Empfohlen

Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie Poster Assignment ABC vs FES-I
Ähnlich wie Poster Assignment ABC vs FES-I (20)
Poster Assignment ABC vs FES-I
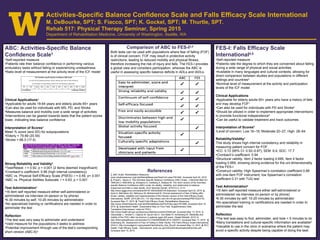
- 1. ABC: Activities-Specific Balance Confidence Scale1 •Self-reported measure •Patients rate their balance confidence in performing various ambulatory tasks without falling or experiencing unsteadiness •Ratio level of measurement at the activity level of the ICF model Clinical Applications1 •Applicable for adults 18-64 years and elderly adults 65+ years •Can also be used for individuals with MS, PD, and Stroke •Measures balance and mobility over a wide range of activities •Interventions can be geared towards tasks that the patient scores lower, indicating less balance confidence Interpretation of Scores1 Mean % score (and SD) for subpopulations: •Elderly = 79.89 (20.59) •Stroke = 68.3 (17.5) Strong Reliability and Validity2 •Test/Retest: r = 0.92, p < 0.001 (2 items deemed insignificant) •Cronbach’s coefficient: 0.96 (high internal consistency) •ABC vs. Physical Self-Efficacy Scale (PSES): r = 0.49, p< 0.001 •ABC vs. Physical Abilities Subscale: r = 0.63, p < 0.001 Test Administration1 •16 item self reported measure either self-administered or administered via interview (in-person or by phone) •6-30 minutes by self; 10-20 minutes by administrator •No specialized training or certifications are needed in order to administer the test Reflection •The test was very easy to administer and understand •Valid measure for the populations it seeks to address •Potential improvement through use of the test’s corresponding short version (ABC-6)3 Activities-Specific Balance Confidence Scale and Falls Efficacy Scale International M. DeBourke, SPT; S. Fiacco, SPT; K. Gockel, SPT; M. Thurtle, SPT. Rehab 517: Physical Therapy Seminar, Spring 2015 Department of Rehabilitation Medicine, University of Washington, Seattle, WA Comparison of ABC to FES-I2,4 Both tests can be used with populations where fear of falling (FOF) is of clinical concern. FOF may result in protective activity restrictions, leading to reduced mobility and physical fitness, therefore increasing the risk of injury and falls. The FES-I provides a global view and considers participation, whereas the ABC is useful in assessing specific balance deficits in ADLs and IADLs. FES-I: Falls Efficacy Scale International4,5 •Self-reported measure •Patients rate the degree to which they are concerned about falling during a wide range of physical and social activities •Available in many languages and cultural contexts, allowing for direct comparison between studies and populations in different settings and countries6 •Nominal level of measurement at the activity and participation levels of the ICF model Clinical Applications •Applicable for elderly adults 65+ years who have a history of falls and may develop FOF7 •Can also be used for individuals with PD and Stroke4 •Should be utilized in order to implement appropriate interventions to promote functional independence8 •Can be useful to validate treatment and track outcomes Interpretation of Scores9 •Level of concern: Low 16–19; Moderate 20–27; High: 28–64 Reliability/Validity7 This study shows high internal consistency and reliability in measuring patient concern for FOF. •ICC: 0.72 (95% CI: 0.52–0.87); SEM: 6.4; SDC: 17.7 •Cronbach’s coefficient: 0.94 •Structural validity: Item 2 factor loading 0.695, Item 4 factor loading 0.669, showing strong evidence for the uni-dimensionality of the FES-I •Construct validity: High Spearman’s correlation coefficient 0.68 with one-item FOF instrument; low Spearman’s correlation coefficient 0.31 with TUG test Test Administration5 •16 item self reported measure either self-administered or administered via interview (in-person or by phone) •6-30 minutes by self; 10-20 minutes by administrator •No specialized training or certifications are needed in order to administer the test Reflection •The test was easy to find, administer, and took < 5 minutes to do •Many translations and cultural-specific information are available6 •Valuable to use in the clinic in scenarios where the patient may avoid a specific activity despite being capable of doing the task References 1. ABC Scale. Rehabilitation Measures. www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=949. Accessed April 24, 2015. 2. Powell L, Myers A. The Activities-Specific Balance Confidence (ABC) Scale. J Gerontol Med Sci. 1995;50(1): M28-M34. 3. Schepens S, Goldberg A, Wallace M. The short version of the Activities- specific Balance Confidence (ABC) scale: Its validity, reliability, and relationship to balance impairment and falls in older adults. Arch Gerontol Geriatr. 2010;51(1): 9-12. http://www.aggjournal.com/article/S0167-4943(09)00145-9/abstract. Accessed April 24, 2015. 4. Azad A, Mehraban AH, Mehrpour M, Mohammadi B. Clinical assessment of fear of falling after stroke: validity, reliability and responsiveness of the Persian version of the Falls Efficacy Scale- International. MJIRI. 2014;28(131): 1-8. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4322319/. Accessed May 17, 2015. 5. Tinetti Falls Efficacy Scale. Rehabilitation Measures. http://www.rehabmeasures.org/Lists/RehabMeasures/PrintView.aspx?ID=899. Accessed April 15, 2015. 6. Queensland Health. Queensland Stay on Your Feet. Supplementary Data Translators’/Interviewers’ notes for FES-I. http://www.health.qld.gov.au/stayonyourfeet/documents/33346.pdf. Accessed May 13, 2015. 7. Visschedijk J, Terwee C, Caljouw M, Spruit-Van E, Van Balen R, Achterberg W. Reliability and validity of the FES-I after hip fracture in patients aged ≥65 years. Disabil Rehabil. 2015;14. http://informahealthcare.com/doi/abs/10.3109/09638288.2014.1002573. Accessed May 17, 2015. 8. Greenberg SA. Assessment of Fear of Falling in Older Adults: The Falls Efficacy Scale-International (FES-I). http://consultgerirn.org/uploads/File/trythis/try_this_29.pdf. Accessed May 13, 2015. 9. NYC Health. Falls Efficacy Scale - International. www.nyc.gov/html/doh/downloads/pdf/win/fes.pdf. Accessed April 15, 2015.