Nephrotic syndrome IN CHILDREN Lecture for MBBS
•Als PPT, PDF herunterladen•
43 gefällt mir•8,287 views

Nephrotic syndrome IN CHILDREN FOR UNDER GRADUATES

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Nephrotic syndrome IN CHILDREN Lecture for MBBS
Ähnlich wie Nephrotic syndrome IN CHILDREN Lecture for MBBS (20)
Mehr von Sajjad Sabir
Mehr von Sajjad Sabir (11)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Nephrotic syndrome IN CHILDREN Lecture for MBBS
- 3. Dr. Muhammad Sajjad Sabir MBBS, DCH, MCPS, FCPS Assistant Professor of Paediatrics
- 4. Manifestation of glomerular disease, characterized by nephrotic range proteinuria and a triad of clinical findings associated with large urinary losses of protein : hypoalbuminaemia , edema and hyperlipidemia
- 5. Edema Heavy proteinuria > 40mg/m2/hr Hypoalbuminemia <2.5g/dl Hyperlipidema >250mg/dl
- 6. 15 x more common in children than adults 2 – 7 cases / 100,000 children / year (Global) Incidence South Asia 16/100,000 children Most common= 1.5 - 6 year boys : girls --- 2:1
- 7. Defined as Protein excretion of > 40 mg/m2 /hr (>1g/m2 /24 hr) Spot Protein : Creatinine > 2-3 : 1 (First morning urine sample) - Nelson Textbook of Paediatrics, Vol 2, 19th Edition, page 1801
- 9. Minimal Change disease ( >80 % ) Mesangial proliferation Focal segmental Glomerulosclerosis Membranous Nephropathy Membranoproliferative glomerulonephritis - Nelson Textbook of Paediatrics, Vol 2, 19th Edition, page 1804
- 10. Finnish type Cong. Nephrotic Syndrome Focal Segmental Glomerulosclerosis Diffuse Mesangial Sclerosis Denys-Drash Syndrome- Nelson Textbook of Paediatrics, Vol 2, 19th edition, page 1802, table 521-1
- 11. Congenital--Oligomeganephronia Infectious--Hepatitis (B,C) , HIV-1, Malaria, Syphilis, Toxoplasmosis Inflammatory--Glomerulonephritis Immunological--Castleman Disease,Bee sting, Food allergens Neoplastic--Lymphoma, Leukemia Traumatic ( Drug induced )--Penicillamine, Gold, NSAIDS, Pamidronate, Mercury, Lithium
- 13. Preceding flu-like illness General health (anorexia, weight gain ,lethargy) Edema Urinary symptoms (hematuria, oliguria) Infection, diarrhea, abd. pain Drug intake Past history
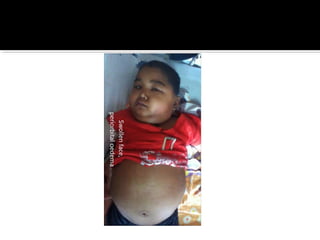
- 15. Edema Mild early – periorbital puffiness, lower extremities Progression to gen. edema, ascites, pleural effusion, genital edema Decreased urine output Anorexia, Irritability, Abdominal pain and diarrhoea Vital & BP Height & weight for age Anemia - Nelson Textbook of Paediatrics, Vol 2, 19th Edition, page 1802 Clinical Features-Examination No Hypertension No Gross hematuria
- 16. CLINICAL FEATURES Minimal Change Nephrotic Syndrome Focal Segmental Glomerulosclerosis Membranous Nephropathy Age ( yr ) 2 - 6 2 - 10 40 - 50 Sex ( M : F ) 2 : 1 1.3 : 1 2 : 1 Nephrotic Syndrome 100 % 90 % 80 % Asymptomatic proteinuria 0% 10 % 20 % Hematuria 10 – 20 % 60 – 80 % 60 % Hypertension 10 % 20 % early Infrequent Rate of progression to renal failure Non progressive 10 yrs 50 % in 10 – 20 yrs Associated Conditions Usually none None Renal vein thrombosis, SLE, Hepatitis B
- 17. URINE ANALYSIS PROTEINURIA: 3+ Or 4+ MICROSCOPIC HEMATURIA: 20% PUS CELLS: underlying UTI CELLULAR CASTS: not in minimal change disease Trace /nil (10-20mg/dl) + (30mg/dl) ++ (100mg/dl) +++(300mg/dl) ++++(1000-2000mg/dl)
- 18. 24HRS URINARY PROTEIN EXCRETION: Children : >40mg/m2/hr (>1g/m2 /24 hr) URINARY spot PROTEIN : CREATININE > 2.0 (Spot UPC ratio > 2.0)
- 19. SERUM S. CREATININE: Normal S. CHOLESTROL: ↑ >250mg/dl S. ALBUMIN: <2.5g/dl C3 & C4: Normal TOTAL CALCIUM: Decreased
- 20. VITRAL SEROLOGY: HBV associated with membranous nephritis BLOOD COUNTS: Hb, TLC & DLC Normal ESR raised X-RAY CHEST: R/O pulmonary TB R/O pleural effusion
- 21. MANTOUX TEST: R/O TB before starting steroids ANA: R/O SLE • Age below 12 months • Gross or persistent microscopic hematuria • Low blood C3 • Hypertension • Impaired renal Function • Failure of steroid therapy Indications for Renal biopsyIndications for Renal biopsy
- 22. Protein losing enteropathy Hepatic failure Heart failure Acute/Chronic Glomerulonephritis Protein Malnutrition
- 23. Other forms of glomerulonephritis Pyelonephritis Obstructive Uropathies Hemolytic Uremic Syndrome Fever Exercise Orthostatic proteinurea Renal Failure Congestive cardiac failure Liver failure
- 24. Management
- 25. DIETARY ADVICE: Balanced diet = adequate proteins & calories Foods high in sodium avoided High protein diet Edema no added salt Treatment of infections Parent Education Can attend school Can participate in physical activities as tolerated
- 26. If significant edema Diuretics + Aldosterone antagonist ( Fursemide, spironolactone ) Salt restriction DIURETICS INDICATIONS: Severe symptomatic edema Steroid toxicity or steroid contraindicated Q.Best diuretic in Nephrotic Syndrome?
- 27. ROLE OF INTRAVENOUS ALBUMIN INDICATIONS: Signs of hypovolemia Sever oedema DOSAGE & ADMINISTRATION: I/V salt poor 25% albumin infusion 0.5-1 gm/kg/dose over 6-12 hrs + I/V Frusemide 1-2 mg/kg
- 28. DOSAGE & ADMINISTRATION:(after a -ve PPD test) Prednisolone 60mg/m2 /day (max 80mg) As single am daily dose {or 2-3 dd} for 6 wks After the initial 6-wk course, Prednisone dose tapered to 40 mg/m2 /day given every other day as a single daily dose for at least 6 wk. Alternate-day dose then slowly tapered→discontinued over next 1-2 mo
- 29. Response means Clinical remission Diuresis , and Urine trace or negative for protein for 3 consecutive days
- 30. REPONSE TO STEROID: 80-90% children respond within 3 wk 10% respond by first week 70% by second week 85% by third week 92% by forth week Who respond to prednisone therapy do so within first 5 wk of treatment
- 31. STEROID DEPENDENT: Patients who relapse while on alternate-day steroid therapy or within 28 days of completing a successful course of prednisone therapy FREQUENT RELAPSERS: Patients who respond well to prednisone therapy but relapse ≥ 4 times in a 12-mo period INFREQUENT RELAPSERS :3 or less relapses per yr STEROID RESISTANT: Fail to respond to corticosteroid therapy within 8 wks Children who continue to have proteinuria (2+ or greater) Diagnostic renal biopsy should be performed
- 32. Relapses should be treated with: Prednisone 60 mg/m2 /day (80 mg daily max) As single am dose Until child enters remission (urine trace or negative for protein for 3 consecutive days) Then prednisone changed to alternate-day (40 mg/m2 /day ) Gradually tapered over 4-8 wk
- 33. ALTERNATIVE THERAPY: INDICATIONS: Steroid dependent Frequent relapsers Steroid responsive Unwanted effects of steroids
- 34. Alternate Day prednisolone Steroid sparing agents Levamisole ( 2 – 2.5 mg/kg ) Cyclophosphamide ( 2 – 2.5 mg/kg/day) Mycophenolate Mofetil (20 – 25 mg/kg/day) Cyclosporin ( 4 – 5 mg/kg/day ) Tacrolimus (0.1 – 0.2 mg/kg/day ) Rituximab ( 375mg/m2 IV once a week )
- 35. INFECTIONS: SBP Pneumonia Cellulitis UTI Disseminated varicella THROMBOEMBOLISM: Renal vein thrombosis Pulmonary embolism Saggital sinus thrombosis OTHERS: Acute renal failure Hypertension Malnutrition Flare up of tuberculosis Steroid & drug related toxicity
- 36. Blood CP Urine RE Growth parameters General examination Blood Pressure Eye examination RFTs Serum electrolytes BSR Serum calcium X-Ray wrist X-Ray spine Chest X-Ray PT/APTT
- 37. Steroid Responsive NS : Good prognosis ( MCNS ) Steroid Resistant NS : Poor prognosis ( FSGS ) Mortality rate 1-2 % - Nelson Textbook of Paediatrics, Vol 2, 19th Edition, page 1806
- 38. DEFINITION: Infants who develop nephrotic syndrome within first 3 months of life ETIOLOGY: Finish type congenital nephrotic syndrome Congenital infections HIV/HBV Diffused mesengial sclerosis Drash syndrome
- 39. TREATMENT: ACE inhibitors + Indomethacin + unilateral neprectomy B/L nephrectomy →Chronic dialysis & Renal transplant no role of steroid or immunosuppressive agents PROGNOSIS: Poor Progressive renal failure Death by 5 yrs age if untreated