Pharmaceutical Quality Assurance in the 21st Century, Sharper Focus Needed on Education, Training & Experience 13 June 2016
•
5 gefällt mir•697 views

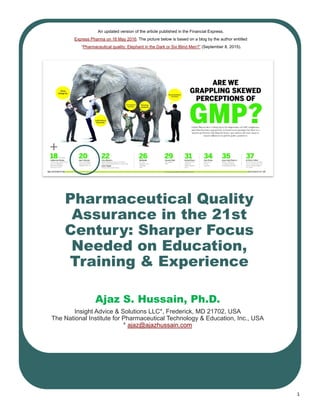
An updated version of the article published in the Financial Express, Express Pharma on 16 May 2016. The picture below is based on a LinkedIn blog by the author entitled “Pharmaceutical quality: Elephant in the Dark or Six Blind Men?” (September 8, 2015).

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (17)
Ähnlich wie Pharmaceutical Quality Assurance in the 21st Century, Sharper Focus Needed on Education, Training & Experience 13 June 2016
Ähnlich wie Pharmaceutical Quality Assurance in the 21st Century, Sharper Focus Needed on Education, Training & Experience 13 June 2016 (20)
Mehr von Ajaz Hussain
Mehr von Ajaz Hussain (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Pharmaceutical Quality Assurance in the 21st Century, Sharper Focus Needed on Education, Training & Experience 13 June 2016
- 1. 1 Pharmaceutical Quality Assurance in the 21st Century: Sharper Focus Needed on Education, Training & Experience Ajaz S. Hussain, Ph.D. Insight Advice & Solutions LLC*, Frederick, MD 21702, USA The National Institute for Pharmaceutical Technology & Education, Inc., USA * ajaz@ajazhussain.com An updated version of the article published in the Financial Express, Express Pharma on 16 May 2016. The picture below is based on a blog by the author entitled “Pharmaceutical quality: Elephant in the Dark or Six Blind Men?” (September 8, 2015).
- 2. 2 India’s aspiration to be ‘Pharmacy of the World’ is credible, palpable and indispensable. Progress achieved over the past several dec- ades is remarkable. A key determinant of this success is the talent pool in India; which is relatively young and getting younger. The quality of their education, training and experience (maturity) is an im- portant determinant of the level of assurance in pharmaceutical quality they can deliver. In the current state, inspectional observations, particularly by several international regulatory authorities, have given a reason for a “pause” - to reflect on how global regulatory expecta- tions for assurance of pharmaceutical quality should be met. Although this challenge is not unique to India; it points to certain “blind- spots” in the current system. Attention to these gaps is in need of urgent attention. Many products we develop and manufacture today are complex, and this complexity is on a rapid rise. This additional complexity places a higher demand on scientific evidence neces- sary to assure quality, safety and efficacy (and equivalence) over the life-cycle of these prod- ucts. Assurance of data integrity is the critical basis for assuring pharmaceutical quality. There is a need to bring more attention to the integrity of evidence. Noted CGMP deviations are, perhaps, a “blessing in disguise”. Learning from these the India’s pharma sector can and should accel- erate its progress towards achieving its goals with a better accounting of complexity and un- certainty in their systems. Unless proactive steps are taken, “blind- spots” can emerge in any rapidly growing business. Examples of such “blind-spots” can include: (a) human tendency for optimistic business forecasts and expectations (e.g., rate of ‘right first time’), (b) under-appreciating intrinsic error rates in a system, and (c) not recognizing the increasing complexity in phar- maceutical quality assurance. Such cognitive biases can put a high burden on achieving ra- tional assurance of quality; especially when results, and the not the process for getting to the result, is often the primary incentive. In such situations staff and managers—and all of us - can be in over our heads (1) and be vul- nerable to irrational decision making (2). Other cognitive biases or blind-spots such “it is US FDA approved”, and “process is validat- ed” can sometimes provide reasons for ration- alizing deviations from established and com- mitted (to regulatory authorities) procedures. Gaps that may have existed in an “FDA Ap- proved” submission (due to an attitude such as “file first and figure it out later” (3)) can re- sult in the development of a commercial man- ufacturing process that is not sufficiently sta- ble and in control. After FDA approval, such gaps are not easy to remember (4-7). Again, this scenario can manifest anywhere in the world. Response to the “pause” induced by the nu- merous warning letters and import alerts, has varied. Some have questioned the validity of this pause. While others have focused on un- derstanding what needs to be understood more clearly and more consistently. This pa- per seeks to support the latter view-point by sharing insights gained by the author on how to strengthen the ‘culture of pharmaceutical quality’ (4-7). This paper recapitulates, sum- marize and consolidate these insights in the current context: Recapitulating insights shared previously, in the year 2013 - “Strategies for making high pharma quality affordable” (8); Summarize new insights gathered while conducting a training program entitled “Culture of Pharmaceutical Quality” at many companies located in diverse geog- raphies of India (5-7); and, Consolidate these in a global context utiliz- ing experience gained as a teacher, a reg- ulator (at US FDA) (4), and as a corporate executive.
- 3. 3 Recapitulating insights shared previously Table 1 (see below) lists insights shared in 2013. It also provides an update - where are we in 2016. The growing evidence supporting the significance of perception factors and pla- cebo/nocebo effects in quality assurance, par- ticularly in the US, is remarkable. It makes the case stronger on the importance of corporate- name recognition, even for companies making generic products. In the US, the year 2015 marks a ‘tipping point’ for adoption of continuous manufactur- ing technologies (12). As discussed in 2013, this potentially sets up different strategies and path to the coveted title of ‘Pharmacy of the World’ (8). To compete, India’s pharma will need to factor these technological develop- ments into their strategies. Companies with a high interest in serving markets in the US will also need to consider changes outlined in the FDA’s review and inspections approaches; particularly on FDA’s sharper focus on ‘One Quality Voice’ (14). The efforts proposed by leaders of India’s pharma sector to collaborate, to engage with global regulators, and to commit to “Quality Excellence” (11) are commendable. Some of the insights shared here are intended to en- courage and contribute to such efforts. New insights gathered since 2013 Efforts expended to develop and conduct a training program on ‘Culture of Pharmaceutical Quality’, for several companies with facilities distributed across India (see 5-7), provided valuable insights. The key take-away from this effort is that “confidence (of/in people, in process/system/results, and in the assurance of product quality) is a critical quality attribute”. Understanding the Why, What, and How of this critical quality attribute is highly variable, and this variability needs to be reduced, signifi- cantly. Insight 2013 (8) Where are we in 2016? Perceptions about quality can change effica- cy and safety of a drug product via placebo and nocebo effects. Evidence on the significance of perception factors, and placebo/nocebo effects emerged very prominently, particularly in the US (9). The US FDA had to issue a final guidance highlighting the importance of color and shape of tablets have on adherence rates (10). Remediation of cGMP issues are often diffi- cult and expensive. CGMP remediation, particularly as it relates to US FDA Warning Letter and Import Alerts, are on-going with very few exceptions and other companies have been added to this list. Leaders should consider working together in pre-competitive space to strengthen training and education, and, for creating venues for dialog with regulators to improve understand- ing and to seek out solutions to common challenges. Leaders of India’s pharma sector have taken significant steps to collaborate and to engage with global regulators and have outlined a plan for “Quality Excellence” (11). With the active encouragement of the US FDA, there is visible progress in the area of continuous monitoring – a potential shift in paradigm in the making. Automated continuous manufacturing is now rapidly becoming a reality in the US and Europe; the tipping point was reached in 2015. Significant collabora- tions have been announced among major companies (12). Increasingly patients across the globe will ask the question “who makes the drug I take”; and trust and credibility will be criti- cal. Media coverage of FDA Warning Letters and Import Alerts have continued to be a source of concern (13).
- 4. 4 Education, Training, and Experience in the 21st Century Pharmaceutical quality assurance in the 21st century necessitates development of curricula and training approaches to facilitate acquisi- tion of new technical know-how alongside communication skills and the maturity to adapt with confidence to environments where com- plexity and uncertainty are high and increas- ing. As noted in 2005, in the US context (4), industrial pharmacy education was and contin- ues to be in need, for a transformation. For example, material science, process design, and control, more rigorous mathematical and statistical skill sets, and systems engineering are some of the areas that are in need for ad- ditional emphasis. More importantly, attention to developing adaptive-learning skills – to in- crease orders of consciousness (1), design/ system thinking, and leadership development must be key areas of focus (7). As leaders of India’s pharma sector progress their efforts on “Quality Excellence” (11), it would be useful to consider establishing world class “Global Institutes of Pharmaceutical Quality” (GIPQ). Given the aspirations of this sector – it is important to take a global per- spective with short-, mid-, and long-term goals. In the short-term the focus should be on de- veloping adaptive-learning skills, design/ system thinking, improving investigations, rig- orous risk assessment, and the know-how to seamlessly implement continued process veri- fication and other topics relevant to proactive compliance with cGMP. In the mid-term focus could be on improving (e.g., standardization and reducing variability in) the broader educa- tional system and providing more opportuni- ties for effective training and experience in quality by design, process analytical technolo- gy, and control strategies. In the long-term, to be a global leader, the focus should be on de- veloping institutions that are recognized as important contributors of knowledge and ex- pertise needed to improve regulatory science and policy across the globe. Increasing complexity and uncertainty place a high demand on knowledge management and on the correct analysis of prior knowledge. There are significant gaps (e.g., objective quality risk assessment, establishing the clini- cal relevance of quality specifications and in the science of pharmaceutical materials as it pertains to functionality and process-ability). The next decade places a high demand for improving pharmaceutical ontology and epis- temology such that the benefits of quality by design methodology, which is now an im- portant foundation of the global regulatory system, are fully realized (15). The pharma- ceutical science and technology, as a disci- pline, has much work to do to fill these gaps. Patients and their care givers need to have trust in our systems. India’s pharma is already a major global play- er. It can and must nurture institutions such as the proposed GIPQ to develop knowledge and expertise needed to support the sector and to also inform on ways to improve domes- tic and global regulatory policies to meet the needs of patients in India and across the globe. The pharmaceutical sector is a major part of India’s economy. India already is and will con- tinue to progress as one of the major econo- mies of the world. Let this journey accelerate (16). References: 1. Kegan, R. In over our heads: The metal demands of modern life.” Harvard Universi- ty Press, 1995. 2. Kahneman D. Thinking, fast and slow. Macmillan; 2011. 3. Ted Fuhr and Katy George (McKinsey & Co). Moving Beyond the Business Case for QbD. 13 March 2011. http://www.pharmaqbd.com/ mckinsey_beyond_business_case_qbd/ (accessed 28 March 2016) 4. Ajaz S. Hussain. The Nation Needs a Comprehensive Pharmaceutical Engineer- ing Education and Research System. Phar- maceutical Technology. September 2005.
- 5. 5 5. Ajaz S. Hussain. Culture of Pharmaceutical Quality: Connecting the Dots. Biopharma Asia, September/October 2015. 6. Ajaz S. Hussain. Culture of Pharmaceutical Quality: Quality Management System. Biophar- ma Asia, November/December 2015. 7. Ajaz S. Hussain. Culture of Pharmaceutical Quality: Personnel Development. Biopharma Asia, March/April 2016. 8. Ajaz S. Hussain. Strategies for making high pharma quality affordable. Express Pharma. 2 November 2013. http://archivepharma.financialexpress.com/ sections/management/2907-strategies-for-making-high-pharma-quality- affordable (accessed 28 March 2016). 9. Peter A. LeWitt, P A., and Kim, S. The pharma- codynamics of placebo: Expectation effects of price as a proxy for efficacy Neurology,84:766– 767 (2015) 10. US FDA Guidance for Industry: Size, Shape, and Other Physical Attributes of Generic Tablets and Capsules. June 2015. 11. Indian Pharmaceutical Alliance. Quality Excel- lence: The next frontier for the Indian pharma- ceutical industry (2016) http://ipa-india.org/pdf/ipa-report- quality-excellence-2016.pdf (Accessed 28 March 2016). 12. Eric Palmer. Vertex, J&J, GSK, Novartis all working on continuous manufacturing facilities. FDA supports the move as a way to improve quality in manufacturing. Fierce Pharma Manu- facturing. February 2015. http:// www.fiercepharmamanufacturing.com/story/vertex-jj-gsk-novartis-all- working-continuous-manufacturing-facilities/2015-02-09 . (accessed 28 March 2016). 13. Caroline Chen and Anna Edney. Generic Drugs: As Imports Rise, Regulators Struggle. Bloom- berg, Mar 18, 2016. http://www.bloombergview.com/quicktake/ generic-drugs . (accessed 28 March 2016). 14. FDA Pharmaceutical Quality Oversight: One Quality Voice. http://www.fda.gov/downloads/AboutFDA CentersOf- fices/OfficeofMedicalProductsandTobacco/CDER/UCM442666.pdf (accessed 28 March 2016). 15. Visioning the Next Decade: NIPTE-FDA Collab- oration. NIPTE Seminar at US FDA, 16 March 2016. http://www.slideshare.net/a2zpharmsci/visioning-the-next-decade- niptefda-collaboration (accessed 28 March 2016). 16. Ajaz S. Hussain. A 21st Century Fable about Pharmaceutical Quality and Preventing a Clash of Cultures. LinkedIn Post. Sep 13, 2015. https:// www.linkedin.com/pulse/21st-century-fable-pharmaceutical-quality- preventing-hussain-ph-d- (accessed 28 March 2016). About the Author: Ajaz is a globally recognized leader in pharmaceutical quality and is one of the most influential ‘Medicine Maker’ (named in the 100 Power list by the UK’s Medicine Maker magazine in 2015). He trained at the Bom- bay College of Pharmacy (B. Pharm, 1981) and received an interdisciplinary doctoral degree from University of Cincin- nati (1986). He began his career as Assistant Professor of Pharmacy at the Ohio Northern University and in 1989 he returned to University of Cincinnati as Research Assistant Professor of Pharmaceutics. He was promoted to Associate Professor (1992) and achieved tenure status in 1994. In 1995 he moved to the US FDA CDER as Branch Chief for Biopharmaceutics Research and thereafter was rapidly pro- moted with increasing oversight and policy development responsibilities in the area of product quality (Director Prod- uct Quality Research (DPQR) and then Director Office of Testing and Research). In 2000 he was promoted to the position of Deputy Director Office of Pharmaceutical Sci- ence and served under the Senior Biomedical Research Service (SBRS – a track under the Public Health Service Act). His contributions at FDA range from research on spe- cific topics (such as the Biopharmaceutics Classification System Guidance) to global policy development (such as ICH Q8) in the area of Quality by Design. He launched and led the FDA’s PAT Initiative. He and his teams were recog- nized by two FDA Scientific Achievement Awards. In 2005 he moved to Sandoz (a division of Novartis Corp.) as Vice President and Global Head for Biopharmaceutical Develop- ment and contributed to this organization for achieving the industry leadership position in Biosimilars. He was then recruited by Philip Morris International (PMI) in Switzerland to develop adjacent business opportunities (tobacco plant- based vaccines) and to establish a rigorous scientific basis for tobacco harm reduction. At PMI he was promoted to the position of Chief Scientific Officer. For about a year he served as the Chief Scientific Officer and President Biotech- nology at Wockhardt Ltd. He launched his consulting firm Insight Advice and Solutions LLC in July 2013. In October 2014 he was also appointed as the Executive Director of the National Institute for Pharmaceutical Technology and Education, a collaboration among pharmaceutical science and engineering programs at 15 major universities in the USA. He was elected President of NIPTE in February 2016. Ajaz is a Fellow of the American Association of Phar- maceutical Scientist and of the Swiss Society of Pharma- ceutical Sciences. Email;: Ajaz@ajazhussain.com Phone: +12404577064