Occupational Liver Disorders
•Als PPTX, PDF herunterladen•
13 gefällt mir•6,041 views

liver disorders related to work

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Occupational Liver Disorders
Ähnlich wie Occupational Liver Disorders (20)
Mehr von Dalia El-Shafei
Mehr von Dalia El-Shafei (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Occupational Liver Disorders
- 1. OCCUPATIONAL LIVER DISORDERS Dr. Dalia Abdallah El-Shafei Lecturer, Community medicine department, Zagazig University
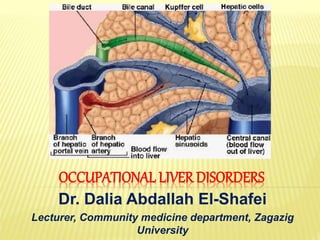
- 2. Zone 1 (Periportal lobule): nearest the portal vein. Zone 2 (Midzonal region): intermediate to the final region of liver. Zone 3 (Centrilobular area): adjacent to the central vein.
- 3. Viral hepatitis Physical agent- induced Chemical- induced 1-Similarity of presenting symptoms (acute toxic liver disorders frequently with nonspecific clinical manifestations 2-Chronic liver injury usually are asymptomatic until its end stage 3-Simultaneous conditions (viral hepatitis and/or alcohol & drug abuse) confound liver disorders caused by specific occupational or environmental hepatotoxins. 4-Host-susceptibility factors (genetic polymorphisms of metabolic & detoxifying enzymes)
- 4. SEROLOGIC MARKERS •Serologic viral markers & their antibodies & antigens. •Reveals cause & stage of disease Specific pathogens •Hepatic enzymes released into blood. •Indicates extent of hepatic injury Liver function
- 5. Cytotoxic hepatic injury (a) Less specific enz. reflecting injury to extrahepatic tissue (AST or SGOT & LDH) (b) Enzymes mainly in the liver (ALT or SGPT) (c) Very specific enz. to the liver (ornithine carbamyltransferase (OCT) & sorbitol dehydrogenase (SDH). Cholestatic injury - Alkaline phosphatase (AP) - 5'-nucleotidase (5'-NT) - γ-glutamyltranspeptidase (γ-GT) Serum alpha-fetoprotein is a well-established marker for hepatocellular carcinoma (low specificity) Serum enzymes generally only elevated with extrahepatic diseases as, creatine phosphokinase (CPK). Serologic Markers for Liver Function
- 8. INFLAMMATORY LIVER DISORDERS Predominate cause of liver-related morbidity The consequence of cumulative damage that leads to hepatocyte death and recruitment of inflammatory cells to sites of injury. Long-term conditions that may progress to cirrhosis & hepatic failure due to a lack of effective early diagnostic & treatment protocols. The primary causes: Viral: Hepatitis A,B,C,D,E, Yellow fever, Epstein-Barr virus, Cytomegalovirus, four exotic viruses (Ebola, Marburg, Lassa fever, and Rift Valley fever viruses), Herpes hominis, Rubella, Adenoviruses, and Enteroviruses. Other: Miliary tuberculosis, Malaria, Staphylococcal bacteremia, Salmonelloses, Candida, and amebiasis.
- 17. • More than 100 chemicals • Painting, Textile&Dye manufacturing • Arsphenamine, Carbon tetrachloride (CCl4), Trinitrotoluene (TNT), Dimethylnitrosamine (DMN), Chloroform & Polychlorinated biphenyls (PCB), Ethanol • Cooking oil heavily contaminated with PCBs (Japan, 1968), • Wheat with hexachlorobenzene (Turkey, 1955- 1957) • Flour with 4,4'diaminodiphenyl-methane (England, 1965)
- 18. Chemical Hepatotoxins Naturally occurring Bacterial toxins, Mycotoxins, Mushroom toxins & algae toxins. (aflatoxins, phalloidin, (& microcystin Synthetic Therapeutic drugs, Pesticides, Metals, Ethanol, & Industrial chemicals (aromatic hydrocarbons, halogenated hydrocarbons, chlorinated aromatic compounds, & nitro compounds)
- 20. MECHANISM OF TOXICITY Intrinsic toxin (Dose-dependent): Most hepatotoxins Direct hepatotoxins: - Direct physicochemical effect (peroxidation of membrane lipids or denaturation of protiens) leading to hepatocyte membrane destruction and distortion. - CCL4, Chloroform, CBr4, Trichloroethan,Tetrachloroethylene. - - Hepatotoxic potential of Haloalkans: - Inversely proportionate to chain length & bond energy. - Directly proportionate to no. of halogen atoms in molecule & atomic no. of halogen.
- 21. Indirect hepatotoxicity: - Interference with metabolic pathway Cytotoxic damage: Degeneration or Necrosis of hepatocytes by interfering with pathway necessary for structural integrity (steatosis or necrosis) - Botanicals (aflatoxin, tannic acid) & drugs (tetracycline, methotrexate) Cholestatic damage: interfering with bile secretion - Only one is MDA (Methylene dianiline)
- 22. Idiosyncratic toxin (Dose-independent): - Few hepatotoxins - e.g., Beryllium & Halothane - Sporadic liver injury, possibly due to a hypersensitivity or immunologic-type reaction.
- 24. CLINICAL SYNDROMES INDUCED BY CHEMICAL HEPATOTOXINS
- 26. Acute injury often results in an accumulation of lipids (Steatosis) & appearance of degenerative processes, leading to cell death (Necrosis). Necrotic process can affect small groups of isolated parenchymal cells (Focal necrosis), groups of cells located in zones (Centrilobular, Midzonal, or Periportal necrosis), or all cells within a hepatic lobule (Massive necrosis). ACUTE HEPATITIS
- 27. CHRONIC ACTIVE HEPATITIS Chronic active hepatitis (CAH),(chronic aggressive hepatitis), is one of the 3 major forms of chronic hepatitis. The other two forms, chronic persistent hepatitis (CPH) and chronic lobular hepatitis (CLH), are usually clinically mild and histologically nonprogressive and, therefore, are considered benign. CAH is frequently characterized by the development of symptoms and abnormality of liver function or histologic status with a high likelihood of progression to cirrhosis. Causes: Infections with HBV, HCV, and HDV; Drug-induced, Autoimmune reactions; Genetic metabolic disorders, & Occupational or environmental exposures to certain Hepatotoxins & Alcohol.
- 30. CHRONIC HEPATITIS 1. Cholestatic Injury 2. Fatty Liver (Steatosis) 3. Hepatoportal Sclerosis 4. Fulminant Hepatic Failure & Necrosis 5. Cirrhosis 6. Granulomatous Disease of the Liver 7. Porphyria Cutanea Tarda & Related Abnormalities
- 31. 1. CHOLESTATIC INJURY Diminution or cessation of bile flow and retention of bile salts & bilirubin. Clinical symptoms: Jaundice, abdominal pain, pruritus, & fever Rare but has been reported following exposure to the chemical Methylene Dianiline (MDA), an aromatic amine used as an epoxy resin hardener. Epping jaundice (1965): Epidemic of Acute Cholestatic Jaundice occurred in Epping, England, after bread was made from flour contaminated with MDA.
- 32. Chronic cholestatic liver disorder - The Spanish toxic oil syndrome (1981)associated with accidental high ingestion of denatured rapeseed oil. - Patient with severe muscle wasting accompanied by muscle and skin fibrosis, prominent features of the Spanish toxic oil syndrome. Epidemiologic studies demonstrated that affected subjects consumed a rapeseed oil containing fatty acid anilides. Oil from France that had been deliberately adulterated with aniline to prevent food use was illegally intercepted in Spain, heated to remove the aniline, and sold in and around Madrid in 1981.
- 33. 2. FATTY LIVER(STEATOSIS) Morphologically as greater than 5% of the hepatocytes containing fat or, Quantitatively, as greater than 5 g lipid per 100 g hepatic tissue. Also occurs in other disorders (DM, hypertriglyceridemia, & obesity). Some degree of steatosis is usually found accompanying acute hepatocellular necrosis; But, marked steatosis is more commonly seen in exposure to chronic hepatotoxins.
- 34. First described with Yellow Phosphorus poisoning. Chronic exposure to chlorinated solvents such as CCl4, methyl chloroform. Styrene, Toluene, Trichloroethane (TCE) & other aromatic compounds. TNT in munitions industries, Arsenical pesticide use in vintners. More subtle microsteatosis was described following short- term, low-level exposure to dimethylformamide (DMF) in a fabric-coating factory.
- 36. 3- HEPATOPORTALSCLEROSIS Rare form of noncirrhotic periportal fibrosis, which can lead to Portal Hypertension. Occupational exposure to the Vinyl Chloride Monomer (VCM) in Polyvinyl Chloride (PVC) polymerization plants, Inorganic Arsenicals, and Thorium compounds. Liver histology has shown hyperplasia of hepatocytes and sinusoidal cells, with dilatation of sinusoids and progressive subcapsular, portal, perisinusoidal, and occasionally, intralobular fibrosis, which is accompanied by portal hypertension and splenomegaly.
- 37. 4- FULMINANTHEPATIC FAILURE & NECROSIS Exposure to TNT (munitions manufacture during WWI & II). CCl4 , chloroform, TCE, & epoxy resin coating containing 2- nitropropane after inhalation exposure in an enclosed space. A severe liver disorder in which hepatic insufficiency progresses from the onset of symptoms to hepatic encephalopathy within 2 to 3 weeks, resulting in liver necrosis & liver failure. The symptoms included jaundice, hepatomegaly, and severe liver necrosis. Even people who survive the acute phases of the disease often later develop postnecrotic cirrhosis or aplastic anemia. Onset of symptoms developed 2 to 4 days after exposure, often accompanied by renal failure in severe cases. Those who survived the acute stages recovered in 2 to 4 weeks, but repeated subclinical exposure could induce cirrhosis.
- 38. 5- CIRRHOSIS A chronic, irreversible condition where the normal lobular architecture is replaced by fibrous tissue and regenerating nodules derived from the remaining hepatocytes. Mainly due to chronic viral infection & alcohol abuse Organic Solvents, Dimethylnitrosamine (DMN), TNT, TCE, pesticides, Arsenic , PCBs& Hydrazines. Cirrhosis & other liver disorders have been reported to be more prevalent among Anesthesiologists compared to other hospital personnel. Morticians exposed long term to formaldehyde had a greater prevalence of cirrhosis, although ethanol was a possible confounding factor.
- 39. 6- GRANULOMATOUSDISEASE OF THE LIVER Beryllium and Copper. In beryllium injury, the histopathologic appearance of the liver biopsy specimen can be indistinguishable from sarcoidosis. Berylliosis may include involve granulomas in the spleen, bone marrow, and lungs, as well as the usual granulomatous interstitial lung disease. Vineyard sprayer's lung were found to be associated with liver damage with inclusion of copper in biopsy tissue. The liver disorder included proliferation & swelling of the Kupffer cells, sarcoidlike granulomas, fibrosis, micronodular cirrhosis, hepatic angiosarcomas, & idiopathic portal hypertension.
- 40. The mildew of the vineyards is prevented by the use of sprays with a solution of Copper Sulphate neutralized with hydrated lime. The inhalation of this solution while spraying may give rise to predominantly interstitial pulmonary lesions which may lead to respiratory insufficiency.
- 41. 7- PORPHYRIA CUTANEA TARDA Vinyl chloride-induced hepatic injury by the inhibition of a number of hepatic enzymes in the porphyrin biosynthesis pathway. Porphyrinuria due to vinyl chloride exposure is rare. Methyl chloride poisoning, Dioxin, HCB, 2,4,5- trichloro-phenoxy acetic acid (2,4,5-T), PCBs & other polyhalogenated aromatic hydrocarbon-induced liver injury. Following exposure to (TCDD), porphyria cutanea tarda seems to be quite a specific disorder, producing increased urinary concentrations of uroporphyrin.
- 42. 8- OTHER LIVER ABNORMALITIES Transient increased values of liver function tests recorded following occupational exposure to methylene chloride. Increased transaminase values with exposure to (DMF) dimethylformamide with microvesicular fat & hepatocellular changes in liver biopsy specimens. Liver biopsy of workers manufacturing pesticide Kepone (chlordecone) showed increased fat, numerous dense bodies & proliferative smooth endoplasmic reticulum, as well as severe neurologic symptoms. Jaundice & mild transient liver necrosis diagnosed in exposed to Chrome during chrome-plating operations.
- 43. Transient liver function abnormalities were also found in association with TCDD exposure. 10% of the Seveso (Italy) population environmentally exposed to TCDD after an industrial explosion had modest elevations of γ-GT. Separately, workers exposed to tetrachlorophenol (TCP) & TCDD had prolonged prothrombin time and elevated plasma lipid & other liver transaminase values. Mild steatosis, periportal fibrosis, activation of Kupffer cells & porphyria cutanea tarda were reported in workers who manufactured TCDD.
- 44. In Japan and Taiwan, more than 2,000 people who ingested cooking rice oil contaminated with PCB and related compounds had abnormal liver function tests, hepatomegaly in severe cases, and electron microscopic alterations in the endoplasmic reticulum and mitochondria in biopsy samples.
- 45. Increased hepatic enzyme values (especially γ-GT & ALT) were seen in human populations who consumed water from a reservoir contaminated with a heavy bloom of the toxic blue-green alga, Microcystis aeruginosa, compared to an adjacent population who drank water from other sources. Toxic hepatitis outbreak occurred in India in 1974 and Kenya in 2004 with a high mortality. These incidents were associated with food contamination with aflatoxin & other mycotoxins.
- 46. LIVER DISORDERS INDUCED BY PHYSICAL AGENTS
- 47. Environmentally induced hyperthermia (heat stroke) can cause acute hepatic injury characterized by Centrilobular necrosis & Cholestasis.
- 48. Exposure to a cumulative dose of Ionizing Radiation in excess of 3,000 to 6,000 rad gives rise to radiation- induced hepatitis 2 to 6 weeks later. Those who survived often subsequently develop cirrhosis with progressive fibrosis & obliteration of the central veins with centrilobular congestion. Radiation-induced hepatitis has been reported after intense accidental exposure.
- 50. There are two types of human malignant liver disorders associated with occupational & environmental hepatotoxicants, 1. Hepatocellular carcinoma (HCC). 2. Hepatic angiosarcoma (HAS) (Endothelial cell sarcoma).
- 51. Codon 249 p53 mutations
- 52. HEPATIC ANGIOSARCOMA (HAS) A rare malignant tumor. Associated with chronic exposure to VCM, Arsenic, Anabolic Steroids, & Thorotrast (an obsolete scintigraphy contrast agent that contained colloidal thorium dioxide, an emitter of α-particle ionizing radiation). Vineyard workers & others who used arsenicals, including Fowler's solution (1% potassium arsenite), or copper as a pesticide. Long-term ingestion of Arsenic-contaminated well water.
- 53. HEPATOCELLULAR CARCINOMA (HCC) One of the most common cancers worldwide, with a striking geographic variation in incidence. In China, accounts for over 300,000 deaths annually & this is the 3rd leading cause of cancer mortality.
- 56. The two major HCC risk factors, HBV & aflatoxin B1 (AFB1) exposure. Presence of aflatoxin-nucleic acid adduct (AFB-N7-gua) in urine always resulted in 2-3 fold increase in HCC risk. A dose-response relationship between urinary aflatoxin M1 (AFM1) levels & HCC in chronic HBV carriers. Mutations in the p53 tumor suppressor gene
- 57. The p53 gene is found mutated in a majority of human cancers, and there is a large variation in number and type of mutations between cancers of different tissues. "molecular fingerprint" in the p53 gene is a characteristic G→T transversion at the 3rd base of codon 249 observed in liver cancer patients from regions of high aflatoxin exposure (50% of HCCs).
- 60. BIOMARKERS & HBV INFECTION IN LIVER CANCER A double mutation in the HBV genome, an adenine to thymine transversion at nucleotide 1762 and a guanine to adenine transition at nucleotide 1764 (1762T/1764A), has been found in HCCs