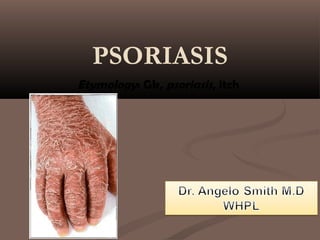
2. ■Psoriasis is a disease which
affects the skin is a disease which
affects the skin and joints.
3. ■ It commonly causes red
scaly patches to appear on
the skin.
■ The scaly patches caused
by psoriasis, called
psoriatic plaques, are
areas of inflammation
and excessive skin
production.
■ Skin rapidly accumulates
at these sites and takes a
silvery-white appearance.
■ Plaques frequently occur
on the skin of the elbows
and knees, but can affect
any area including the
4. ■ Psoriasis is an inflammatory skin disease in which skin cells replicate
at an extremely rapid rate. New skin cells are produced about eight
times faster than normal--over several days instead of a month--but
the rate at which old cells slough off is unchanged.
■ This causes cells to build up on the skin's surface, forming thick
patches, or plaques, of red sores (lesions) covered with flaky, silvery-
white dead skin cells (scales).
5. ■ The disorder is a chronic recurring
condition which varies in severity from
minor localized patches to complete body
coverage.
■ Fingernails and toenails are frequently
affected (psoriatic nail dystrophy).
■ Psoriasis can also cause inflammation of
the joints, which is known as psoriatic
arthritis.
6. Genetics
■Psoriasis was present in 73% of monozygotic
twins compared with 20% in dizygotic twins.
■When both parents are affected by psoriasis, the
rate in siblings is as high as 50%.
■When one parent is affected, the rate is 16.4%
■ When neither parent has psoriasis, only 7.8% of
siblings of probands are affected
■Other studies have shown that 36-71% of
patients with psoriasis have one relative who is
also affected by psoriasis
7. Exacerbating Factors
■Local factors
■ Trauma: e g, physical, chemical, electrical,
surgical, infective, and inflammatory types of
injury or even excessive scratching can
aggravate or precipitate localized psoriasis
(Koebner reaction)
■Sunlight: Most patients generally consider
sunlight to be beneficial for their psoriasis. Most
report a decrease in illness severity during the
summer months or periods of increased sun
exposure; however, a small minority find that
their symptoms are aggravated by strong
sunlight.
8. ■Systemic factors
■Infection: Pharyngeal streptococcal infections
have been shown to produce guttate psoriasis.
Some evidence suggests that subclinical
streptococcal colonization or overgrowth could
be responsible for refractory plaque psoriasis.
An increase in psoriasis activity was observed
in HIV infected patients.
■Drugs: Some drugs cause an exacerbation of
psoriasis. Lithium and withdrawal from systemic
corticosteroids are well known to cause flares
of disease. Beta-blockers, antimalarials, and
nonsteroidal anti-inflammatory drugs (NSAIDs)
have also been implicated.
9. ■Psychogenic/emotional factors: Many
patients report an increase in
psoriasis severity with psychological
stress.
■A clear cause-and-effect
relationship between disease
exacerbation and stress
unfortunately has not been proven
but, pruritus associated with
increased anxiety or depression
may promote scratching and a
Koebner reaction.
10. ■Smoking: An increased risk of chronic
plaque psoriasis exists in smokers
■Alcohol: Alcohol is considered a risk
factor for psoriasis
■Endocrine: Psoriasis severity has been
noted to fluctuate with hormonal changes.
■Disease incidence peaks at puberty and
during menopause.
■Pregnant patients' symptoms are more
likely to improve than worsen.
■In contrast, the disease is more likely to
flare in the postpartum period
11.
12. HYPOTHESIS
■two main
■The first considers psoriasis as primarily
a disorder of excessive growth and
reproduction of skin cells.
■The problem is simply seen as a fault
of the epidermis and its keratinocytes.
13. ■ The second hypothesis sees the disease as being an
immune-mediated disorder
■ The second hypothesis sees the disease as being an
immune-mediated disorder in which the excessive
reproduction of skin cells is secondary to factors
produced by the immune system. T cells (which
normally help protect the body against infection)
become active, migrate to the dermis and trigger the
release of cytokines (tumor necrosis factor-alpha
TNFα, in particular) which cause inflammation and
the rapid production of skin cells. It is not known
what initiates the activation of the T cells.
■ The immune-mediated model of psoriasis has been
supported by the observation that immunosuppressant
medications can clear psoriasis plaques.
21. 21
Psoriasis: Clinical Presentation
Type Characteristics
Plaque psoriasis
Guttate psoriasis
Erythrodermic
psoriasis
Pustular
psoriasis
Nail psoriasis
Palmar/Plantar
psoriasis
Psoriatic arthritis
Scalp psoriasis
Dry scaling patches (AKA common psoriasis) 75%
Drop-like dots, occurs after strep or viral infection 12%
Exfoliation of fine scales (total body “dandruff”),
widespread, often accompanied by severe itching and
pain 7%
Pus-like blisters, noninfectious, fluid contains white blood
cells 2%
Seen on toenails and fingernails, starts as numerous pits,
at times progresses to yellowing, crumbly, and thickened
nail; nails may slough
Erythema, thickening and peeling of the skin, blistering is
often present. Can lead to disability.
Inflammation, swelling, and joint destruction
Plaque-type lesion
22.
23. ■ Plaque psoriasis (psoriasis vulgaris) is the
most common form of psoriasis. It affects 80 to
90% of people with psoriasis. Plaque psoriasis
typically appears as raised areas of inflamed skin
covered with silvery white scaly skin. These areas
are called plaques.
27. ■Guttate psoriasis is characterized by numerous
small oval (Gutta - teardrop-shaped) spots.
These numerous spots of psoriasis appear over
large areas of the body, such as the trunk, limbs,
and scalp.
■Guttate psoriasis is associated with
streptococcal throat infection
29. ■ Erythrodermic psoriasis
involves the widespread
inflammation and exfoliation of
the skin over most of the body
surface. It may be accompanied
by severe itching, swelling and
pain.
■ It is often the result of an
exacerbation of unstable plaque
psoriasis, particularly following
the abrupt withdrawal of
systemic treatment.
■ This form of psoriasis can be
fatal, as the extreme
inflammation and exfoliation
disrupt the body's ability to
regulate temperature and for the
skin to perform barrier
functions.
30.
31. ■ Pustular psoriasis appears as raised bumps that
are filled with non-infectious pus (pustules).
■ The skin under and surrounding pustules is
red and tender.
■ localized - hands and feet ,
■ generalized and randomly on any part of the
body.
33. Generalized pustular psoriasis (von
Zumbusch type)
■It is usually preceded by other
forms of the disease
■The disease occurs as attacks
characterized by fever that lasts
several days and a sudden
generalized eruption of sterile
pustules 2 to 3 mm in diameter
34. ■The pustules are disseminated over the trunk and
extremities, including the nail beds, palms, and soles
■The pustules usually arise on highly erythematous skin,
first as patches and then becoming confluent as the
disease becomes more severe
35. Annular Pustular Psoriasis
■It is a rare variant of pustular
psoriasis
■Lesions may appear at the
onset of pustular psoriasis,
with a tendency to spread
and form enlarged rings, or
they may develop during the
course of generalized
pustular psoriasis
■The characteristic features
are pustules on a ring-like
erythema
36. Impetigo Herpetiformis
■ lesions are identical to annular pustular psoriasis but occur
during pregnancy
■ Onset is usually early in the third trimester and persists until
delivery
■ It tends to develop earlier in subsequent pregnancies
■ It is often associated with hypocalcemia
■ There is usually no personal or family history of psoriasis
37. Acrodermatitis Continua
of Hallopeau
■It is rare
■sterile, pustular eruption of the
fingers or toes slowly extends
proximally
■Continuous pustulation leads
to nail destruction and atrophy
of the distal phalanx
39. ■ In 78% of psoriatic patients
■ Fingernails>Toenails
■ Six changes
1. Onycholysis (= separation from nail bed)
and crumbling of the nail
2. Pitting*
3. Subungual debris accumulation
4. Color alterations
5. Thickening of skin under the nails
6. Beau’s Lines going across the nails
*Pitting rules out a fungal infection
43. ■ Flexural psoriasis (inverse psoriasis) appears as
smooth inflamed patches of skin. It occurs in skin folds,
particularly around the genitals (between the thigh and
groin), the armpits, under an overweight stomach
(pannus), and under the breasts (inframammary fold).
■ It is aggravated by friction and sweat, and is vulnerable
to fungal infections.
44. ■ Psoriatic arthritis involves joint and connective tissue
inflammation.
■ Psoriatic arthritis can affect any joint but is most common in the
joints of the fingers and toes.
■ This can result in a sausage-shaped swelling of the fingers and
toes known as dactylitis. Psoriatic arthritis can also affect the hips,
knees and spine (spondylitis).
■ About 10-15% of people who have psoriasis also have psoriatic
arthritis.
45. ■In 10-20% of psoriasis patients
■Distal inter phalangeal joints
■No elevated serum levels of
rheumatoid factors (as seen in
rheumatoid arthritis, yet has all other
features)
■Often seen in patients with nail and
scalp psoriasis
46. ■ Enthesitis(inflammation of the insertion points of tendons
and joints into bone)
■ Periosteal new bone formation
■ Asymmetric oligoarthritis &
spondylitis
•The blue arrow = a normal joint space
• Red arrow = “cup and saucer” effect of the fourth
metatarsal bone being jammed into the base of the
fourth toe
•The yellow circle = “Pencil appearance”destruction
characteristic of the disease
47. Sebopsoriasis
■ It is a common clinical entity
■ It presents with erythematous plaques with greasy yellow scales
localized to seborrheic areas (scalp, glabella, nasolabial folds,
perioral and presternal areas, and intertriginous areas)
■ In the absence of typical findings of psoriasis elsewhere, distinction
from seborrheic dermatitis is difficult
■ It may represent a modification of seborrheic dermatitis by the
genetic background of psoriasis
50. Napkin psoriasis
■Usually begins between the
ages of 3 and 6 months
■First appears in the napkin
areas as a confluent red area
with appearance a few days
later of small red papules on
the trunk that may also involve
the limbs
■These papules have the
typical white scales of
psoriasis
51. Geographic tongue
■Presents as asymptomatic erythematous
patches with serpiginous
borders, resembling a map
■The lesions have a migratory
character
■It has been postulated to be an oral variant of
psoriasis, as these lesions show several
histologic features of psoriasis.
■However, geographic tongue is a relatively
common condition and is seen in many
nonpsoriatic individuals
52.
53. -Auspitz sign(Grattage
test): Removing the
scale reveals a smooth,
red, glossy membrane
with tiny punctate
bleeding points.
These points represent
bleeding from enlarged
dermal capillaries after
removal of the
overlying epithelium
54. -Rich red color:often referred to as 'salmon pink‘.
This quality of color is of special diagnostic value to
differentiate psoriasis from eczema in lesions on the
palms, soles and scalp.
In the fair-skinned individual, the color is less rich and
almost magenta pink.
In dark-skinned races, the quality of the color is lost
55.
56.
57. PASI Score
(Psoriasis Area and Severity
Index)
■It is a method to estimate severity of psoriasis in
order to evaluate the clinical efficacy of new
treatments
■Psoriatic plaques are graded based on three
criteria: redness (R), thickness (T), and scaliness
(S)
■Severity is rated on a 0-4 scale (0 for no
involvement up to 4 for severe involvement)
■The highest PASI score is 12; the lowest is 0
64. ■ Coal Tar
■ Prefered for limited or scalp psoriasis.
■ In 1925, Goeckerman introduced “The
Goekerman technique” which uses crude coal
tar and UV light for the treatment of psoriasis
■ Can be effective in widespread psoriasis
■ Antimitotic, anti-pruritic
■ No quick onset but longer remission
■ Often combined with SA, UV light therapy
■ 2 types: Crude coal tar and Liquor picis carbonis
65. ■Coal tar, in concentrations 5- 20% can be
compounded in creams, ointments,
shampoos and and pastes
■It is often combined with salicylic acid (2-
5% ), which by its keratolytic action leads to
better absorption of the coal tar
■Disadvantages include: allergic
reactions, folliculitis, it has an unwelcome
smell and appearance and can stain
clothing and other items. Coal tar is
carcinogenic
66. Dithranol
■ May restore normal epidermal proliferation and
keratinization
■ Useful in thick plaque psoriasis
■ Commonly used with SA
■ 2 treatment approach: long contact and short
contact
■ Stains clothes, irritating to normal skin
67. Vitamin D Analogues
Calcipotriene (calcipotriol)”Betdaivonex”
■Potent topical corticosteroids are superior to
calcipotriene. But calcipotriene was more effective than
coal tar or anthralin
■The efficacy of calcipotriene is not reduced with long-
term treatment
■Calcipotriene is applied twice daily
■Salicylic acid inactivates calcipotriene
■It is often used in combination with or in rotation with
topical corticosteroids in an effort to maximize
therapeutic effectiveness while minimizing steroid-related
skin atrophy.
■In view of their efficacy, cosmetic acceptability and
relative safety, they may accepted as first-choice
therapies in the topical treatment of mild to moderate
psoriasis, although cost may be a problem
68. Topical CS
■ Anti-inflammatory, immunosuppressive
■ Quick onset than coal tar and dithranol
■ Tachyphylaxis can occur
■ High potent agents used in severe cases, thick
plaques
■ AE local and systemic
■ Should not be stopped abruptly – rebound
psoriasis
69. Phototherapy
■ UVA, UVB, PUVA
■ UVB prefered
■ Administered by lamp, sunlight exposure alone
or in combo with another topical agent
■ PUVA (methoxsalen) given PO 2 hours before
UVA or lotion applied 30mins before exposure
■ AE: itch, edema
71. Determination of the minimal
erythema dose (MED)
1-The patient wears a
thick cotton shirt which
has 10 small, vertical
holes on its back
2-The patient is
exposed to 50 mj of UV
on the back while all
the holes are opened
72. 3-The first hole is closed and another exposure is
given By that time the skin under the first hole was
exposed to 50 mj of UV while the skin under the
second hole was exposed to 100 mj
4-The second hole is closed and the procedure is
repeated in the same way (closing an hole and giving
a dose) for all the holes
5-After 24-72 hours the skin of the back is examined
and the first skin area showing well-defined erythema
is determined and the amount of UV causing it is
called "the minimal erythema dose"
73. Dosing
NB-UVB PUVA Excimer laser
•Initial dose at
50% of MED
followed by 3
treatments /w
•Lubricate before
ttt
•Increase dose
by at least 10-20%
of the MED
•Initial dose 0.5-2.0
J/cm2
, depending on
skin type followed by
twice weekly
•Increase dose by
40% per week until
erythema, then
maximum 20% per
week until a
maximum of 15 J/cm2
•2-6 MED twice
weekly
•NB-UVB=Narrow-band Ultraviolet B (Wave length 310-331 nm)
•PUVA=Psoralen +ultraviolet A (Wave length 315–380 nm)
• Excimer laser (Wave length 308 nm)
74. Efficacy
NB-UVB PUVA Excimer laser
> 70%
improvement
study after 4 wk
of treatment
Induces
remission in
70%-90% of
patients
75%
improvement in
72% of patients
in an average of
6.2 treatments
75. Side Effects
NB-UVB PUVA Excimer laser
•Photodamage
•Polymorphic
light eruption
•Increased risk
of skin aging
and skin cancer
Similar to NB-
UVB but the
risk is higher
Erythema,
blisters,
hyperpigmentati
on, and
erosions
78. ■ Systemic agents are generally recommended for
patients with moderate-to-severe disease.
■ Moderate disease is defined as greater than 5%
body-surface area involvement; severe disease is
defined by greater than 10%
79. Efficacy
Cyclosporin A Methotrexate Acitretin
Up to 90% of
patients achieve
clearance or
marked
improvement
May reduce the
severity of
psoriasis by at
least 50% in
more than 75%
of patients
Modestly
effective as
monotherapy
80. Side effects
Cyclosporin A Methotrexate Acitretin
•Nephrotoxicity
•Hypertension
•Immuno-
suppression
•Neurotoxicity
•Increased risk
of malignancy
•Chronic use
may lead to
hepatic fibrosis
•Fetal abnorma-
lities or death
•Myelosupp-
ression
•Pulmonary
fibrosis
•Hepatotoxicity
•Lipid
abnormalities
•Fetal abnorma-
lities or death
•Alopecia,
mucocutaneous
toxicity
•Hyperostosis
81. Monitoring
Cyclosporin A Methotrexate Acitretin
•BP
•Baseline CBC
•CMP, Mg, uric
acid, lipids,
urinalysis
Repeat tests
every 2-4 wk,
then every
month along
with BP
•Baseline CBC,
CMP, LFTs
Repeat baseline
tests weekly
during dose
escalation, then
every 2 wk. Hold if
WBC ≤ 4.0 ×109
/L,
platelet count is <
125 × 109
/L, or Hg
< 110 g/L
•Baseline CBC
and CMP
Repeat
laboratory tests
weekly × 6 wk,
then every 2
wk × 2 mo, and
then monthly.
Monitor BP
Cyclosporin A Methotrexate Acitretin
•BP
•Baseline CBC
•CMP, Mg, uric
acid, lipids,
urinalysis
Repeat tests
every 2-4 wk,
then every
month along
with BP
•Baseline CBC,
CMP, LFTs
Repeat baseline
tests weekly
during dose
escalation, then
every 2 wk. Hold if
WBC ≤ 4.0 ×109
/L,
platelet count is <
125 × 109
/L, or Hg
< 110 g/L
•Baseline CBC
and CMP
Repeat
laboratory tests
weekly × 6 wk,
then every 2
wk × 2 mo, and
then monthly.
Monitor BP
82. Contraindications
Cyclosporin A Methotrexate Acitretin
Absolute:
•Prior bone
marrow
depression
•Pregnancy
•Lactation
Relative:
Renal
abnormalities
Absolute:
•Inherited
deficiency of
thiopurine
methyltransferase
enzyme due to
increased risk of
myelosuppression
• Liver toxicity
• Pregnancy
Absolute:
•Severe
infections
•Malignancy
83. Use in Pregnancy
Cyclosporin A Methotrexate Acitretin
C category
Studies on animals
revealed teratogenic
or embryocidal
effects and there
are no controlled
studies in women
It should be given
only if the potential
benefit justifies the
potential risk to the
fetus
D category
There is positive
evidence of human
fetal risk, but the
benefits from use in
pregnant women
may be acceptable
despite the risk
(e.g., if the drug is
needed in a life-
threatening
situation)
X category
The drug is
contraindicated in
women who are
or may become
pregnant
84. ■ Psoriasis is a lifelong condition.
■ There is currently no cure but various treatments can
help to control the symptoms. Many of the most
effective agents used to treat severe psoriasis carry an
increased risk of significant morbidity including skin
cancers, lymphoma and liver disease.
■ Psoriasis does get worse over time but it is not possible
to predict who will go on to develop extensive psoriasis
or those in whom the disease may appear to vanish.
■ Individuals will often experience flares and remissions
throughout their lives. Controlling the signs and
symptoms typically requires lifelong therapy.
Summary
Hinweis der Redaktion
Normal layers on the left
Psoriasis on the right where the stratum corneum is disorganized, cracked and flaky/ the stratum granulosum has thickened and has tremendous neutrophil accumulation/ the stratum spinosum has many immature cells and is thicker
This is a picture of guttate (shaped like a drop) psoriasis on the arms and chest. Guttate psoriasis is a rare form of psoriasis. It frequently follows a streptococcal infection, appears rapidly and affects the face, chest (trunk) and nearest (proximal) limbs. The patches are small and round or oval and have the typical appearance of psoriasis. It is seen almost exclusively in children. This photograph shows the diffuse and widespread coverage on the arm and chest.
Plaque type psoriasis on knuckles with nail changes
Also at the cuticle and distal nail (ungulus)