
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Biomechanical analysis of external fixation
Ähnlich wie Biomechanical analysis of external fixation (20)
Mehr von Hiren Divecha
Mehr von Hiren Divecha (18)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Biomechanical analysis of external fixation
- 1. Cardiff School of Engineering Coursework Cover Sheet Personal Details Student No: 1056984 Family Name: Divecha First Name: Hiren Personal Tutor: Prof Sam Davies Discipline: MMM Module Details Module Name: Engineering Theory 1 Module No: ENT 536 Coursework Title: Discuss the underlying biomechanics of an external fracture fixation device and its influence on the fracture repair process Lecturer: Dr D O’Doherty Submission Deadline: 26/2/2011 Declaration I hereby declare that, except where I have made clear and full reference to the work of others, this submission, and all the material (e.g. text, pictures, diagrams) contained in it, is my own work, has not previously been submitted for assessment, and I have not knowingly allowed it to be copied by another student. In the case of group projects, the contribution of group members has been appropriately quantified. I understand that deceiving, or attempting to deceive, examiners by passing off the work of another as my own is plagiarism. I also understand that plagiarising another's work, or knowingly allowing another student to plagiarise from my work, is against University Regulations and that doing so will result in loss of marks and disciplinary proceedings. I understand and agree that the University’s plagiarism software ‘Turnitin’ may be used to check the originality of the submitted coursework. Signed: …..…………………………………….………... Date: ………………………
- 2. Discuss the underlying biomechanics of an external fracture fixation device and its influence on the fracture repair process Hiren Maganlal Divecha Candidate Number: 1056984 ENT536 – Engineering Theory 1 Word count – 3231
- 3. Abstract External fixator devices are available in many configurations and are particularly indicated in the management of complex injuries with segmental bone loss or severe soft tissue injuries. The rigidity of a simple unilateral external fixator frame can be controlled in various ways, such as changing the pin length, diameter, number per fragment and material properties. The diameter and material properties of the connecting rod will also affect the overall rigidity. The pin diameter determines the moment of inertia and therefore causes the greatest change in rigidity (radius to the fourth power). Using a analytical model proposed by Huiskes and Chao (1986), the overall vertical deflection at the fracture site (z) ranges from 0.0005 m at a pin length of 0.02 m to 0.009 m at 0.08 m (0.006 m diameter, stainless steel pins). These calculated values are within the ranges of reported values from other analytical ,experimental and finite element analyses (FEA). The importance of being able to manipulate the frame rigidity lies in the sensitivity of bone to its “mechanical environment”. Too rigid a construct will inhibit fracture healing, whereas low rigidities (and therefore high strains) will lead to fracture displacement and fibrous non-union. This has significant clinical relevance in ensuring that such fractures are managed optimally, giving the best chance of maintenance of alignment and fracture union based on the biomechanical understanding of external fixator frame rigidity.
- 4. Contents Abstract ................................................................................................................................................... 3 1. Introduction .................................................................................................................................... 1 2. Analysis of a unilateral fixator......................................................................................................... 3 a. Deflection due to pin bending .................................................................................................... 6 b. Overall frame deflection ........................................................................................................... 10 3. Discussion...................................................................................................................................... 12 a. Fixator frame rigidity................................................................................................................. 12 b. Effect on fracture healing ......................................................................................................... 14 4. Conclusion ..................................................................................................................................... 16 5. Bibliography .................................................................................................................................. 17 6. Appendices .................................................................................................................................... 19 a. Appendix 1 – Nomenclature ..................................................................................................... 19 b. Appendix 2 – Abbreviations ...................................................................................................... 19
- 5. 1. Introduction An external fixator is a device that allows for the reduction and maintenance of fracture alignment using pins or wires inserted into the fracture fragments and connected to an external frame setup. The main indications for the use of an external fixator for fracture management includes (Giotakis and Narayan 2007) (Moss and Tejwani 2007): 1. Temporary/ emergency stabilisation of life/ limb threatening injuries (ie: “damage control surgery” (Roberts, Pape and Jones 2005)) 2. Temporary fracture stabilisation in fractures with a severe soft tissue injury 3. Definitive fracture management 4. Limb reconstruction procedures 5. Treatment of non-unions and osteomyelitis There are many frame configurations that can be used, each with pros and cons. The simpler setups allow for ease of application, are less bulky but may offer less rigidity or fragment control. The more complex setups (such as Ilizarov fine wire-ring configurations) are technically more difficult to apply, but offer greater control over fracture fragments: 1. Unilateral / bilateral 2. Multiplanar 3. Ring fixator (eg: Ilizarov) 4. Hybrid (ring-unilateral) External fixators behave as load sharing devices and as the fracture heals and becomes more rigid, it will take a greater proportion of the load compared to the external fixator. The rigidity of the external fixator will affect the fracture repair process. Initially, a more rigid fixation will prevent fracture fragment displacement and maintain alignment. However if the construct is too rigid there 1
- 6. will be minimal fracture strain and minimal callus formation, as per Perren’s Strain Theory (S. M. Perren 1979). Conversely, a too flexible construct will lead to loss of alignment and a non-union or fibrous union because the fracture strain is too high, resulting in inhibition of callus formation. The overall external fixator frame rigidity can be manipulated by changing certain variables. This is important clinically in ensuring that a fracture remains well aligned during the healing process and to ensure that the fracture is “stimulated” enough to undergo secondary healing through callus formation. The following analyses demonstrate the effect on vertical deflection of an axially loaded, unilateral external fixator frame by altering some of the variables such as pin length, diameter and material. 2
- 7. 2. Analysis of a unilateral fixator For the following analyses, the example of a mid-tibial shaft fracture stabilised with a unilateral external fixator shall be used (see Figure 1). The stiffness of the external fixator construct depends on a number of variables including: 1. Pin a. Number per fracture segment b. Spacing (between pins on a fragment and across the fracture site) c. Length d. Diameter e. Material 2. Connecting rod a. Number (ie: stacked one on top of each other on the same pins) b. Spacing from bone c. Length d. Diameter e. Material 3. Bi-/ multi planar set ups 3
- 8. F rrod a Pin b Fracture d c Clamp F Connecting Rod Figure 1: Schematic representation of tibial shaft fracture with unilateral external fixator applied with 2 pins per fracture segment. (a – effective pin length (m); b – pin separation (m); c- pin separation at fracture site (m); d – effective pin separation (m); rrod – radius of connecting rod (m); F – ½ body weight (N)) 4
- 9. The effect of altering some of these variables on frame stiffness shall be explored further. Ideally, a finite element analysis (FEA) would allow a more realistic modelling of the external fixator/ fracture construct and thus give accurate results of frame stiffness under different modes of loading (axial, bending, torsion). A simpler static analysis shall be used here with the following assumptions made to allow for ease of calculation: 1. All pin – bone interfaces are tight and axial load is shared equally between the pins in each fracture fragment 2. Deformation of the bone at the pin – bone interface is presumed to be negligible 3. There is no contact between the fracture ends 4. The pin – connecting rod clamp interface is presumed to be rigid, thus no bending occurs here 5. The construct is loaded in axial compression with a force of half body weight (F = 400N) to simulate standing on both legs (body weight = 80 kgs; acceleration due to gravity = 10 m.s-2) 6. An equal and opposite ground reaction force acts upwards on the distal fracture segment as noted in Figure 1. 5
- 10. a. Deflection due to pin bending The deflection of the pin shall be analysed first in isolation from the connecting bar. Figure 2 a) represents one pin-clamp-connecting rod unit modelled as a cantilever beam, with the pin being rigidly fixed at the clamp-connecting rod end and subjected to a load at the free end. As the axial load F (ie: ½ body weight) is shared equally between the pins in each fracture fragment, the pin is subjected to F/2 (ie: 200 N). This is uniformly distributed over the length of the pin within the tibia (x) (approximately 0.02 m for an adult tibia). The load per unit length is represented by ω (ie: 10000 N.m-1). Instead of bending uniformly, the segment of the pin within the tibia will remain relatively straight provided the pin remains tight and the bone is of good quality to withstand the pin-bone interface stresses without deformation. An approximation of the vertical deflection due to bending (y) under axial load can be taken at the point where the pin enters the bone (ie: x m from the free end of the pin). ω a) x a ω b) y Figure 2: Representation of single pin-clamp-connecting rod unit modelled as a cantilever beam with uniformly distributed axial load at the free end (x – pin length within tibia (m); y – vertical deflection due to bending (m); -1 ω – load per unit length on pin within tibia (N.m )) 6
- 11. The vertical deflection (y) at the point where the pin enters the bone is given by the following equation, where l is the overall length of the pin (x + a), rpin is the radius of the pin, Epin is the Young’s modulus of elasticity of the pin and Ipin is the moment of inertia of the pin: For a 0.006 m diameter pin made of stainless steel (Young’s modulus 200 GPa) with an overall length of 0.07 m, the vertical deflection (y) is 0.0003 m. Each pin in a fracture segment is presumed to deflect by the same amount (given that they each experience a similar load, are of same dimensions and are made of the same material). The total deflection or movement at the fracture site for this setup will be 0.0006 m as the bottom fracture fragment will deflect superiorly under axial load due to the equal and opposite ground reaction force. Figure 3 is a graphical plot of vertical deflection (y) vs overall length of the pin (l) for varying pin diameters (0.004 m, 0.005 m, 0.006 m, 0.007 m). The minimum overall pin length is realistically 0.04 m (0.02 m within the tibia and 0.02 m accounting for overlying soft tissues), which would involve the connecting rod and clamps being right up against the skin. As the diameter is increased, the vertical deflection reduces. As the overall pin length increases, the bending deflection increases. 7
- 12. 4 3.5 3 Vertical Deflection "y" (mm) 2.5 Pin Diameter 4 mm 2 5 mm 1.5 6 mm 7 mm 1 0.5 0 0.03 0.04 0.05 0.06 0.07 0.08 0.09 0.1 Pin Length "l" (m) Figure 3: Graphical plot of vertical deflection (y) vs pin length (l) for different diameter pins Altering the material and thus the Young’s modulus of elasticity of the pin (Epin) will also affect the amount of deflection that occurs as shown in Figure 4, which shows the vertical displacement with increasing pin length for different pin materials (titanium, carbon fibre/polyetheretherketone (CF/PEEK) and stainless steel) of 0.006 m diameter. 8
- 13. 1.6 1.4 1.2 Vertical Deflection "y" (mm) 1 Pin Material (Young's Modulus) 0.8 Titanium (100 GPa) CF/ PEEK (140 GPa) 0.6 Stainless Steel (200 GPa) 0.4 0.2 0 0.03 0.04 0.05 0.06 0.07 0.08 0.09 0.1 Pin Length "l" (m) Figure 4: Graphical plot of vertical deflection (y) vs pin length (l) for different material pins of 0.006 m diameter 9
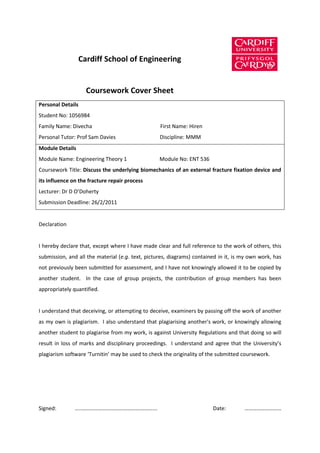
- 14. b. Overall frame deflection The bending of the connecting rod cannot be realistically ignored, as it will contribute to the overall vertical displacement occurring at the fracture site. Huiskes and Chao (1986) (Huiskes and Chao 1986) suggested the following equation to represent the overall frame rigidity (with all pins tight) based on beam theory (kf – frame rigidity (N.m-1); m – number of pins per fracture segment; z – overall vertical deflection at fracture site (m)): Thus in terms of z: Figure 5 is a graphical plot of the vertical deflection at the fracture site (z) vs pin length using the above equation (diamond marker) for a fixator with a 0.008 m diameter connecting rod made of stainless steel with two stainless steel pins (varying diameter) per fracture fragment spaced 0.08 m apart and a 0.04 m gap between the two near-fracture pins. The equation proposed by Huiskes & Chao (Huiskes and Chao 1986) predicts higher fracture site deflections under these conditions. 10
- 15. 16 14 12 Vertical Deflection "z" (mm) 10 4 mm 8 5 mm 6 6 mm 7 mm 4 2 0 0.03 0.04 0.05 0.06 0.07 0.08 0.09 0.1 Pin length "l" (m) Figure 5: Graphical plot of vertical deflection at fracture site (z) vs pin length (l) for combined pin and connecting rod analysis according to pin diameter 11
- 16. 3. Discussion a. Fixator frame rigidity The results of the analyses above demonstrate in a simple manner that the overall rigidity of the external fixator setup can be varied by altering certain factors. The pin diameter and hence the moment of inertia of the pin makes the biggest contribution (as the radius to the fourth power determines the moment of inertia) – smaller diameter pins have greater vertical deflections under load compared to larger diameter pins (as shown in Figure 3). If we take the example of a pin with an effective length (x) of 0.05 m (ie: overall length (l) = 0.07 m), the vertical deflection of one stainless steel pin in this analysis is 0.0016 m (0.004 m pin), 0.0007 m (0.005 m pin), 0.0003 m (0.006 m pin) and 0.0002 m (0.007 m pin). The most commonly used external fixator pins for adult long bones are Schanz pins, which are usually 0.006 m in diameter. Pin diameters that exceed 1/3rd of the tibial diameter run the risk of stress raiser effect and fractures in torsion after pin removal (Behrens 1989) (Edgerton, An and Morrey 1990). Increasing the pin length also leads to an increased vertical deflection as shown in Figure 3. Thus for a 0.006 m diameter stainless steel pin, the vertical deflection (y) increases from 0.00009 m at an effective length of 0.02 m (which would clinically represent the connecting bar being right against the skin) to 0.0007 m at 0.08 m. Whilst the simplistic analysis performed in Section 2 a. gives a good representation of how the pins used can alter the vertical deflection under load, it is far from being a representative model of the in vivo scenario. The equation suggested by Huiskes and Chao (Huiskes and Chao 1986) (Figure 5) attempts to take into consideration other variable factors including the number of pins per fracture segment (m) and the separation between the centres of the inter-pin spacing between each fracture segment. They compared the results of fixator rigidity using this equation with those generated by an FEA and found a very close agreement between the two. The overall vertical deflection at the 12
- 17. fracture site (z) ranges from 0.0005 m at a pin length of 0.02 m to 0.009 m at 0.08 m (0.006 m diameter stainless steel pins, 0.008 m diameter stainless steel connecting rod). These results are nearly consistent to those obtained by other authors using both FEA and experimental models. Goodship et al (Goodship, et al. 1993) used ovine tibiae osteotomised, fixed with a unilateral stainless steel external fixator using three 0.006 m diameter stainless steel pins per fracture fragment. In vitro testing of vertical displacement under axial loading was performed with effective pin lengths of 0.025 m and 0.035 m. The corresponding displacements under 400 N load were approximately 0.0006 m and 0.0008 m respectively. Using the equation suggested by Huiskes and Chao, the vertical displacements are 0.0007 m and 0.0015 m respectively (after correcting for the use of 3 pins per fracture segment as used by Goodship et al.). A similar loading experiment performed on acrylic bone models performed by Kristiansen et al (Kristiansen, et al. 1987) using a unilateral external fixator with two 0.005 m diameter pins per fracture fragment at an effective pin length of 0.025 m resulted in an average stiffness of 132 N.mm -1, which would represent a vertical deflection of 0.003 m under a 400 N load. The equivalent variables used with Huiskes’ equation would give a vertical deflection of 0.0008 m. The large difference here could be due to the differences in the connecting rod rigidity and the pin spacing, which is not mentioned in Kristiansen et al’s report. An FEA performed by Oni et al (Oni, Capper and Soutis 1993) analysed the effect of pin distribution on each fracture fragment (3 pins per fragment, effective pin length 0.05 m). They found a vertical deflection of 0.0023 m with the pins spread out evenly favouring the fracture site, which again compares favourably to the results of the equation proposed by Huiskes and Chao (0.0032 m). Altering the material, and thus the Young’s modulus of elasticity, of the pins does make a little difference in the calculated vertical deflections as represented in Figure 4. The stainless steel pins show smaller deflections than titanium or carbon fibre ones. In practice, stainless steel pins are usually used to withstand the pin-bone interface stresses (Huiskes, Chao and Crippen 1985) 13
- 18. (Fragomen and Rozbruch 2007) (Giotakis and Narayan 2007) (Moss and Tejwani 2007). There are advantages to using CF/PEEK in the connecting rods: 1. Lightweight compared to stainless steel 2. Radiolucent – x-rays can be taken without obscuring the fracture site 3. High strength – higher load to failure under bending compared to stainless steel rods (Kowalski, et al. 1996) b. Effect on fracture healing Bone is a “mechanically sensitive” tissue and will remodel according to applied stresses, as per Wolff’s Law (Maquet and Furlong 1986). With respect to the fracture healing process, a similar “sensitivity” to the mechanical environment has also been noted from work done in animal studies (S. M. Perren 1979) (Goodship, et al. 1993). Kenwright and Goodship (Kenwright and Goodship 1989) showed in an in vivo study of tibial fractures that lower strains (17%) resulted in callus formation whereas higher strains (67%) inhibited callus formation. In Goodship et al’s (Goodship, et al. 1993) report of fracture healing with an external fixator in a sheep model, an increased frame rigidity (achieved by reducing the effective pin length) resulted in a significantly reduced rate of healing when compared to a more flexible external fixator setup (longer effective pin length). The formation of callus in indirect or secondary fracture healing will occur in the setting of relative stability (ie: not too rigid and not too flexible fixation). Claes et al (Claes, Heigele and Neidlinger-Wilke, et al. 1998) performed a series of animal experiments and cell culture studies to study the effect of fracture motion and strain on healing and on osteoblast activity. They suggested that fracture gap movement should be between 0.0002 – 0.001 m in amplitude to allow for callus formation in transverse fractures, but should not exceed 0.002 m. Strains between 5 -15% resulted in callus formation. At less than 5%, intramembranous bone healing occurred (ie: primary/ direct healing). Strains greater than 15% resulted in fibrous tissue formation. 14
- 19. Direct or primary bone healing occurs in the setting of rigid fixation following anatomic fragment reduction (S. Perren 2002). For this to proceed, the fracture strain must be less than 2 – 5% (ie: rigid fixation) (Mann and Payne 1989) (Claes and Heigele, Magnitudes of local stress and strain along bony surfaces predict the course and type of fracture healing 1999). No callus formation occurs and the fracture heals by Haversian remodelling across the fracture site. Callus formation allows quicker fracture healing, though not as anatomical as primary/ direct healing. Thus, the ideal scenario would involve the external fixator setup initially being stiff enough to maintain the overall alignment and allow early weight bearing. As fracture healing progresses and the callus becomes more rigid, it will bear more of the load. At this stage, the external fixator should be made less rigid to allow some fracture strain which will stimulate callus formation (Goodship, et al. 1993) (Claes, Heigele and Neidlinger-Wilke, et al. 1998) (Fragomen and Rozbruch 2007). If the fixator frame remained too rigid, it would result in a stress/ strain shielding effect leading to a delayed or a non-union as fracture healing would be inhibited. Reducing the external fixator rigidity could be achieved by: 1. Removing some pins 2. Removing stacked connecting rods 3. Increasing the effective pin length 4. Dynamising the fracture (ie: loosening the connecting rod and allowing the fracture ends to impact into each other 15
- 20. 4. Conclusion The analyses presented here demonstrate the effect on external fixator rigidity of altering pin length, diameter and material properties. The calculated vertical deflections are within the ranges quoted in the literature from analytical, FEA and experimental studies (Goodship, et al. 1993) (Huiskes and Chao 1986) (Kristiansen, et al. 1987) (Oni, Capper and Soutis 1993). It is clear from the discussion of the effect of the “mechanical environment” on fracture healing that altering the external fixator rigidity will result in changes in the fracture strain and thus influence fracture healing (Claes, Heigele and Neidlinger-Wilke, et al. 1998) (Kenwright and Goodship 1989) (S. Perren 2002). This is important clinically on the outcome of treatment. Too rigid a frame, whilst maintaining excellent alignment and allowing earlier weight-bearing, will result in a delayed/ non- union because of inhibition of osteoblast function. Conversely, a frame that is too flexible may leading to fracture displacement and the resulting high facture strain will also inhibit osteoblast function leading to fibrous tissue formation. The ideal external fixator rigidity remains unknown. The principle of allowing an initially rigid construct to prevent fracture displacement, followed by gradual reduction in the fixator stiffness to allow increased fracture strain (and reduce the stress/ shielding effect) and thus stimulate callus formation and fracture repair seems to represent the best compromise. This is easily achievable in the out-patient department given the versatility and easy manipulation of external fixator frames. 16
- 21. 5. Bibliography Behrens, F. “A primer of fixator devices and configurations.” Clin Orthop Rel Res 241 (1989): 5-15. Claes, L E, and C A Heigele. “Magnitudes of local stress and strain along bony surfaces predict the course and type of fracture healing.” J Biomech 32 (1999): 255-266. Claes, L E, et al. “Effects of Mechanical Factors on the Fracture Healing Proces.” Clin Orthop Relat Res 355 (Suppl) (1998): S132-S147. Edgerton, B C, K N An, and B F Morrey. “Torsional strength reduction due to cortical defects in bone.” J Orthop Res 8 (1990): 851-855. Fragomen, A T, and R Rozbruch. “The mechanics of external fixation.” HSSJ 3, no. 1 (2007): 13-29. Giotakis, N, and B Narayan. “Stability with unilateral external fixation in the tibia.” Strat Traum Limb Recon 2, no. 1 (2007): 13-20. Goodship, A E, P E Watkins, H S Rigby, and J Kenwright. “The role of fixator frame stiffness in the control of fracture healing. An experimental study.” J Biomech 26, no. 9 (1993): 1027-1135. Huiskes, R, and E Y S Chao. “Guidelines for external fixation frame rigidity and stresses.” J Orthop Res 4, no. 1 (1986): 68-75. Huiskes, R, E Y S Chao, and T E Crippen. “Parametric analyses of pin-bone stresses in external fracture fixation devices.” J Ortho Res 3, no. 3 (1985): 341-349. Kenwright, J, and A E Goodship. “Controlled mechanical stimulation in the treatment of tibial fractures.” Clin Orth and Rel Res 241 (1989): 36-47. Kowalski, M, E H Schemitsch, R M Harrington, and J R Chapman. “Comparative biomechanical evaluation of different external fixation sidebars: Stainless-steel tubes versus carbon fiber rods.” J Orthop Trauma 10, no. 7 (1996): 470-475. Kristiansen, T, B Fleming, G Neale, S Reinecke, and M H Pope. “Comparative study of fracture gap motion in external fixation.” Clin Biomech 2, no. 4 (1987): 191-195. 17
- 22. Mann, F A, and J T Payne. “Bone Healing.” Semin Vet Med Surg (Small Anim) 4, no. 4 (1989): 312- 321. Maquet, P, and R Furlong. The law of bone remodelling. Berlin: Springer-Verlag, 1986. Moss, D P, and N C Tejwani. “Biomechanics of external fixation: A review of the literature.” Bull NYU Hosp Jt Dis 65, no. 4 (2007): 294-299. Oni, O O A, M Capper, and C Soutis. “A finite element analysis of the effect of pin distribution on the rigidity of a unilateral fixation system.” Injury 24, no. 8 (1993): 525-527. Perren, S. “Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation: choosing a new balance between stability and biology.” J Bone Joint Surg [Br] 84, no. 8 (2002): 1093-1110. Perren, S M. “Physical and biological aspects of fracture healing with special reference to internal fixation.” Clin Orthope Relat Res 138 (1979): 175-196. Roberts, C S, H-C Pape, and A L Jones. “Damage control orthopaedics. Evolving concepts in the treatment of patients who have sustained orthopaedic trauma.” JBJS [Am] 87 (2005): 434- 449. 18
- 23. 6. Appendices a. Appendix 1 – Nomenclature Symbol Quantity SI Unit a effective pin length m b pin separation m c pin separation at fracture site m d effective pin separation m Epin Young’s modulus of elasticity of pin GPa Erod Young’s modulus of elasticity of GPa connecting rod F ½ body weight N Ipin Moment of inertia of pin m4 Irod Moment of inertia of pin m4 kf frame rigidity N.m-1 l Overall length of pin (ie: a + x) m m number of pins per fracture segment rpin Radius of pin m rrod radius of connecting rod m X pin length within tibia m y vertical deflection due to bending m z overall vertical deflection at fracture m site (ie: 2 * y) ω load per unit length on pin within N.m-1 tibia b. Appendix 2 – Abbreviations Abbreviation Full term FEA Finite element analysis 19
- 24. CF/ PEEK Carbon fiber/ polyetheretherketone 20