Maternal anatomy shi
•Als PPTX, PDF herunterladen•
18 gefällt mir•5,137 views

source: williams obstetrics

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Maternal anatomy shi
Ähnlich wie Maternal anatomy shi (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Maternal anatomy shi
- 1. MATERNAL ANATOMY MA. SHIRIL J. ARMERO, M.D.
- 2. Maternal anatomy • Anterior abdominal wall • External Generative Organs – Vulva – Vagina, Hymen – Perineum • Internal Generative Organs – Uterus – Ligaments – Ovaries – Fallopian Tubes • Pelvic Anatomy
- 3. LAYERS OF THE ANTERIOR ABDOMINAL WALL • Skin – Langer lines • Subcutaneous Layer – Camper’s fascia – Scarpa’s fascia • Primary fascia (aponeurosis) • Abdominal wall muscles – Rectus abdominis – Pyramidalis – Obliques (Ext. & Int.) – Tranversus abdominis
- 4. LAYERS OF THE ANTERIOR ABDOMINAL WALL • Skin – Langer lines • Subcutaneous Layer – Camper’s fascia – Scarpa’s fascia • Primary fascia (aponeurosis) • Abdominal wall muscles • Peritoneum – +/- Transversalis fascia
- 5. LAYERS OF THE ANTERIOR ABDOMINAL WALL • Skin – Langer lines • Dermal fibers within the skin • Arranged transversely
- 6. LAYERS OF THE ANTERIOR ABDOMINAL WALL • Skin – Langer lines • Subcutaneous Layer – Camper’s fascia – Scarpa’s fascia
- 7. LAYERS OF THE ANTERIOR ABDOMINAL WALL • Skin – Langer lines • Subcutaneous Layer – Camper’s fascia (fatty) – Scarpa’s fascia (membranous)
- 8. LAYERS OF THE ANTERIOR ABDOMINAL WALL • Primary fascia (aponeurosis), Rectus sheath
- 9. LAYERS OF THE ANTERIOR ABDOMINAL WALL • Abdominal wall muscles – Rectus abdominis – Pyramidalis – External Oblique – Internal Oblique – Tranversus abdominis
- 10. Blood Supply of the ANTERIOR ABDOMINAL WALL Anterior abdominal wall
- 11. Blood Supply of the ANTERIOR ABDOMINAL WALL Anterior abdominal wall
- 12. Nerve Supply of the ANTERIOR ABDOMINAL WALL Anterior abdominal wall
- 14. Nerve Supply of the ANTERIOR ABDOMINAL WALL Anterior abdominal wall
- 16. EXTERNAL GENERATIVE ORGANS Vulva (Pudenda) Structures visible externally from SP to the perineal body Includes: mons pubis labia majora labia minora Hymen Vestibule Urethral opening greater vestibular gland minor vestibular glands Clitoris paraurethral glands
- 17. EXTERNAL GENERATIVE ORGANS Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 18. EXTERNAL GENERATIVE ORGANS • Vulva (pudenda): includes all structures visible externally from the symphysis pubis to the perineal body. Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 19. EXTERNAL GENERATIVE ORGANS CLITORIS • Principal female erogenous organ • Parts: – Glans – richly innervated – Corpus – (2) crura • Blood supply: – Branches of the internal pudendal artery
- 20. EXTERNAL GENERATIVE ORGANS VESTIBULE • Boundaries – P: fourchette – A: clitoral frenulum anteriorly – L: Hart line laterally – M: external surface of hymen medially • fossa navicularis – posterior portion of the vestibule between the fourchette and the vaginal opening nulliparas
- 21. VESTIBULE • perforated by 6 openings – Urethra – Vagina – Bartholin gland ducts – Skene glands EXTERNAL GENERATIVE ORGANS
- 22. VESTIBULE • Bartholin glands – Greater vestibular glands – Bartholin cyst (obstructed) – Bartholin abscess (if infected) • Paraurethral glands • Skene glands – largest • Inflammation, duct obstruction urethral diverticulum formation
- 23. HYMEN
- 24. VAGINA
- 25. VAGINA anterior wall: 6 to 8 cm posterior vaginal wall: 7 to 10 cm Lining: NKSS
- 26. VAGINA anterior wall: 6 to 8 cm posterior vaginal wall: 7 to 10 cm Lining: NKSS There are no vaginal glands. Blood supply: cervical branch of the uterine artery and by the vaginal artery
- 27. VAGINA anterior wall: 6 to 8 cm posterior vaginal wall: 7 to 10 cm Lining: NKSS There are no vaginal glands. Blood supply: Middle rectal artery Internal pudedal artery
- 28. VAGINA Lymphatics: inguinal lymph nodes lower third, along with those of the vulva internal iliac nodes middle third external, internal, and common iliac nodes upper third
- 29. ANATOMY OF THE PERINEUM Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 30. ANATOMY OF THE ANTERIOR TRIANGLE
- 31. ANATOMY OF THE ANTERIOR TRIANGLE • Urethra – Measures 3-4cm – Lining: transitional to NKSS epithelium – Blood supply: • Inferior vessical • Vaginal • Internal pudendal – Smooth muscle: ILOC – Striated urogenital sphincter (Skeletal muscle) • Sphincter urethrae • Urethrovaginal sphincter • Compressor urethrae Innervated by pudendal nerve
- 32. PELVIC DIAPHRAGM • broad muscular sling that provides substantial support to the pelvic viscera • composed of: – Levator Ani* Pubococcygeus puborectalis iliococcygeus – Coccygeus Muscle
- 33. ANATOMY OF THE POSTERIOR TRIANGLE ISCHIOANAL FOSSAE • two fat-filled wedge-shaped spaces found on either side of the anal canal (comprise the bulk of the posterior triangle) ANAL CANAL distal continuation of the rectum: begins at the level of levator ani attachment to the rectum and ends at the anal skin (4 to 5-cm long) • Anal cushion – aids in the complete closure of canal and fecal continence when apposed • Lining (mucosa): – columnar epithelium (upper) – stratified squamous epithelium (dentate line) Hemorrhoids • External CC: pain (inferior rectal nerve) • Internal CC: bleeding
- 34. The ANAL SPHINCTER Complex Description Function Symptoms EAS Striated muscle attaching to PB anteriorly Provides squeeze pressure responsible or maintaining fecal continence when continence is threatened 25% resting pressure Provides emergency control for liquid stool and flatus Fecal urgency Urge incontinence: liquid & flatus IAS Continuation of the rectal circular smooth muscle. (70-85% resting pressure) maintenance of fecal continence at rest Receives parasympathetic nerve fibers Keeps anal canal closed at rest, continence of liquid stool & flatus Fecal soiling Incontinence of liquid stool and flatus
- 36. PUDENDAL NERVE • Anterior rami of S2-4 • Lies within the Alcock canal • 3 terminal branches: – Dorsal nerve of the clitoris – Perineal nerve • Posterior labial branches • Muscular branches – Inferior rectal
- 38. INTERNAL GENERATIVE ORGANS • Cervix • Uterus • Ovaries • Fallopian tubes • Ligaments • Blood supply • Lymphatics • innervation
- 39. Cervix • Small opening (nulli) • Slit-like (parous) • Ectocervix: NKSS epithelium • Endocervix: Simple Columnar ep. • SCJ is the mc site of malignant transformation • Eversion – during pregnancy • Composition: collagen, elastin, proteoglycans, very little SM • Chadwick sign – bluish discoloration due to increased vascularity. • Goodell sign – softening due to cervical edema • Hegar sign – isthmic softening
- 40. Uterus nulligravid multiparous Weight 60kg Weighs more Length 6-8cm 9-10cm Fundus and cervix Equal in length Cervix is only a third of entire length
- 41. ANTERIOR POSTERIOR LATERAL ANTERIOR POSTERIOR LATERAL ANTERIOR POSTERIOR LATERAL FALLOPIAN TUBE FALLOPIAN TUBE ROUND LIGAMENT ROUND LIGAMENT OVARIAN LIGAMENT OVARIAN LIGAMENT FALLOPIAN TUBE
- 42. Where does the ROUND ligament terminate? LABIA MAJORA
- 43. Where ARTERY courses through the ROUND ligament? SAMPSON artery
- 44. Ligaments Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 45. • The broad ligaments • two winglike structures that extend from the lateral uterine margins to the pelvic sidewalls. • Peritoneum that folds over the fallopian tube mesosalpinx, round ligament is the mesoteres • ovarian ligament is the mesovarium. Ligaments
- 46. Ligaments Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 47. Ligaments • CARDINAL LIGAMENT – Transverse Cervical Ligament – Mackenrodt ligament • anchors medially to the uterus and upper vagina. • Parametrium is the connective tissues adjacent and lateral to the uterus within the broad ligament. • Paracervical tissues are those adjacent to the cervix • Paracolpium is that tissue lateral to the vaginal walls.
- 50. Moore, K. et. al. Moore Clinically Oriented Anatomy. 7th Edition. Lippincott Williams & Wilkins, 2014.
- 51. Venous drainage • the right ovarian vein empties into the vena cava • left ovarian vein empties into the left renal vein
- 52. Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 53. Lymphatics • Cervix: internal iliac nodes • Uterine corpus: internal iliac nodes, paraaortic lymph nodes
- 54. Fallopian Tubes (Oviducts) • 8–14 cm from the uterine cornua Moore, K. et. al. Moore Clinically Oriented Anatomy. 7th Edition. Lippincott Williams & Wilkins, 2014.
- 55. Fallopian Tubes (Oviducts) • Mesosalpinx • Myosalpinx • Endosalpinx Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 56. Ovaries • Rests at the ovarian fossa of Waldeyer. • Sympathetic nerves: ovarian plexus (originates in the renal plexus) • Parasympathetic input: vagus nerve
- 57. Ovaries • Sympathetic nerves: ovarian plexus (originates in the renal plexus) • Parasympathetic input: vagus nerve • Sensory afferents follow the ovarian artery and enter at T10 spinal cord level.
- 58. Fallopian Tubes (Oviducts) • 8–14 cm from the uterine cornua Moore, K. et. al. Moore Clinically Oriented Anatomy. 7th Edition. Lippincott Williams & Wilkins, 2014.
- 59. What internal generative organ is unchanged during pregnancy? • Cervix • Uterus • Fallopian Tubes • Ovaries
- 60. What internal generative organ is unchanged during pregnancy? • Cervix • Uterus • Fallopian Tubes Ovaries
- 61. Derivatives of Embryonic genital Structures Structure Female Male homologue Undifferentiated Gonad Ovary Testis Mullerian Duct FT Appendix of testesUterus Cervix Urogenital sinus Vagina Prostatic utricle Hymen Seminal colliculus Phallus Clitoris Penis Labioscrotal swelling Labia majora Scrotum Urogenital Folds Labia minora Ventral part penis
- 62. FEMALE REPRODUCTIVE TRACT Lining Epithelium Vulva Vagina Cervix Uterus FT Ovary Stratified squamous keratinizing Stratified squamous non- keratinizing Ectocervix: stratified squamous non-keratinizing Endocervix: simple columnar mucin-producing Simple columnar Simple columnar ciliated cuboidal Transformation zone: squamo-columnar junction
- 63. PELVIC BONES Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 64. PELVIC BONES
- 65. Pelvic Joints • Anteriorly: the symphysis pubis • Posteriorly: the sacroiliac joints limited degree of mobility during pregnancy: upward gliding of the sacroiliac joint (dorsal lithotomy) increase the diameter of the outlet by 1.5–2.0 cm
- 66. Planes and Diameters of the Pelvis 1. The plane of the pelvic inlet—the superior strait 2. The plane of the pelvic outlet—the inferior strait 3. The plane of the midpelvis—the least pelvic dimensions 4. The plane of greatest pelvic dimension—of no obstetrical signifcance
- 67. Pelvimetry Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
- 68. Pelvic Inlet • True conjugate • Obstetric conjugate – 10cm or more – Shotest distance between the sacral promontory and SP – Cannot directly measured • Diagonal conjugate – Can be assessed clinically – DC – 1.5 or 2cm = OC
- 69. Pelvimetry Midpelvis • Cannot be directly measured • Contracted if: Ischial spines prominent Sacrum concavity is shallow Sidewalls converge Pelvic Outlet • Diameter between the ischial tuberosities (normal: 8cm) • Measurement can be estimated by putting a closed fist again the perineum between the ischial tuberosities. • Pubic arch (wide)
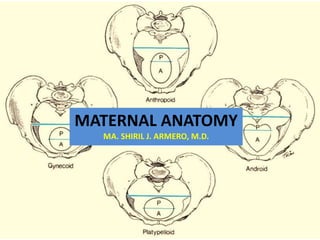
- 70. Pelvic Shapes • Caldwell-Moloy anatomical classifcation of the pelvis: based on shape Cunningham, et. al. Williams Obstetrics, 24th Edition. McGraw-Hill Education, New York, 2014
Hinweis der Redaktion
- vertical skin* incisions sustain greater lateral tension and thus, in general, develop wider scars. In contrast, low transverse incisions, such as the Pfannenstiel, follow Langer lines and lead to superior cosmetic results.
- Camper’s F provided fat substance to the mons, labia while the scarpa’s fascia continue inferiorly to the peineum as COLLE’S FASCIA. As a result, perineal infection or hemorrhage superficial to Colles fascia has the ability to extend upward to involve the superficial layers of the abdominal wall. likewise, seroma may also present as edema on the perineum
- The construction varies above and below the arcuate line. Cephalad to this border, the aponeuroses invest the rectus abdominis bellies on both dorsal and ventral surfaces.* Caudal to this line all aponeuroses lie ventral or superficial to the rectus abdominis muscle, and only the thin transversalis fascia and peritoneum lie beneath the rectus
- The superficial epigastric, superficial circumflex iliac, and superficial external pudendal arteries arise from the femoral artery just below the inguinal ligament within the femoral triangle. SUPPLYING skin and subcutaneous layers and mons. the SUPERFICIAL EPIGASTRIC VESSELS are surgically important to the obstetrician and course diagonally from their origin toward the umbilicus. With a low transverse skin incision, these vessels can usually be identified at a depth halfway between the skin and the anterior rectus sheath. They lie above Scarpa fascia and several centimeters from the midline. Ideally, these vessels are identified and surgically occluded.
- the inferior “deep” epigastric vessels and deep circumflex iliac vessels are branches of the external iliac vessels.They supply the muscles and fascia of the anterior abdominal wall. When a Maylard incision is used for cesarean delivery, the inferior epigastric artery may be lacerated lateral to the rectus belly during muscle transection. These vessels rarely may rupture following abdominal trauma and create a rectus sheath hematoma. Hesselbach triangle is the region bounded laterally by the inferior epigastric vessels, inferiorly by the inguinal ligament, and medially by the lateral border of the rectus muscle: direct inguinal hernias indirect inguinal hernias do so through the deep inguinal ring, which lies lateral to this triangle, and then may exit out the superficial inguinal ring
- IC and SC nerves are anterior rami of the thoracic spinal nerves: run along the lateral and then anterior abdominal wall in the transversus abdominis plane. (between the transversus abdominis and internal oblique muscles) Near the rectus abdominis lateral borders, these nerve branches pierce the posterior sheath, rectus muscle, and then anterior sheath to reach the skin. Thus, these nerve branches may be severed during a Pfannenstiel incision at the point in which the overlying anterior rectus sheath is separated from the rectus muscle.
- The anterior abdominal wall is innervated by intercostal nerves (T7–11) subcostal nerve (T12) iliohypogastric and the ilioinguinal nerves (L1)
- Originate from the anterior ramus of the first lumbar spinal nerve: At a site 2 to 3 cm medial to the anterior superior iliac spine, the nerves then pierce the internal oblique muscle and course superficial to it toward the midline. Iliohypogastric nerve perforates the external oblique aponeurosis near the lateral rectus border to provide sensation to the skin over the suprapubic area. The ilioinguinal nerve in its course medially travels through the inguinal canal and exits through the superficial inguinal ring, which forms by splitting of external abdominal oblique aponeurosis fibers. This nerve supplies the skin of the mons pubis, upper labia majora, and medial upper thigh. The ilioinguinal and iliohypogastric nerves can be severed during a low transverse incision or entrapped during closure, especially if incisions extend beyond the lateral borders of the rectus muscle
- II and IH nerves carry sensory information only, and injury leads to loss of sensation within the areas supplied. Rarely, chronic pain may develop (Whiteside, 2005). The T10 dermatome approximates the level of the umbilicus. Analgesia to this level is suitable for labor and vaginal birth. Regional analgesia for cesarean delivery or for puerperal sterilization ideally extends to T4. Regional analgesia for cesarean delivery or for puerperal sterilization ideally blocks T10 through L1 Levels.
- Mons pubis/mons veneris, is a fat-filled cushion overlying the symphysis pubis. After puberty, it is covered by curly hair that forming the escutcheon, triangular in shape, In men and some hirsute women, the escutcheon is not so well circumscribed and extends to the anterior abdominal wall toward the umbilicus. the labia majora are homologous with the male scrotum. Labia vary depending on the fat they contain. round ligaments terminate at their upper borders. Posteriorly, the labia majora taper and merge into the area overlying the perineal body to form the posterior commissure. Hair covers the labia majora outer surface but is absent on their inner surface. In addition, apocrine, eccrine, and sebaceous glands are abundant. During pregnancy, rich vascular plexus commonly develops varicosities, especially in parous women, from increased venous pressure created by the enlarging uterus. They appear as engorged tortuous veins or as small grapelike clusters, but they are typically asymptomatic.
- labium minus Male homologue: ventral shaft of the penis. The labia minora extend superiorly, where each divides into two lamellae. lower lamellae fuse to form the frenulum the upper merge to form the prepuce. Inferiorly, the labia minora extend to approach the midline to form the fourchette. Epithelia depends on location: Thinly keratinized stratifed squamous epithelium covers the outer surface of each labium. On their inner surface, the lateral portion is covered by this same epithelium up to the Hart line. Medially, squamous epithelium that is nonkeratinized. The labia minora lack hair follicles, eccrine glands, and apocrine glands. However, there are many sebaceous glands. They are supplied with many nerve endings and are extremely sensitive
- erectile homologue of the glans located beneath the prepuce, above the frenulum and urethra, and projects downward and inward rarely exceeds 2 cm in length covered by stratified squamous epithelium richly innervated and extremely sensitive
- derived from the embryonic urogenital membrane almond-shaped area
- Bartholin glands greater vestibular glands measure 0.5 to 1 cm in diameter. The ducts open distal to the hymenal ring: 5 and 7 o’clock on the vestibule Paraurethral glands collective arborization of glands whose multiple small ducts open predominantly along the entire inferior aspect of the urethra two largest are called Skene glands with ductsnear the urethral meatus inflammation and duct obstruction of any of the paraurethral glands leads to urethral diverticulum formation urethral opening or meatus midline of the vestibule 1 to 1.5 cm below the pubic arch
- Hymen a membrane of varying thickness that surrounds the vaginal opening composed mainly of elastic and collagenous connective tissue, covered by nonkeratinized stratified squamous epithelium Imperforate hymen is a rare malformation in which the vaginal orifice is occluded completely, there is failure to canalize In pregnant women -> hymeneal epithelium is thick and rich in glycogen and transforms into myrtiform caruncles
- Vagina a thin-walled, distensible, fibromuscular tube that extends from the vestibule of the vulva to the uterus and is interposed lengthwise between the bladder* and the rectum* Anteriorly separated by the vesicovaginal septum and posteriorly separated by the rectovaginal septum. The upper fourth of the vagina is separated from the rectum by the rectouterine pouch/cul-de-sac or pouch of Douglas
- potential space of the vagina is larger in the middle and upper thirds At the midportion of the vagina, its lateral walls are attached to the pelvis by visceral connective tissue that blend into the investing fascia of the levator ani. Creating a letter H in cross section due to flattened AP diameter upper end of the vaginal vault is subdivided by the cervix anterior fornix posterior fornix two lateral fornices clinically importance since the internal pelvic organs may be palpated of these fornices and posterior fornix provides surgical access to the peritoneal cavity. vaginal lining : nonkeratinized stratified squamous epithelium and underlying lamina propria.
- there are no vaginal glands vagina is lubricated by a transudate originating from the vaginal subepithelial capillary plexus abundant vascular supply: proximal portion is supplied by the cervical branch of the uterine artery and by the vaginal artery (arising from the uterine or inferior vesical or directly from the internal iliac artery)
- there are no vaginal glands vagina is lubricated by a transudate originating from the vaginal subepithelial capillary plexus abundant vascular supply: proximal portion is supplied by the cervical branch of the uterine artery and by the vaginal artery (arising from the uterine or inferior vesical or directly from the internal iliac artery) middle rectal artery contributes supply to the posterior vaginal wall the distal walls receive contributions from the internal pudendal artery
- AP VIEW between the pubic symphysis and coccyx, wc is a diamond shape area consisting of two triangleAn arbitrary line joining the ischial tuberosities divides the perineum into an anterior (urogenital) triangle, and a posterior (anal) triangle. The perineal body (also called the central tendon of the perineum) is a fibromuscular mass found in the midline at the junction between these anterior and posterior triangles. It measures 2 cm tall and wide and 1.5 cm thick. It serves as the junction for several structures and provides significant perineal support. So let’s start with the urogenital triangle.
- The anterior triangle is divided by the perineal membrane into superficial and deep Superficially, we find the 3 muscles: ischiocavernosus muscles help maintain clitoral erection by compressing the crus to obstruct venous drainage bulbocavernosus muscles constrict the vaginal lumen and aid release of secretions from the Bartholin glands. They also may contribute to clitoral erection by compressing the deep dorsal vein of the clitoris. Last, the superficial transverse perineal muscles are narrow strips that attach to the ischial tuberosities laterally and the perineal body medially. They may be attenuated or even absent, but when present, they contribute to the perineal body. Clinical significance: vulvar hematoma located superficially (above PM) will be enclosed in this space
- In contrast to the superficial perineal space, deep space is continuous with pelvic cavity superiorly. The striated urogenital sphincter supplies constant tonus and provide emergency reflex contraction to sustain continence.
- Found deep to the anterior and posterior triangles Vaginal birth conveys significant risk for damage to the levator ani or to its innervation. Of these muscles, the pubovisceral muscle is more commonly damaged. Evidence supports that these injuries may predispose women to greater risk of pelvic organ prolapse or urinary incontinence
- The fat found within each fossa provides support to surrounding organs yet allows rectal distention during defecation and vaginal stretching during delivery. Clinically, injury to vessels in the posterior triangle can lead to hematoma formation in the ischioanal fossa, and possible large accumulation in these easily distensible spaces. These two fossae communicate dorsally, thus an episiotomy infection or hematoma may extend from one fossa into the other. Within the anal canal, three highly vascularized submucosal arteriovenous plexuses termed anal cushions aid complete closure of the canal and fecal continence when apposed. Increasing uterine size, excessive straining, and hard stool create increased pressure that ultimately leads to degeneration and subsequent laxity of the cushion’s supportive connective tissue base. These cushions then protrude into and downward through the anal canal. This leads to venous engorgement within the cushions— now termed hemorrhoids
- Layers of the anal canal: Anal mucosa, IAS, longitudinal smooth muscle, EAS, puborectalis The distal site where IAS ans EAS overlap is called the intersphincteric groove which is palpable on DRE Blood supply: inferior rectal artery of internal pudendal Innervation: inferior rectal br of the pudendal nerve
- Clinically, we apply the sphincter complex knowledge in vaginal delivery. So, What degree of laceration?
- Due to its location, when doing pudendal block, locate the ischial spines. It may be at risk for stretch injury during downward displacment of the pelvic floor during childbirth.
- Major blood supply of the perineum is via the internal pudendal A and branches mirrior the pudendal nerve
- Eversion – the endocervical epithelium moves out and onto the ectocervix
- Anterior: bladder Posterior: rectum Entire posterior portion is covered by the serosa/ visceral peritoneum while only the upper portion of the anterior wall is covered, creating a vesicouterine pouch. Separating the anterior uterine wall from the posterior bladder wall, creating the vesicouterine space, that is sharply incised during CS Parts of the uterus include: cervix (described earlier), corpus, fundus and cornua and the isthmus which forms the LUS
- Which is a branch of the uterine artery
- Peritoneum that extends beneath the fimbriated end of the fallopian tube toward the pelvic wall forms the suspensory ligament or the infundibulopelvic ligament of the ovary. This contains the ovarian artery which is a branch of the aorta. Uterosacral ligament originates with a posterolateral attachment to the supravaginal portion of the cervix and inserts into the fascia over the sacrum, forming the lateral boundaries of the pouch of Douglas.
- Pricipally supplied by the ovarian and uterine arteries. The uterine artery, a main branch of the internal iliac artery—previously called the hypogastric artery. Approximately 2 cm lateral to the cervix, the uterine artery crosses over the ureter. This proximity is of great surgical significance as the ureter may be injured or ligated during hysterectomy when the vessels are clamped and ligated.
- Once the uterine artery has reached the supravaginal portion of the cervix, it divides. A branch of considerable size extends into the upper portion of the cervix, whereas numerous other branches penetrate the body of the uterus to form the arcuate arteries. from the arcuate arteries, radial branches originate at right angles, traverse inward through the myometrium, enter the endometrium, and branch there to become basal arteries arteries extend only into the basalis layer and are not responsive to hormonal influences. or coiled spiral arteries thst supply the functionalis layer. These vessels respond to hormonal stimulation—vasoconstriction and dilatation—thus serve an important role in menstruation.
- Blood supply to the pelvis is predominantly supplied from branches of the internal iliac artery. These branches are organized into anterior and posterior divisions The anterior division provides blood supply to the pelvic organs and perineum and includes the inferior gluteal, internal pudendal, middle rectal, vaginal, uterine, and obturator arteries, as well as the umbilical artery and its continuation as the superior vesical artery. The posterior division branches extend to the buttock and thigh and include the superior gluteal, lateral sacral, and iliolumbar arteries. For this reason, during internal iliac artery ligation, many advocate ligation distal to the posterior division to avoid compromised blood flow to the areas supplied by this division.
- Ovarian artery is one of the major blood supply, venous drainage also include the ovarian veins, whereby
- Sympathetic innervation to pelvic viscera begins with the superior hypogastric plexus, also termed the presacral nerve, formed by sympathetic fbers arising from spinal levels T10 through L2. which divides into a right and a left hypogastric nerve The parasympathetic innervation to the pelvic viscera derives from neurons at spinal levels S2 through S4. These combine on each side to form the pelvic splanchnic nerves, also termed nervi erigentes. Blending of the two S and PS nerve gives rise to the inferior hypogastric plexus, also termed the pelvic plexus. Dividing into 3: The vesical plexus innervates the bladder and the middle rectal travels to the rectum, the uterovaginal plexus, also termed Frankenhäuser plexus, reaches the proximal fallopian tubes, uterus, and upper vagina.
- Lymphatics from the cervix terminate mainly in the internal iliac nodes, which are situated near the bifurcation of the common iliac vessels. The lymphatics from the uterine corpus are distributed to two groups of nodes.
- Also called oviducts, these serpentine tubes extend 8 to 14 cm from the uterine cornua and are anatomically classifed along their length as an interstitial portion, isthmus, ampulla, and infundibulum.
- In cross section, the fallopian tube contains a mesosalpinx, myosalpinx, and endosalpinx. The outer of these, the mesosalpinx, is a single-cell mesothelial layer functioning as visceral peritoneum. In the myosalpinx, smooth muscle is arranged in an inner circular and an outer longitudinal layer. The tubal musculature undergoes rhythmic contractions constantly, the rate of which varies with cyclical ovarian hormonal changes. The tubal mucosa or endosalpinx is a single columnar epithelium composed of ciliated and secretory cells resting on a sparse lamina propria. Tubal peristalsis created by cilia and muscular layer contraction is believed to be an important factor in ovum transport toward the uterine cavity
- Fossa of waldeyer is a slight depression bet the ext and int iliac vessels. The ovaries are supplied with both sympathetic and parasympathetic nerves. The sympathetic nerves are derived primarily from the ovarian plexus that accompanies the ovarian vessels and originates in the renal plexus. Others are derived from the plexus that surrounds the ovarian branch of the uterine artery. Parasympathetic input is from the vagus nerve. Sensory afferents follow the ovarian artery and enter at T10 spinal cord level.
- The ovaries are supplied with both sympathetic and parasympathetic nerves. The sympathetic nerves are derived primarily from the ovarian plexus that accompanies the ovarian vessels and originates in the renal plexus. Others are derived from the plexus that surrounds the ovarian branch of the uterine artery. Parasympathetic input is from the vagus nerve. Sensory afferents follow the ovarian artery and enter at T10 spinal cord level.
- Also called oviducts, these serpentine tubes extend 8 to 14 cm from the uterine cornua and are anatomically classifed along their length as an interstitial portion, isthmus, ampulla, and infundibulum
- Mesonephric Duct: duct of oophron; Gartner duct
- The pelvis is composed of four bones— the sacrum, coccyx, and two innominate bones. Each innominate bone is formed by the fusion of three bones—the ilium, ischium, and pubis.
- The pelvis is conceptually divided into false and true componentsdivided by the linea terminalis
- Anteriorly, the pelvic bones are joined together by the symphysis pubis, designated the arcuate ligament of the pubis. Posteriorly, the pelvic bones are joined by articulations between the sacrum and the iliac portion of the innominate bones to form the sacroiliac joints.
- Te pelvis is described as having four imaginary planes: 1. Te plane of the pelvic inlet—the superior strait. 2. Te plane of the pelvic outlet—the inferior strait. 3. Te plane of the midpelvis—the least pelvic dimensions. 4. Te plane of greatest pelvic dimension—of no obstetrical signifcance.
- We check the pelvimetry by..insering 2 gloved finger and palpate the promontory.
- We check the pelvimetry by..insering 2 gloved finger and palpate the promontory.
- The Caldwell-Moloy (1933, 1934) anatomical classifcation of the pelvis is based on shape, and its concepts aid an understanding of labor mechanisms. From viewing the four basic types, the configuration of the gynecoid pelvis would intuitively seem suited for delivery of most fetuses and was found in almost half of women.