Empfohlen

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Colon Cancer PDX Organoids and Cell Lines
Ähnlich wie Colon Cancer PDX Organoids and Cell Lines (20)
Mehr von Sean Maden
Mehr von Sean Maden (6)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Colon Cancer PDX Organoids and Cell Lines
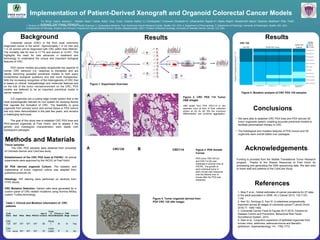
- 1. Background Methods and Materials Acknowledgements Implementation of Patient-Derived Xenograft and Organoid Colorectal Cancer Models Conclusions Results Figure 2. CRC PDX 114 Tumor H&E Images H&E slides from PDX CRC114 in two separate mice at time of final collection shown at (A) 4x (B) 20x the mucinous differentiation and lymphoid aggregation. Tissue samples: The CRC PDX samples were obtained from University of Colorado-Denver and ColoCare study. Establishment of the CRC PDX lines at FHCRC: All animal experiments were approved by the IACUC at Fred Hutch. 3D PDX derived organoid Culture: The isolation and maitainance of tumor organoid culture was adapted from published protocols (4). Histology: H/E staining were performed on sections from FFPE blocks. CRC Mutation Detection: Variant calls were generated for a custom panel of CRC-related mutations using Illumina MiSeq custom TruSeq technology. Figure 5. Mutation analysis of CRC PDX 125 samples. Figure 1. Experiment Overview Figure 4. Tumor organoid derived from PDX CRC 125 (40x image) Figure 3. PDX Growth Curves PDX tumor CRC125 (A) and CRC114 (B) was implanted in several mice at FHCRC. The growth of each individual tumor in each mouse was measured over the lifetime over of mouse after the PDX was implanted. CRC114CRC125 B Code Name Braf KRas NRas PIK3CA Age of Consent Colon or Rectal Primary or Metastatic TNM Stage Chemo? CRC 125 WT WT WT WT 58 Recta l M IV Yes CRC 114 V600E WT WT WT 70 Colon (right) P III No A B • We were able to establish CRC PDX lines and PDX derived 3D tumor organoids system, enabling accurate preclinical models to facilitate personalized therapy in CRC. • The histological and mutation features of PDX tumors and 3D organoids were overall stable over passages. Colorectal cancer (CRC) is the third most commonly diagnosed cancer in the world1 . Approximately 1 in 22 men and 1 in 24 women will be diagnosed with CRC within their lifetime2 . The mortality rate for men is 17.7% and women is 12.4%3 . This highlights the need for new advances in treatment and technology to understand the unique and important biological features of CRC. PDX cancer models accurately recapitulate key aspects of human CRC behavior (i.e. response to therapies) and are rapidly becoming accepted preclinical models to both query fundamental biological questions and test novel therapeutics. With the increasing recognition of the heterogeneity of CRC that is based on clinical, histopathologic and molecular features and on the role of the tumor microenvironment on the CRC, PDX models are believed to be an important preclinical model in cancer research. 3-D organoids are a cutting edge model system that is the most physiologically relevant ex vivo system for studying factors that regulate the formation of CRC. The feasibility to grow organoids from primary tumor and normal tissue or PDX tumors has only been demonstrated in the past few years, and remains a challenging technique. The goal of this study was to establish CRC PDX lines and PDX-derived organoids at Fred Hutch, and to assess if the genetic and histological characteristics were stable over subsequent passages. Table 1. Clinical and Mutation information of CRC patients Results Funding is provided from the Seattle Translational Tumor Research program. Thanks to the Shared Resources at Fred Hutch for processing and generating the DNA sequencing data. We also wish to thank staff and patients of the ColoCare Study. A B A B References 1. Bray F et al., Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int J Cancer 2013; 132:1133– 1145. 2. Kerr DJ, Domingo E, Kerr R. Is sidedness prognostically important across all stages of colorectal cancer? Lancet Oncol. 2016;17: 1480-1482 3. Colorectal Cancer Facts & Figures 2017-2019. Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System, 2014. 4. Sato et al., Long-term expansion of epithelial organoids from human colon, adenoma, adenocarcinoma and Barrett’s epithelium. Gastroenterology 141, 1762-1772. Yu, Ming1 ; Ayers, Jessica L.1 ; Maden, Sean1 ; Carter, Kelly1 ; Guo, Yuna1 ; Vickers, Kathy2 ; Li, Christopher2 ; Cromwell, Elizabeth A3 ; Uthamanthil, Rajesh K3 ; Stella, Nephi4 ; Westerhoff, Maria5 ; Stachler, Matthew6 ; Pitts, Todd7 ; Eckhardt, Gail7 ;Grady, William M.1 1. Division of Clinical Research; 2. Division of Public Health Sciences; 3. Comparative Medicine, Fred Hutchinson Cancer Research Center, Seattle, WA. USA; 4. Department of Pharmacology, 5. Department of Pathology, University of Washington, Seattle, WA. USA; 6.Department of Pathology, Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts, USA; 7.Division of Medical Oncology, University of Colorado Denver, Denver, CO, USA.