' When the anticipated rare
event occurs (eg, a tone of a different
frequency than the others), a positive
brain wave is recorded between 300
and 500 ms (the P300) following the
stimulus. Studies of préadolescent
sons of alcoholics by Begleiter and
colleagues' have revealed a lower
P300 amplitude for these boys, even
without ethanol. This might indicate
that some of these young men may
experience difficulties in adequately
focusing attention on their surround¬
ings. It is possible that this phenome¬
non might contribute to the decreased
sensitivity to modest ethanol doses
reported in my work.
Second, alcoholics seem to have a
deficiency in the amount of a rhythm,
or slow waves, in their background
cortical EEGs." Similar a-wave defi¬
ciencies may be seen in sons of alco¬
holics, along with a possible greater
increase for waves in the a band after
drinking.20 If the amount of a rhythm
relates to feelings of relaxation,21 then
these data may indicate that there is
a qualitatively different type of
"high" in the high- and low-risk
groups.
Some Additional
Areas of Research With
High-Risk Populations
A number of studies have ad¬
dressed whether high- and low-risk
groups differ on the metabolism of
ethanol. The two family history
groups have similar blood alcohol
concentration patterns after drink¬
ing,13"22 but there is a possible differ¬
ence between the groups on the level
of accumulation of the toxic and psy-choactive
first breakdown product of
ethanol, acetaldehyde. While not all
studies agree,2324 three groups have
reported that blood and breath levels
of this potent substance tend to be
higher after drinking in the sons of
alcoholics than in controls.2527 How¬
ever, conclusions are undermined by
inadequate technology for the mea¬
surement of acetaldehyde, with re¬
sulting disagreements about the va¬
lidity and sensitivity of the assay procedures.23
A variety of studies have also
looked at personality profiles of high-risk
and low-risk pairs. In my labora¬
tory, using students closely matched
for demography and drinking history,
the two family groups were similar on
most subtests of the Minnesota Multi-phasic
Personality Inventory (MMPI),
the Eysenck Personality Inven¬
tory measures of extroversion and neu-roticism,
levels of anxiety, and the
feelings of control over external
events.2831 Other researchers, looking
at less highly selected groups usually
identified as a consequence of police
problems or because their fathers
were currently in treatment for alco¬
holism, have reported profiles of
increased risk-taking and impulsivity
in those with a positive family histo¬
ry32 and indicated a possible associa¬
tion between signs of hyperactivity in
childhood and the later development
of alcoholism.33 The divergence of
results from different studies does
not justify solid conclusions on the
association between measurable per¬
sonality attributes and the risk for
the future development of alcoholism,
but this remains an important area
for future research.
Young children of alcoholics have
also been reported to demonstrate
poorer performance on verbal intelli¬
gence and the Categories Test of the
Halstead-Reitan Battery and tend to
show more difficulties in psycho-motor
performance, abstracting
abilities, and auditory wordspan per¬
formance.10" However, studies of col¬
lege-age children of alcoholics have
revealed no differences before ethanol
challenge on body sway, memory, and
divided-attention tasks, nor on other
cognitive or psychomotor test per¬
formance measures.13 " 3435 In addition,
prospective studies of population co¬
horts that included some individuals
who later became alcoholic have dem¬
onstrated no consistent correlation
between relatively obvious neurologi¬
cal or intellectual problems and the
later development of alcoholism.34 In
the final analysis, the associations
between the alcoholism risk and mea¬
surable signs of neurological damage
in children of the average alcoholic
are complex and might differ with the
sample selected for study.
CONCLUSIONS
This discussion has centered on
some exciting research generated
over the last decade. The studies
suggest that genetic influences are
important in alcoholism and reflect
multiple genes interacting with envi¬
ronment to produce a final level of
risk. In this theory, no one is predes¬
tined to become an alcoholic, but
genetic factors increase or decrease
the level of vulnerability toward this
disorder. Taking advantage of the
fourfold higher risk in sons of alco¬
holics, subjects predisposed toward
Downloaded from jama.ama-assn.org at Mt Sinai School Of Medicine on April 23, 2012
4. alcoholism have been studied in the
preteen years and in the early 20s,
with populations selected from cam¬
puses, court dockets, and from fami¬
lies of alcoholics in treatment. The
evaluation of levels of functioning
both before and after an ethanol
challenge has revealed some interest¬
ing differences between high-risk
populations and controls.
The most consistent data indicate
that an alcoholism vulnerability
might be, in part, related to factors
that result in a decreased intensity of
reaction to ethanol. This might subse¬
quently interfere with the ability to
learn to discriminate the blood alco¬
hol concentrations at which drinking
should cease during an evening. Other
studies indicate possible differences
between groups with a negative or
positive family history on the ability
to attend adequately to a stimulus
(one possible mechanism for an
inability to discriminate modest blood
alcohol concentration effects) and
potential differences on the effects of
ethanol on a. rhythms in the back¬
ground cortical EEGs (perhaps re¬
flecting the ability to feel relaxation
in the presence of ethanol).
Despite this progress, these studies
are still in their infancy. Research
must next establish the generalizabil-ity
of results to women and divergent
ethnic and socioeconomic groups.
Also, the actual biological mecha¬
nisms responsible for the reactions to
ethanol and/or EEG attributes of a
positive family history of alcoholism
must be elucidated, the level of
genetic control of these phenomena
must be established, and the actual
linkage, if any, to the final develop¬
ment of alcoholism must be proved.
Even recognizing these limitations,
there are a number of implications of
the data for the daily practice of
medicine. First, the evidence support¬
ing the importance of genetic factors
in this disorder, combined with clini¬
cal experience, underscores the im¬
portance of recognizing that alco¬
holism is a biologically influenced
problem, not a moral weakness. Many
physicians may need to change their
stereotype of alcoholics or they will
continue to misdiagnose the average
middle-class alcoholic who needs
help.3637 Second, no matter how they
are mediated, the genetic factors can
help us begin to work on preventing
this illness. While the optimum
approach to prevention has not been
found, it makes sense that children of
alcoholics should be educated about
their risk, taught that they may not
react to alcohol the way their peers
do, and informed that attempting to
drink like others could be a dangerous
undertaking.
Finally, the implications for the
future of prevention and treatment of
alcoholism are even more marked.
Identifying factors that actually in¬
crease the risk could help us to pin¬
point those children of alcoholics who
are most likely to become alcoholic
themselves and to develop more effec¬
tive and specific prevention ap¬
proaches. Similarly, understanding
more about factors influencing the
development of alcoholism might help
clinicians to discover more effective
treatment approaches.
This work was supported by grant PHS
AA05526-03 from the National Institute on Alco¬
hol Abuse and Alcoholism, by the Veterans
Administration Research Service, and by a grant
from the Joan B. Kroc Foundation.
Thanks to Eric Gold, Karen Croot, and Chey-vonne
Frontiero for their devotion to excellence
in the series of studies reported herein.
References
1. Schuckit MA: The epidemiology of alcohol-ism,
in Schuckit MA (ed): Alcohol Patterns and
Problems, Series in Psychosocial Epidemiology.
New Brunswick, NJ, Rutgers Press, 1985, vol 5,
pp 1-42.
2. Robins LN, et al: Lifetime prevalence of
specific psychiatric disorders in sites. Arch Gen
Psychiatry 1984;41:949-958.
3. Cotton NS: The familial incidence of alco-holism:
A review. J Stud Alcohol 1979;40:89-116.
4. Gurling HM: Genetic epidemiology in medi-cine
p=m-recenttwin research. Br Med J 1984;
288:3-5.
5. Schuckit MA: Twin studies on substance
abuse: An overview, in Gedda L, Parisi P, Nance
W (eds): Twin Research: 3. Epidemiological and
Clinical Studies. New York, Alan R Liss Inc,
1981.
6. Goodwin DW, Schulsinger F, Moller N, et
al: Drinking problems in adopted and non-adopted
sons of alcoholics. Arch Gen Psychiatry
1974;31:164-169.
7. Bohman M, Sigvardsson S, Cloninger R:
Material inheritance of alcohol abuse. Arch Gen
Psychiatry 1981;38:965-969.
8. Schuckit MA: Studies of populations at high
risk for alcoholism. Psychiatr Dev 1985;3:31-63.
9. Begleiter H, Porjesz B, Bihari B, et al:
Event-related brain potentials in boys at risk for
alcoholism. Science 1984;225:1493-1495.
10. Schaeffer KW, Parsons OQ, Yohman JR:
Neuropsychological differences between male
familial and nonfamilial alcoholics and nonalco-holics.
Alcoholism Clin Exp Res 1984;8:347-358.
11. Hedegus AM, Alterman AI, Tarter RE:
Learning achievement in sons of alcoholics.
Alcoholism Clin Exp Res 1984;8:330-333.
12. Lipscomb TR, Nathan PE: Blood alcohol
level discrimination: The effects of family his-tory
and alcoholism, drinking pattern, and toler-ance.
Arch Gen Psychiatry 1980;37:571-576.
13. Schuckit MA: Subjective responses to alco-hol
in sons of alcoholics and controls. Arch Gen
Psychiatry 1984;41:879-884.
14. O'Malley SS, Maisto SA: The effects of
family drinking history on responses to alcohol:
Expectancies and reactions to intoxication. J
Stud Alcohol 1985;46:289-297.
15. Mednick SA: Subjects at risk for alcohol-ism:
Recent reports. Presented at the 14th
Annual Medical Conference Scientific Confer-ence
of the National Alcoholism Forum (Re-search
Society on Alcoholism), Houston, April 4,
1983.
16. Schuckit MA: Ethanol-induced changes in
body sway in men at high alcoholism risk. Arch
Gen Psychiatry 1985;42:375-379.
17. Schuckit MA, Parker DC, Rossman LR:
Ethanol-related prolactin responses and risk for
alcoholism. Biol Psychiatry 1983;18:1153-1159.
18. Schuckit MA: Differences in plasma corti-sol
after ingestion of ethanol in relatives of
alcoholics and controls: Preliminary results. J
Clin Psychiatry 1984;45:374-376.
19. Propping P, Kruger J, Mark N: Genetic
disposition to alcoholism: An EEG study in
alcoholics and their relatives. Hum Genet 1981;
59:51-59.
20. Pollock VE, Volavka J, Goodwin DW, et al:
The EEG after alcohol administration in men at
risk for alcoholism. Arch Gen Psychiatry 1983;
40:857-861.
21. Schuckit MA, Engstrom D, Alpert R, et al:
Differences in muscle-tension response to etha-nol
in young men with and without family
histories of alcoholism. J Stud Alcohol 1981;
42:918-924.
22. Schuckit MA: Peak blood alcohol levels in
men at high risk for the future development of
alcoholism. Alcoholism Clin Exp Res 1981;5:64x=req-
66.
23. Eriksson CJ: Human blood acetaldehyde
concentration during ethanol oxidation (update,
1982). Pharmacol Biochem Behav 1983;18:141x=req-
150.
24. Behar D, Berg CJ, Rapoport JL: Behavioral
and physiological effects of ethanol in high-risk
and control children: A pilot study. Alcoholism
Clin Exp Res 1983;7:404-410.
25. Schuckit MA, Rayses V: Ethanol ingestion:
Differences in blood acetaldehyde concentra-tions
in relatives of alcoholics and controls.
Science 1979;203:54-55.
26. Zeiner AR, Krug R, Kegg P, et al: Cardio-vascular
and pharmacokinetic effects of ethanol
in offspring of alcoholics and social drinkers.
Presented at the 20th International Congress of
Applied Psychology, Edinburgh, Scotland, July
12, 1982.
27. Ward K, Weir DG, McCrodden JM, et al:
Blood acetaldehyde levels in relatives of alcohol-ics
following ethanol ingestion. ICRS Med Sci
1983;11:950.
28. Saunders GR, Schuckit MA: Brief commu-nication:
MMPI scores in young men with alco-holic
relatives and controls. J Nerv Ment Dis
1981;168:456-458.
29. Schuckit MA: Anxiety and assertiveness in
the relatives of alcoholics and controls. J Clin
Psychiatry 1982;43:238-239.
30. Schuckit MA: Extroversion and neuroti-cism
in young men. Am J Psychiatry 1983;
140:1223-1224.
31. Morrison C, Schuckit MA: Locus of control
in young men with alcoholic relatives and con-trols.
J Clin Psychiatry 1983;44:306-307.
32. MacAndrew C: On the possibility of the
psychometric detection of persons who are prone
to the abuse of alcohol and other substances.
Addict Behav 1979;4:11-20.
33. Goodwin DW, Schulsinger F, Hermansen
L, et al: Alcoholism and the hyperactive child
syndrome. J Nerv Ment Dis 1975;160:349-353.
34. Vaillant GE, Milofsky ES: The etiology of
alcoholism: A prospective viewpoint. Am Psychol
1982;37:494-502.
35. Schuckit MA: Genetic and biochemical
factors in the etiology of alcoholism, in Grin-spoon
L (ed): Psychiatry Update. Washington,
DC, American Psychiatric Press Inc, 1984, vol 3,
pp 320-327.
36. Schuckit MA: Drug and Alcohol Abuse: A
Clinical Guide to Diagnosis and Treatment. New
York, Plenum Publishing Corp, 1984.
37. Schuckit MA: Alcoholism and other psy-chiatric
disorders. Hosp Community Psychiatry
1983;34:1022-1027.
Downloaded from jama.ama-assn.org at Mt Sinai School Of Medicine on April 23, 2012