Breech presentation
•Als PPTX, PDF herunterladen•
50 gefällt mir•13,341 views

Seminar presentation

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Breech presentation
Ähnlich wie Breech presentation (20)
Mehr von yuyuricci
Mehr von yuyuricci (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Breech presentation
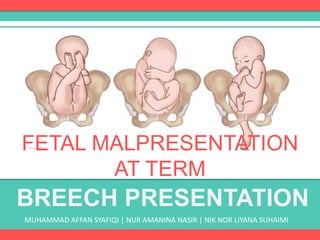
- 1. BREECH PRESENTATION MUHAMMAD AFFAN SYAFIQI | NUR AMANINA NASIR | NIK NOR LIYANA SUHAIMI FETAL MALPRESENTATION AT TERM
- 2. WHAT IS BREECH? Malpresentation is a presentation that is not cephalic The most commonly encountered malpresentation in pregnancy is breech presentation Breech means that your baby is lying bottom first or feet first in the womb (uterus) instead of in the usual head first position. As pregnancy continues, a baby usually turns naturally into the head first position.
- 3. INCIDENCE This presentation occurs in: 1. 3-4% of term pregnancies. 2. 7% of pregnancies at 32 weeks 3. 25% of pregnancies of less than 28 weeks’
- 4. TYPES OF BREECH FRANK BREECH FOOTLING BREECHCOMPLETE BREECH Extended or frank breech – the baby is bottom first, with the thighs against the chest and feet up by the ears. Most breech babies are in this position (most common) Flexed breech – the baby is bottom first, with the thighs against the chest and the knees bent Footing breech – the baby’s foot or feet are below the bottom A BREECH BABY MAY BE LYING IN ONE OF THE FOLLOWING POSITIONS
- 5. WHY ARE SOME BABIES BREECH? Sometimes it’s just a matter of chance that a baby does not turn and remains the breech position. At other times, certain factors make it difficult for a baby to turn during pregnancy. These might include the amount of fluid in the womb (either too much or too little), the position of placenta or if there’s any more than one baby in the womb. The vast majority of breech babies are born healthy. For a few babies, breech may be a sign of a problem with the baby
- 6. PREDISPOSING FACTORS MATERNAL FETAL / PLACENTAL Fibroids Congenital uterine abnormalities Uterine surgery Multiple Gestation Prematurity Placenta praevia Abnormality, e.g. anencephaly or hydrocephalus Fetal neuromuscular condition Oligohydramnios Polyhydramnios
- 7. DIAGNOSIS • The diagnosis of breech presentation may be made by: 1. Abdominal palpation 2. Vaginal examination 3. Confirmed by ultrasound If breech presentation is clinically suspected at or after 36 weeks, this should be confirmed by ultrasound scan. The scan should document fetal biometry, amniotic fluid volume, placental site and position of fetal legs. The scan should also look for any anomalies previously undetected.
- 8. CLINICAL DIAGNOSIS• Palpation – Fundal grips; the head is felt with its characters. – Pelvic grip; the breech is felt, with its characters. • Auscultation – The fetal heart sounds are head just at, or above the level of the umbilicus • Slow dilatation of cervix • After rupture of the membranes, the presenting part is felt that is , the two buttocks with the anus in between , the genitalia on one side and the sacral spines on the opposite side. • In case of complete breech, the feet are felt on the same level as the buttocks. • In case of breech with extended legs, the buttocks only are felt. • In case of footling presentation, the feet are at a lower level than the buttocks. • In case of knee presentation, the knees are a lower level than the buttocks. ABDOMINAL EXAMINATION VAGINAL EXAMINATION
- 10. MANAGEM ENT 1.EXTERNAL CEPHALIC VERSION 2.Vaginal delivery 3.Lower segment caesarean section
- 11. MANAGEMENT ECV is a relatively straightforward and safe technique and has been shown to reduce the number of Caesarean sections due to breech presentations. Should be offered at 36-37 weeks of pregnancy. Success rate is around 50 per cent and are higher in multiparous women who tend to have more lax abdominal musculature. However it depends on the experience of the obstetrician. A fetal heart rate trace must be performed before and after the procedure. It is important to administer anti-D if the woman is Rhesus- negative. 1. EXTERNAL CEPHALIC VERSION
- 12. MANAGEMENT 1. EXTERNAL CEPHALIC VERSION The procedure is performed at or after 37 completed weeks by an experienced obstetrician. ECV should be performed with tocolytics (e.g. nifedipine) as this has been shown to improve the success rate. The woman is laid flat with a left lateral tilt having ensured that she has emptied her bladder and is comfortable. HOW IS IT DONE? With ultrasound guidance the breech is elevated from the pelvis and one hand is used to manipulate this upward in the direction of a forward role, while the other hand applies gentle pressure to flex the fetal head and bring it down to the maternal pelvis.
- 13. MANAGEMENT
- 14. RISK OF ECV Placental abruption Premature rupture of membrane (PROM) Cord accident Transplacental hemorrhage Fetal bradycardia
- 15. CONTRAINDICATIONS Fetal abnormality (e.g. hydrocephalus) Placenta praevia Oligohydramnios or polyhydramnios History of antepartum haemorrhage Previous Caesarean or myomectomy scar on the uterus Multiple gestation Pre-eclampsia or hypertension Plan to deliver by Caesarean section anyway
- 16. Pros and cons ADVANTAGES DISADVANTAGES Reduction in breech presentation in term pregnancies Reduction in Caesarian or Vaginal Breech Delivery (lower the risk of going to LSCS). If fails, about 3% will turn to spontaneous delivery Placental Abruption Umbilical Cord Entanglement Premature Rupture of Membrane Severe maternal discomfort Fetal bradycardia and non-reactive CTG Alteration in umbilical artery and mid cerebral artery waveform Increase in Amniotic Fluid Volume
- 19. INDICATIONS Presentation should be either extended or flexed No evidence of feto pelvic disproportion Estimated fetal weight < 3.5 kg No evidence of hyperextension of fetal head and fetal abnormalities (hydrocephalus) No other obstetric complications.
- 20. MANAGEMENT DURING LABOUR Fetal well being and progress of labour should be monitored Epidural administration can prevent pushing before full dilatation Fetal blood sampling to monitor acid base status Operator experienced in delivering breech babies should be available.
- 21. TECHNIQUE Descent of the buttocks occurs until the anterior buttock touches the pelvic floor. ( naturally ) Internal rotation of the anterior buttock occurs through 1/8th of a circle placing it behind the symphysis pubis. Further descent with lateral flexion of the trunk occurs until the anterior hip hinges under the symphysis pubis which is released first followed by the posterior hip. Legs are flexed (deliver spontaneously) Legs are extended, (deliver using pinard’s manoeuvre) Using a fingers to flex the leg at the knee and then extend the hip With contractions and maternal effort, lower body will delivered 1. Delivery of the buttocks 2. Delivery of the legs and lower body
- 22. TECHNIQUE
- 23. TECHNIQUE 3. Delivery of SHOULDERS Baby will be lying the shoulders in the transverse diameter of the pelvic mid cavity Descent occurs with internal rotation of the shoulders bringing the shoulders to lie in the antero-posterior diameter of the pelvic outlet. Finger will gently above the shoulder Posterior arm/ shoulder reaches the pelvic floor, it will rotate anteriorly Once the spine become visible, delivery of the second arm will follow Loveset’s manoeuvre .
- 24. TECHNIQUE
- 25. TECHNIQUE 4. Delivery of THE HEAD Delivered using the Mauriceau- smellie-veit Manoeuvre Lies between obstetrician arm with downward traction being levelled on the head via finger in the mouth and one on each maxilla If difficult, forceps need to be applied
- 26. TECHNIQUE
- 27. COMPLICATIO NS The greatest fear with a vaginal breech is that the baby will get ‘stuck’. Interference in the natural process by the inappropriate use of oxytoxic agents or by trying to pull the baby out (breech extraction) will (paradoxically) increase the obstruction occuring. When delay occurs, particularly with delivery of the shoulders or head, the presence of an experienced obstetrician will reduce the risk of death or serious injury.
- 29. Hannah ME, Hofmeyr GJ Trial Studies had proven that a patient with Breech presentation should go for C-Sect “Planned C-sect is safe for singleton term breech babies than planned vaginal birth, managed accordingly to a clinical protocol, but more complications for mothers.” The review of the this study showed that Planned C-sect was safer for the singleton breech baby at term than planned VBD.
- 30. INDICATIONS Clinically inadequate pelvis Footling or kneeling breech presentation Large baby (usually defined as larger than 3800 g) Growth-restricted baby (usually defined as smaller than 2000 g) Hyperextended fetal neck in labour Previous caesarean section. Delay in the descent of the breech at any stage in the second stage of labour. Other contraindications to vaginal birth – placenta praevia, compromised fetal condition
- 31. PROCEDURE Informed consent Surgical basis – The pfannenstiel incision – The infra-umbilical incision – Uterine incision
- 32. COMPLICATIO NS Bowel damage Caesarean hysterectomy Haemorrhage Placenta previa Urinary tract damage Infection Pulmonary emboli /DVT INTRAOPERATIVE POST-OPERATIVE
- 33. REFERENCES Obstetrics Ten Teachers 19th Edition by Philip N Baker and Louise C Kenny http://www.rcog.org.uk/globalassets/docume nts/patients/patient-information- leaflets/pregnancy/a-breech-baby-at-the-end- of-pregnancy.pdf