spinal cord
•Als PPTX, PDF herunterladen•
19 gefällt mir•3,044 views

anatomy and functions of spinal cord

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie spinal cord
Ähnlich wie spinal cord (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
spinal cord
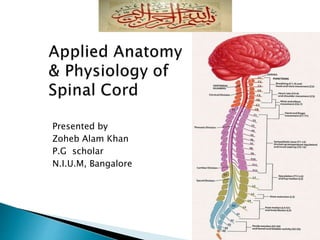
- 1. Presented by Zoheb Alam Khan P.G scholar N.I.U.M, Bangalore
- 2. Nervous system: an overview Spinal cord Regions of Spinal cord Meninges of Spinal cord Cross section of Spinal cord Nuclei of Spinal cord Tracts of Spinal cord Spinal nerves Nerve plexus Spinal cord injuries Unani Concept
- 3. 1. Collection of sensory input 2. Integration of sensory input 3. Motor output Functions of Nervous System
- 4. Central Nervous System (CNS) = brain and spinal cord Peripheral Nervous System (PNS) = nerves CNS PNS
- 5. Brain and Spinal Cord Occupy Dorsal Cavity
- 6. Part of the CNS About 18 Inches (45 cm) long in male, and 43 cm in female with the diameter of ¾(2 cm) Extends from the foramen magnum to the end of L1 (adults) and L3-L4 (infants) Main pathway for information flow to and from the brain Spinal cord is made up of a core of gray matter surrounded by white matter
- 7. Cervical Thoracic Lumbar Sacral Coccygeal Cervical + Lumbar enlargements Conus medullaris Filum terminale Cauda equina
- 9. Pia mater (pia=delicate,mater=mother) (deep) ◦ delicate ◦ highly vascular,Adheres spinal cord tissue Arachnoid mater (arachne=spider) (middle) ◦ impermeable layer = barrier Spinal Dura Mater (dura=tough) (most superficial) ◦ single dural sheath Subarachnoid Space ◦ between arachnoid and pia mater ◦ contains CSF Epidural Space ◦ Between dura mater and vertebra ◦ Contains fat and veins Subdural space Between dura and arachnoid mater
- 11. Anterior median fissure and posterior median sulcus ◦ deep clefts partially separating left and right halves Gray Matter ◦ “H” shaped Inner core ◦ Gray Commissure = crossbar of “H” ◦ Central Canal = in gray commissure ◦ Posterior/Dorsal horns ◦ Anterior/Ventral horns Composed of ◦ Cell bodies ◦ Unmyelinated axons ◦ Dendrites ◦ Neuroglia
- 13. Posterior Horn is made up of interneurons which transmit information from cell bodies situated outside of spinal cord into the spinal cord. ◦ Dorsal Root contains Sensory Fibers Somatic Sensory (SS) Visceral Sensory (VS) ◦ Dorsal Root Ganglia-swelling in the dorsal root through which these interneurons pass. Anterior Horn is made up of cell bodies of motor neurons that send axons out of spinal cord to muscles and glands. ◦ Ventral Root contains Motor Fibers Visceral Motor Somatic Motor
- 14. Nuclei in Anterior Gray Horn: The nuclei in the anterior horn innervate the skeletal muscles. The nuclei of anterior horn are divided into 3 groups. Medial Group : Present throughout entire extent of spinal cord & innervates axial muscles of the body Lateral Group: is present in cervical & lumbar enlargements & supplies musculature of limbs. It is further divided into 3 subgroups: (a) Anterolateral supplying proximal muscles of limb [shoulder & arms / gluteal region & thigh] [b] Posterolateral supplying intermediate muscles of limbs [forearm / leg] [c] Post posterolateral: innervates distal segment {hand / foot] Central Group: Only in cervical region as phrenic nerve nucleus and nucleus of accessory nerve
- 16. Nuclei in Lateral column Inter mediomedial nucleus Intermediolateral nucleus Nuclei in Posterior column Posteromarginal Nucleus : Thin Layer of neurons 1. Substantia Gelatinosa: acts as relay station for pain & temperature fibres & gives rise to lateral spino-thalamic tract. 2. Nucleus Proprius : Concerned with sensory associative mechanism 3. Nucleus Dorsalis : Also k/s Thoracic nucleus. It relays nuclear column for reflex or unconscious proprio-ceptive impulses to cerebellum & its axons give rise to spino-cerebellar tract
- 17. ◦ Surrounds gray matter ◦ White columns Posterior funiculus Anterior funiculus Lateral funiculus ◦ Axons in white matter are: Myelinated axons Unmyelinated axons Function: Allows communication between parts of spinal cord, and between brain + spinal cord Two main types of nerve fibers ◦ Ascending: carry SENSORY info from body to brain (eg) touch, pressure, pain, temperature, ◦ Descending: carry MOTOR info from brain to spinal cord (eg) control precise, skilled movement = writing, maintain balance, create movement
- 18. Group of nerve fibres passing through spinal cord are k/s Tracts. They are divided into two main groups: 1 . Short tracts : Fibers of this tracts connect fibers of spinal cord itself. [a] Association or intrinsic tracts which connect adjacent segments of spinal cord on the same side. [b] Commissural tracts which connect opposite halves of same segment of spinal cord. 2. Long tracts : Also k/s Projection tracts. They connect the spinal cord with other parts of CNS. They are of 2 types: [a] Ascending tracts [b] Descending tracts
- 20. Ascending (afferent) spinal tracts • Pathways that carry sensory information to a conscious level Basic principle of information flow: • receptor (e.g. pain receptor in skin) • primary sensory neurone (cell body in dorsal root ganglia) • second order neurone (in the spinal cord or brainstem) • third order neurone (in thalamus) • target area: cortex somatosensory (somatic sensory) area (postcentral gyrus) of the cortex Note:- All the ascending tracts are formed by second order neuron except posterior white funiculus which are formed from first order neuron
- 21. Name Location Function Fasciculus gracilis Posterior Column Discriminative touch, proprioception Weight discrimination Fasciculus Cuneatus Posterior Column Same as FG Lateral Spinothalamic Lateral Column Pain and Thermal sensations Anterior Spinothalamic Anterior Column Itch, Tickle, Pressure, Crude touch sensations Posterior and Anterior Spinocerebellar Lateral Column Proprioceptors
- 22. Anterior spinothalamic tract: Crossed , Unilateral lesion Loss of crude touch in opposite side, B/L lesion loss of crude touch & sensations like itching & tickling both sides. Lateral spinothalamic tract : Crossed, Unilateral lesion Loss of pain & temp. sensation in opposite side below the level of lesion , B/L lesion loss of pain & temp.sensations on both sides below the level of lesion Ventral Spinocerebellar tract : k/s Grower tract ,Crossed Lesion leads to loss of subconscious kinesthetic sensations in the opposite side. Dorsal Spinocerebellar tract: Uncrossed, Unilateral loss of the subconscious kinesthetic sensations on the same side Spinotectal tract: Crossed, Concerned with spinovisual reflex Fasciculus Dorsolateralis: k/s tract of lissauer, Uncrossed. Carries impulses of pain & thermal sensations Spinoreticular tract: Crossed Components of ascending RAS, concerned with consciousness and awareness
- 23. Spino- Olivary tract : Crossed Concerned with proprioception Spinovestibular tract : Concerned with proprioception Fasciculus Gracilis (Tract of Goll ] And Fasciculus Cuneatus [Tract of Burdach] :Uncrossed , Loss of tactile sensation, localization, point discrimination, vibrations, astereognosis,proprioception,Sensory ataxia on the same side below the lesion Comma tract of Schultze : To establish intersegmental communications and to form short reflex arc.
- 26. They are formed by nerve fibers arising from the brain and decend into the spinal cord. They carry motor impulses from brain to the spinal cord. They are of 2 types: [1] Pyramidal Tracts: Also k/s Corticospinal tract which descend from cerebral cortex to spinal cord. They are concerned with voluntary movements of the body and are responsible for fine skilled movements. They form upper motor neurons. There are 2 coticospinal tracts :- Anterior corticospinal tract, Crossed & Lateral corticospinal tract, Uncrossed Effects of lesion at different level: Cerebral cortex: Causes hypertonia, spasticity & contralateral monoplegia or contralateral hemiplegia Internal capsule: Contralateral hemiplegia Brainstem: Contralateral hemiparesis along with VI and VII nerve palsies, Spinal cord: Unilateral lesion in upper cervical region ipsilateral hemiplegia B/L lesion causes quadriplegia with paralysis of respiratory muscles
- 27. B/L lesion of these fibres in thoracic and lumbar region causes paraplegia with paralysis of respiratory muscles. Extrapyramidal tracts: Medial longitudinal fasciculus: Uncrossed Lesion affects reflex ocular & reflex neck movements Anterior & Lateral Vestibulospinal tract: Uncrossed Lesion affects muscle tone & posture, adjustment of position of head & body becomes difficult during acceleration Reticulospinal tract: Uncrossed Lesion causes disturbances in respiration, B.P , movements of body & muscle tone Rubrospinal tract: Crossed They exhibit facilitatory influence upon flexor muscle tone. Tectospinalspinal tract: Crossed It is responsible for movement of head in response to auditory & visual reflex. Olivospinal tract: Uncrossed Invoved in reflex movements arising from proprioreceptors.
- 29. Each pair of nerves located in particular segment (cervical, thoracic, lumbar, etc.) Each nerve pair is numbered for the vertebra sitting above it (i.e. nerves exit below vertebrae) ◦ 8 pairs of cervical spinal nerves; *C1-C8 ◦ 12 pairs of thoracic spinal nerves; T1-T12 ◦ 5 pairs of lumbar spinal nerves; L1-L5 ◦ 5 pairs of sacral spinal nerves; S1-S5 ◦ 1 pair of coccygeal spinal nerves; C0
- 31. Ventral rami (branches) of various spinal nerves blend together to form an interwoven network of nerves, nerve plexus Four major plexuses ◦ Cervical ◦ Brachial ◦ Lumbar ◦ Sacral
- 32. Ventral rami of C1-C4 with a few fibers from C5 Innveration of muscles of the neck, shoulder and upper breast Phrenic nerve – innervation of diaphragm Brachial plexus Axillary nerve Radial nerve Musculocutaneous nerve Median nerve Ulnar nerve
- 36. Spinal Cord Trauma and Disorders • Severe damage to ventral root results in flaccid paralysis • Skeletal muscles cannot move either voluntarily or involuntarily • Without stimulation, muscles atrophy. • When only UMN of primary motor cortex is damaged • Spastic paralysis occurs - muscles affected by persistent spasms and exaggerated tendon reflexes • Muscles remain healthy longer but their movements are no longer subject to voluntary control. • Muscles commonly become permanently shortened. • Transection (cross sectioning) at any level results in total motor and sensory loss in body regions inferior to site of damage. • If injury in cervical region, all four limbs affected (quadriplegia) • If injury between T1 and L1, only lower limbs affected (paraplegia) •Spinal shock - transient period of functional loss that follows the injury • Results in immediate depression of all reflex activity caudal to lesion. • Bowel and bladder reflexes stop, blood pressure falls, and all muscles (somatic and visceral) below the injury are paralyzed and insensitive. • Neural function usually returns within a few hours following injury
- 38. Spinal Cord Trauma and Disorders •Amyotrophic Lateral Sclerosis (aka, Lou Gehrig’s disease) • Progressive destruction of anterior horn motor neurons and fibers of the pyramidal tracts • Lose ability to speak, swallow, breathe. • Death within 5 yrs • Cause unknown (90%); others have high glutamate levels • Poliomyelitis • Virus destroys anterior horn motor neurons • Victims die from paralysis of respiratory muscles • Virus enters body in feces-contaminated water (public swimming pools] •Syringomyelia • Dilatation in central canal of spinal cord mainly in cervical region. • Decussating fibres of pain and temp are affected but touch and proprioception is present
- 39. Upper Motor Neuron (UMN) vs Lower Motor Neuron (LMN) Syndrome UMN syndrome LMN Syndrome Type of Paralysis Spastic Paresis Flaccid Paralysis Atrophy No (Disuse) Atrophy Severe Atrophy Deep Tendon Reflex Increase Absent DTR Pathological Reflex Positive Babinski Sign Absent Superficial Reflex Absent Present Fasciculation and Absent Could be Fibrillation Present
- 40. UNANI CONCEPT •Zakariya Razi in his book Kitab ul Mansuri (810-895AD) has mentioned spinal cord, spinal nerve and their functions. •Ali Ibn Abbas Majusi in his book Kamil -us-Sana (930-999AD) has described spinal cord briefly: Spinal cord takes origin from brain is covered by two membrane If injury occurs in spinal cord, then other organs also get affected but he did not describe the spinal nerves. •Ibn e Sina in his book Al-Qanoon(980-1037AD) described spinal cord in term of Its full course , origin, classification, and its supply to target organs He told that the cervical has eight pair of nerves, while thoracic has twelve pair of nerves He has dedicated a fresh chapter for the description of cervical spinal nerve.
- 41. Ibn-e-Rush’d in his book Kitabul Kulliyat (1126-1198AD) also described that nerve arises from spinal cord. Abul Sahal Masihi in his book Kitabul Mi’a Spinal cord has 29 pair of nerves emerging between two vertibrae: 8 cervical, 12 thorasic,5 lumber,4 cocyx