Case record...Thalamic glioma
•
2 gefällt mir•1,315 views

Case record...Thalamic glioma http://yassermetwally.com http://yassermetwally.net

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Case record...Thalamic glioma
Ähnlich wie Case record...Thalamic glioma (20)
Mehr von Professor Yasser Metwally
Mehr von Professor Yasser Metwally (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Case record...Thalamic glioma
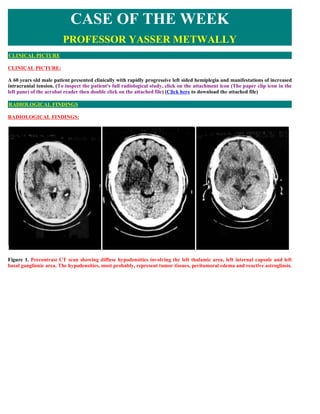
- 1. CASE OF THE WEEK PROFESSOR YASSER METWALLY CLINICAL PICTURE CLINICAL PICTURE: A 60 years old male patient presented clinically with rapidly progressive left sided hemiplegia and manifestations of increased intracranial tension. (To inspect the patient's full radiological study, click on the attachment icon (The paper clip icon in the left pane) of the acrobat reader then double click on the attached file) (Click here to download the attached file) RADIOLOGICAL FINDINGS RADIOLOGICAL FINDINGS: Figure 1. Precontrast CT scan showing diffuse hypodensities involving the left thalamic area, left internal capsule and left basal ganglionic area. The hypodensities, most probably, represent tumor tissues, peritumoral edema and reactive astrogliosis.
- 2. Figure 2. Postcontrast CT scan images showing a densely enhanced space occupying lesion involving the left thalamic area with positive mass effect and peritumoral edema involving the white matter and sparing the gray matter (vasogenic edema). Notice the peritumoral satellitosis (B) Figure 3. A postcontrast CT scan image showing peritumoral satellitosis (Figure 2 B) CT guided stereotactic biopsy revealed Mixed astrocytoma (Grade III-Grade IV diffuse astrocytoma). The patient was not operated upon, he received radiotherapy only to die 4 month following clinical diagnosis. Common pathological characteristics of diffuse astrocytomas Diffuse astrocytomas are tumors predominantly composed of astrocytes. Unless otherwise indicated, the term usually applies to diffusely infiltrating neoplasms (WHO grades II through IV). Diffuse astrocytoma is unusual in the first decade of life and most commonly presents in older children or young adults up to the age of 40 to 45. All diffuse astrocytomas, particularly the diffusely infiltrating variety, have a tendency toward progression to more malignant forms. Diffuse astrocytomas have a peculiar tendency to change its grade over time into the next higher grade of malignancy and the condition is age dependant. A change in the grade of diffuse astrocytoma is more likely to occur in the older age group.
- 3. Diffuse astrocytomas commonly start as grade II at a younger age group then gradually change its grade over time into the next higher grade until they ultimately dedifferentiate into glioblastomas (secondary glioblastoma multiforme), on the other hand, glioblastoma multiforme in older patients are usually primary-that is, they occur as glioblastoma multiforme from their inception, without progression from a lower- grade tumor. Diffuse astrocytomas appear to form a continuum of both biological and histological aggression. They vary from lesions with almost normal cytology (grade I and grade II astrocytomas) through intermediate stages (grade III, anaplastic astrocytomas) and up to the most aggressive of all human brain tumours (grade IV astrocytomas or glioblastoma multiforme). Diffuse astrocytoma often spreads widely through the brain but without destruction and also without interruption of normal function. Microscopically, tumor cells infiltrate between myelinated fibers in a nondestructive manner (perineuronal satellitosis). The local spread of diffuse astrocytomas (forming gliomatosis cerebri and butterfly gliomas) does not mean that the tumour grade is grade IV (glioblastoma multiforme), local spread can occur in grade II and grade III and in the author experience gliomatosis cerebri and butterfly gliomas are much more commonly seen in grade II astrocytomas and has not been encountered in grade III (anaplastic astrocytomas) and grade IV (glioblastoma multiforme). It takes a long time for a diffuse astrocytoma to cross the corpus callosum to the opposite hemisphere to form a butterfly glioma. Patients harbouring glioblastomas have a much shorter life span for their tumours to form butterfly gliomas, however cases were reported for glioblastomas forming butterfly tumours. These glioma cells migrate through the normal parenchyma, collect just below the pial margin (subpial spread), surround neurons and vessels (perineuronal and perivascular satellitosis), and migrate through the white matter tracks (intrafacicular spread). This invasive behavior of the individual cells may correspond to the neoplastic cell's reacquisition of primitive migratory behavior during central nervous system development. The ultimate result of this behavior is the spread of individual tumor cells diffusely over long distances and into regions of brain essential for survival of the patient. The extreme example of this behavior is a condition referred to as gliomatosis cerebri, in which the entire brain is diffusely infiltrated by neoplastic cells with minimal or no central focal area of tumor per se. Furthermore, 25% of patients with GBM have multiple or multicentric GBMs at autopsy. Although GBMs can be visualized on MRI scans as mass lesions that enhance with contrast, the neoplastic cells extend far beyond the area of enhancement. In practice considerable histological heterogeneity in astrocytic tumours is found ( i.e., low grade areas with Rosenthal fibers and calcification can be intermixed with with frankly malignant ones). The differences in histologic features, potential for invasiveness, and extent of progression likely reflect genetic differences acquired during astrocytoma growth. Grade IV astrocytomas (glioblastoma multiforme) differ from diffuse astrocytoma grade II and grade III (anaplastic astrocytomas) in the presence of gross necrosis, and microscopically in the presence of vascular endothelial hyperplasia and tumour hemorrhage. Primary tumors of the thalamus account for only 1-1.5% of all intracranial tumors and approximately 25% of them arise in children aged 15 years or under. Thalamic gliomias might be unilateral or bilateral. Diffuse and involvement of thalamic nuclei by these tumors makes surgical therapy very difficult and no case of radical removal has been described in the literature. Consequently, the main role of surgery is limited and usually performed for a histological diagnosis. Generally, these gliomas are low-grade astrocytomas (grade II of WHO classification), but limited anaplastic areas may be encountered. Radiotherapy and chemotherapy are sometimes utilized as adjuvant therapy, but their role is questionable. Outcome is generally poor, independently of the therapy that is utilized. Rapid fatal evolution after diagnosis and the almost complete unresponsiveness of these tumors to radiotherapy make these rare tumors difficult to treat. Anaplastic gliomas usually show enhancement after contrast administration. Severe dementia and personality modification observed in adults affected by bilateral thalamic glioma is attributed to the involvement of dorsomedial nuclei of thalami and their connections with temporal and frontal lobes [9]. Bilateral thalamic glial tumors are rare and less than 50 cases have been published in the literature [1-8]. DIAGNOSIS: DIAGNOSIS: THALAMIC GLIOMA
- 4. DISCUSSION DISCUSSION: Bailey and Cushing observed that gliomas become more aggressive with time, writing – all of these lesions, so far as our records permit us to judge, show an increasing degree of malignancy, the recurrent tumors giving evidence of more active cell division than the original lesion. 2 It is now understood that the accumulation of molecular abnormalities1 underlies the increasingly aggressive clinical behavior of an individual patient s glioma over time. Moreover, while GBMs may be histologically identical, they are molecularly distinct, [51] and each tumor may require individually tailored treatment with the combination of agents predicted to impact multiple molecular abnormalities. Successful therapy of a molecularly complex disease such as GBM may also require simultaneous administration of multiple agents, including both traditional chemotherapies and several pathway inhibitors. The past of glioblastoma multiforme The most common cancer arising from the brain is the glioblastoma multiforme (GBM). It is also the most deadly, [1] representing the most aggressive subtype among the gliomas, a collection of tumors including astrocytomas and oligodendrogliomas (see Table 1). In 1926, Bailey and Cushing, in describing spongioblastoma multiforme , the label then used for GBM, noted that: - It is from this group doubtless that the generally unfavorable impression regarding gliomas as a whole has been gained. It is not only the largest single group in the series but at the same time is one of the most malignant. In the five unoperated cases, the average duration of life from the onset of symptoms was only three months, which speaks well on the whole for the average survival period of twelve months for those surgically treated. [2] Since their seminal work, the median survival of 12 months has not changed markedly. Both data from the 1960s3 and current data [4] confirm that the extent of surgical resection is an important prognostic factor. However, as Bailey and Cushing observed, GBMs have – infiltrating propensities, and when enucleation is attempted, the growth is found at the depth to spread into and merge with the normal cerebral tissue without recognizable demarcation. [2] In prior eras, radical surgical excisions, including removal of the entire cerebral hemisphere containing the tumor, [5] were occasionally attempted, yet patients who survived the hemispherectomy died of recurrent tumor, [6] clinically proving the importance of the histologic observation that tumor cells invade throughout the brain. In the modern age, brain imaging may disclose macroscopic tumor in the opposite hemisphere (see Figure 1) or even gliomatosis cerebri literally a brain full of tumor. In the years leading to up to World War II, the German pathologist Scherer, whose scientific discoveries were tainted by his Nazi activities, [7] described secondary structures [8,9] that further characterized invasive tumor cells. These structures are secondary because they are dependent for their formation on underlying normal brain structures, as opposed to primary structures of the tumor such as pseudopalisading necrosis and microvascular proliferation. Examples include perineuronal and perivascular satellitosis (accumulation of tumor cells around neurons and blood vessels), subpial spread, and intrafascicular tracking such as infiltration along corpus callosum and other white matter tracks (see Figure 2). Advances in surgical technique, imaging, and targeting of radiotherapy (RT) are important contributions to local control. However, changing GBM from a disease that kills quickly to one that can be managed as a chronic illness, such as hypertension or diabetes mellitus, will require systemic therapies targeting tumor cells infiltrating throughout the brain, such as chemotherapy, immunotherapy, and small molecule pathway inhibitors. The current status of glioblastoma multiforme Currently, treatment for GBM involves both local and systemic therapy. Surgery and partial brain RT are the standard locally directed therapies. Some physicians also advise intra-operative placement of chemotherapy containing polymers (i.e. Gliadel wafers ) directly into the surgical bed in an attempt to prolong local control. [10] While there is a modest survival benefit, the use of these polymers remains controversial because of the potential for toxicity. Other treatment modalities that target disease localized to the surgical bed or the surrounding area have included brachytherapy and stereotactic radiosurgery (with either a linear accelerator or gammaknife), neither of which are commonly advised. Convection-based chemotherapies delivered by catheter infusion, such as local delivery of pseudomonas exotoxin linked to either interleukin [13] (IL-13) or transforming growth factor-a (TGFa), [11] are available in clinical trials for some patients. These trials take advantage of differences in the expression of proteins (such as growth factor receptors) on the surface of residual tumor cells in the periphery of the operative bed to deliver the toxin to tumor cells, but spare normal brain. By contrast, systemic chemotherapy targets tumor cells beyond the reach of local therapies. The most commonly prescribed systemic chemotherapy for GBM is temozolomide (Temodar®), an alkylator that became available during the last decade. The effectiveness of temozolomide in the management of GBM at diagnosis was recently demonstrated by a large multinational study.4 A modest survival benefit of 2.5 months for concurrent temozolomide with RT (14.6 months median survival) was observed relative to RT alone (12.1 months median survival).4 In addition, while the survival benefit was still
- 5. present two years after diagnosis, only 10.7% of patients were progression-free and only 26.5% of patients were alive at that point. [4] While systemic chemotherapy improves the outcome for some patients, long-term disease control therefore remains elusive. Table 1. Common Gliomas. The gliomas are assigned a grade by the World Health Organization (WHO) depending on histologic features that predict behavior.This classification scheme is derived from the clinicopathologic studies of Bailey and Cushing.2 Grade I tumors, such as juvenile pilocytic astrocytomas, are generally focal rather than diffuse and are potentially curable by surgical excision.WHO grade II–IV tumors are diffusely infiltrative.WHO grade III–IV tumors are termed ‘high grade’ or malignant. GBMs, or grade IV astrocytomas, are the most aggressive subtype. Discoveries during the last several years have improved the understanding of glioma and general cancer biology markedly. Generally, a cancer comprises cells that either divide or survive when they should instead undergo either cell cycle arrest or die. These abnormalities are also not mutually exclusive, and most cancers, including GBMs, are driven by several molecular abnormalities. The signal to divide is typically provided by a growth factor (ligand). Examples include TGF?, epidermal growth factor (EGF), platelet-derived growth factor (PDGF), and vascular endothelial growth factor (VEGF). Such ligands interact with cells through receptors including EGF receptors (EGFRs), PDGF receptors (PDGFRs), and VEGF receptors (VEGFRs). Receptor activity is linked with cellular processes such as mitosis or invasion by signal transduction cascades. Examples of signal transduction cascades important in human GBMs include those activated by the oncogenes Ras, Akt, and Src. [12] In cancer cells, these pathways are disrupted through several mechanisms. For example, EGFR is overexpressed in up to 92% of astrocytomas, [13] and up to 62% of GBMs express EGFRvIII, [14] a mutant receptor that is active independently of ligand. Co-expression of EGF and EGFR15,16 in GBMs leads to a potential autocrine loop.An analogous loop is created by PDGF and PDGFR co-expression in up to 94% of high-grade oligodendrogliomas. [17–19] Regardless of ligand or receptor status, close to 100% of GBMs exhibit activation of Ras,20,21 and approximately 70% exhibit activated Akt, [21,22] the latter typically through loss of the tumor suppressor gene phosphatase tensin homolog on chromosome ten (PTEN), [23–25] which normally represses Akt activation. Src is detected in 67% of GBMs.26 Finally, control over cell division is normally maintained by tumor suppressors, such as an inhibitor of CDK4A (INK4A) and its alternative reading frame (ARF), as well as p53, which also contributes to DNA repair and apoptosis, and other enzymes. Disruptions of normal cell cycle control of one form or another have been observed in almost all GBMs. [12,27] Figure 1. Magnetic Resonance Imaging Findings in Glioblastoma Multiforme. Contrast enhanced magnetic resonance image (MRI) of the brain demonstrating a large GBM with a smaller site in the contralateral hemisphere. This infiltrative nature of GBMs, essentially effecting the entire brain, underscores the failure of even radical surgery, such as hemispherectomy, to effect cure. Moreover, the modeling of gliomas in mice has demonstrated that abnormalities of ligands, receptors, signal transducers, and proliferation cause gliomas. For example, combined activation of Ras with Akt in glial progenitors is sufficient to induce GBMs in mice, [22] and transgenic expression of activated forms of Ras [28] or Src [29] in glia leads to GBMs following spontaneous development of cooperative oncogenic abnormalities. Modeling has also demonstrated that PTEN loss is functionally equivalent to Akt activation, [30] when combined with activated Ras. PDGF overexpression in glia causes high- grade oligodendrogliomas [31,32] that also exhibit pathologic features of GBMs, including pseudopalisading necrosis and microvascular proliferation. The threshold to tumor formation is lowered by disruption of Ink4a-Arf or p53 expression. [31,33,34] While more is learned about glioma biology, small molecule inhibitors are being developed that target the causal pathways. [35] For example, several inhibitors of EGFRs are under investigation in clinical trials. These include the EGFR inhibitors erlotinib (OSI- 774/Tarceva), gefitinib (ZD-1839/Iressa), and lapatinib (GW572016). The PDGFR inhibitors imatinib (STI- 571/Gleevec) and PTK787, both of which have other targets, are also in use. Signal transduction cascade blockers are also
- 6. being studied. One example is R11577, which targets the enzyme that activates Ras. Rapamycin (sirolimus), CCI-779 (temsirolimus), and Rad-001 (everolimus) target mTOR, one of the key enzymes activated by Akt. Figure 2. Histology of Gliomas. (A) Pseudopalisading (arrow) necrosis (arrow head) and (B) microvascular proliferation (arrow) are the classic histologic findings in glioblastoma multiforme (GBM). Secondary Scherer structures (C) involve tumor cells (arrow heads) accumulating around blood vessels (BV, long arrow), and neurons (N, long arrow) in a low grade (WHO grade II) oligodendroglioma. Such perivascular and perineuronal satellitosis, along with intrafascicular growth and subpial accumulation (not shown), contribute to the diffusely infiltrative nature of gliomas throughout normal brain structures.. (Click to enlarge figure) Unfortunately, despite initial enthusiasm, treatment of GBMs as well as systemic malignancies with these small molecule inhibitors as single agents has generally been disappointing. For example, published interim and final reports of trials involving gefitinib, [36,37] erlotinib, [38–40] imatinib, [41,42] PTK787, [43,44] and CCI-77945 monotherapy for recurrent high-grade gliomas have not shown response or survival rates that are markedly superior to those observed with traditional chemotherapies, such as temozolomide4,46–48 or carmustine (BCNU). [49] However, there are individual patients treated with these agents who experience durable objective responses or sustained stable disease.Therefore, these agents are likely to have a role in GBM management. Figure 3. Pathways Important in GBM Biology. An extracellular ligand such as EGF,TGFa, or PDGF induces dimerization of receptors such as EGFR or PDGFR. Receptor stimulation activates intrinsic tyrosine kinase (TK) activity and EGFR and PDGFR are therefore called receptor tyrosine kinases (RTKs). RTKs then activate the Akt, Src, and Ras signal transduction cascades.Tumor cell growth is driven by ligand or receptor overexpression, constitutively activating receptor mutations (e.g. EGFRvIII), or signal transduction activity. Pointed (green) and block (red) arrows indicate pathway activation and inhibition, respectively.The inhibitors shown and others are under investigation in the treatment of GBMs. Future perceptive of glioblastoma multiforme In addition to surgical resection and RT, the future of GBM therapy is likely to involve both additional measures to improve local control (such as convection or catheter delivery of antitumor agents into the operative cavity) and systemic treatment to address infiltrative disease distant from the main tumor bed. However, a major thrust of research will be tissue analyses looking for molecular features that predict sensitivity of GBMs to either traditional chemotherapies or small molecule inhibitors. Tailoring therapy with specific drugs to those patients is most likely to improve response rates and spare patients who are unlikely to benefit the expense and potential toxicity of these agents. Determination of a molecularly effective dose (MED) (inhibits a pathway), may also be more useful than the traditionally used maximally tolerated dose (MTD). An example of a molecular prognostic factor is loss of heterozygosity for chromosomes 1p and 19q in anaplastic oligodendrogliomas, which predicts both sensitivity to chemotherapy and radiation, as well as longer overall survival. [50] Consequently, some neurooncologists are currently using results of 1p/19q analysis to guide therapy, [51] although this remains an area of controversy. Other genomic alterations are also predictive—PTEN loss is associated with poor survival for patients with anaplastic oligodendrogliomas [52] and is likely to predict poor outcome from GBM. [23,53,54] More recently it was reported that GBMs, in which O6-methylguanine- DNA methyltransferase (MGMT) expression was silenced by gene methylation, were more sensitive to temozolomide than tumors with unmethylated MGMT. The likely explanation is that MGMT may counteract temozolomide activity by removing alkyl groups on DNA. [55] It is unclear whether MGMT
- 7. methylation impacts sensitivity of other glioma subtypes to temozolomide, yet MGMT methylation status may be used in the near future to guide therapy. Individualized medicine determined by molecular rather than simply histologic phenotype may also guide therapy with small molecule inhibitors. Somatic mutations in exons 18 21 of EGFR are associated with sensitivity of lung cancer to gefitinib [56 58] or erlotinib. [58] However, the authors and others have not found these mutations in gliomas. [34,57,59,60] Efforts are under way to identify the molecular features that predict sensitivity of GBMs to EGFR and other receptor tyrosine kinase (RTK) inhibitors. Response and survival rates may also be improved through combination therapy. For example, preliminary data suggest that concurrent therapy with imatinib (PDGFR/VEGFR inhibitor) and hydroxyurea (a more traditional chemotherapy) is more effective than imatinib monotherapy. A small series with 14 evaluable patients with recurrent GBMs demonstrated a disease control rate (complete response or partial response or stable disease) of 64% for patients treated with this combination. [61] By contrast, imatinib monotherapy led to a disease control rate of 29%. [42] Larger trials of this and other combinations, such as temozolomide with PTK787, are under way. (Click here to download master degree thesis " Non surgical management of brain tumors" in PDF format) SUMMARY SUMMARY The last five years have seen an evolution in the management of highgrade astrocytic tumors comparable in scope yet greater in magnitude to that of the prior 40 years. This is thanks to the convergence of three factors: the introduction of an oral agent with antitumor activity beyond the blood–brain barrier and modest systemic toxicity (temozolomide); the demonstration through a well-conducted randomized trial of the superiority of multimodality therapy; and the fact that we now stand on the threshold of additional progress through key advances in translational biology, which, in many cancers, is providing new targets for therapeutic intervention. Astrocytic tumors have long been the bane of neurosurgeons, radiation therapists, and neuro-oncologists. Although they account for only 2.3% of all cancer-related deaths in the US, [63] little if any substantial progress in brain imaging and treatment had been made until the first years of this millennium. Characteristics of high-grade glial tumors compared with other cancers are its unique location, robust invasive and angiogenic capabilities without a significant propensity to metastasize outside of the central nervous system (CNS), and the profound histological and molecular heterogeneity within tumor specimens. Advances in the Management of Glioblastomas— Multimodality Strategies In 2003, a phase III study in 240 newly diagnosed patients with surgically resectable malignant gliomas—including 207 with glioblastoma multiforme (GBM)—compared surgery plus radiotherapy and placebo wafers with surgery plus radiotherapy and the addition of 3.8% bischloroethyl nitrosourea (BCNU, carmustine) wafers (Gliadel wafers) into the tumor bed. The study demonstrated a modest, albeit significant, prolongation of survival in the latter group (13.9 versus 11.6 months). [64] Long-term follow-up of this study showed that the survival advantage with BCNU wafers was maintained at one, two, and three years, and was statistically significant (p=0.01) at three years compared with placebo, although the absolute number of patients evaluated at this latter timepoint was quite small. [65] Perhaps the most significant advance in the management of glioblastomas emanates from the work of Stupp et al. [65] who, in a safety and efficacy study, randomized 573 patients with newly diagnosed glioblastoma from 85 centers, primarily in Europe, to radiotherapy alone or to radiotherapy plus concomitant temozolomide followed by monthly temozolomide for six cycles. At a median follow-up of 28 months the median survival in the radiotherapy group alone was 12.1 months compared with 14.6 months in the group receiving both treatment modalities (p<0.001). The two-year survival rate was 10.4% with radiotherapy alone versus 26.5% with radiotherapy and temozolomide. The results of this study produced level 1A evidence for the benefit of this combined modality treatment in initially diagnosed patients, and was incorporated into the new National Comprehensive Cancer Network (NCCN) guidelines for CNS tumors in 2005. Thus, as a next logical step, a fusion of these two prior studies was evaluated in a phase II setting in patients with newly
- 8. diagnosed, highgrade GBM undergoing resection with BCNU wafer insertion followed by the combination of radiotherapy plus temozolomide. Early interim data have been presented in abstract form. [67] The study end-points include survival and progression-free survival (PFS). Of 35 patients enrolled so far, 34 were diagnosed with GBM. At median follow-up of 10.4 months, [87] patients had documented recurrence and 19 patients had died. Six patients remain on active treatment. The one- year survival rate is 64%, and median survival is 18.6 months. These early data suggest that combination therapy with BCNU wafers followed by therapy plus temozolomide may be an effective regimen in patients with initial highgrade resectable malignant gliomas, although randomized trials will ultimately be needed to assess the efficacy of this treatment modality. Other treatment modalities that have been investigated for the treatment of high-grade astrocytic tumors—especially in terms of targeting disease localized to the surgical bed or the surrounding area—have included stereotactic radiosurgery and brachytherapy. A randomized trial conducted by the Radiation Therapy Oncology Group (RTOG) compared post-operative conventional radiotherapy plus systemic BCNU alone or preceded by stereotactic radiosurgery—including both linear accelerator or gamma-knife—in patients with GBM (>4cm tumor size). The results of the trial were disappointing with no improvement in local control or survival with stereotactic radiosurgery. [68] The US Food and Drug Administration (FDA) has recently approved GliaSite, a novel brachytherapy device, to provide local post-operative irradiation to high- grade gliomas. However, to date, no efficacy trials have been conducted with the system. In a retrospective, multiinstitutional analysis, median survival— measured from the date of GliaSite placement—was 35.9 weeks for patients with an initial diagnosis of GBM. The patient population consisted of patients with recurrent high-grade gliomas who had previously undergone resection and had received external beam radiotherapy as part of their initial treatment. Following surgical debulking of the recurrent lesion, an expandable balloon catheter (GliaSite) was placed in the tumor cavity. Although reirradiation of malignant gliomas with the GliaSite system appeared to provide a modest survival benefit, it is difficult to assess the value of any survival without the benefit of a control group. [69] Convection-enhanced delivery (CED) of toxins to the tumor site is a new treatment modality under investigation for malignant gliomas. It was developed as a method to treat brain tumors by circumventing the normal limitations imposed by the blood– brain barrier. CED involves the stereotactically guided implantation of delivery catheters directly into the residual tumor or around the resection cavity to facilitate the local delivery by high-flow micro-infusion of the targeted toxin to tumor cells. A combined summary of three phase I clinical trials investigating the use of cintredekin besudotox—a recombinant protein consisting of interleukin-13 (IL-13) and a truncated form of Pseudomonas exotoxin— delivered via CED in the treatment of recurrent malignant glioma following tumor resection, demonstrated an overall median survival after treatment of 45.9 weeks. [70] The Phase III Randomized Evaluation of Convection Enhanced Delivery of IL13-Pe38qqr with Survival Endpoint (PRECISE) Trial was designed to compare CED of cintredekin besudotox to treatment with the BCNU wafers in 294 patients with first recurrence or progression of GBM. Unfortunately, the study was stopped in December 2006 after the efficacy end- point of a statistically significant difference in overall survival was not met. Indeed, the median survival in the CED arm was 36.4 weeks, while that of the BCNU wafer arm was 35.3 weeks. An NCI-sponsored phase I trial is currently evaluating CED of 131I-chTNT-1/B, a chimeric tumor necrosis therapy antibody attached to the radioisotope iodine 131 in malignant glioma. Although CED is a promising alternative for targeted delivery, it remains a complex, interdisciplinary technique that needs further investigation to optimize catheter positioning and drug distribution. Molecular Targets and Prognostic Factors Turning to recent advances in the genomic analysis of glioblastoma, four molecular markers are currently being explored. First is the identification of loss of the chromosome 1p/19q in anaplastic oligodendroglioma as a predictor of response to chemotherapy—particularly PCV (procarbazine, CCNU [chloroethylnitrosourea, lomustine], and vincristine). The initial results, published by Cairncross et al. in 1998, [9] led to two randomized clinical trials. The first—European Organization for Research and Treatment of Cancer (EORTC) 26951—evaluated radiotherapy versus radiotherapy followed by PCV in patients with newly diagnosed anaplastic oligodendroglioma or anaplastic oligo-astrocytomas. [10] The second (RTOG 94-02) evaluated PCV given prior to radiotherapy. [73] Both studies demonstrated that the addition of PCV improved PFS without impacting on overall survival (OS). Although chromosome-1p/19q loss does predict chemosensitivity, it did not identify patients who have a better outcome after adjuvant chemotherapy. Moreover, it became apparent that patients with the combined chromosomal 1p/19q loss have a better outcome after radiotherapy compared with patients whose tumor does not contain this chromosomal aberration. At a molecular level, up to 50% of glioblastoma specimens express dysregulated epidermal growth factor receptor (HER1/EGFR). [74] This observation has spurred interest in the use of the small molecule HER1/EGFR-targeted therapy agents such as erlotinib and gefitinib. Initial phase II studies evaluating gefitinib failed to demonstrate significant objective tumor regressions, with a six-month PFS of only 13% in 53 patients with recurrent glioblastoma. [75] In contrast, the data relating to erlotinib initially appeared somewhat more promising in one study of 31 patients with recurrent glioblastomas, in which six patients achieved a partial response and the six-month PFS was 26%. [76,77] Of note is that these authors could not determine any correlation between response and EGFR expression or amplification within the tumor specimens. Also, a second phase II study of 30 patients treated with erlotinib failed to result in any objective responses or six-month PFS. [78] Unfortunately, a recent EORTC trial comparing erlotinib with either temozolomide or BCNU in 110 patients with recurrent glioblastoma failed to demonstrate a benefit of the oral targeted therapy with respect to sixmonth PFS or 12-month survival. [79] Optimal dosing of these oral agents, especially while patients are taking enzyme-inducing anti-
- 9. epileptics or drugs with similar pharmacological effects, may be a significant confounding variable in determining their true clinical efficacy. [80] Another molecular target of some promise in the management of patients with GBM is transforming growth factor beta (TGF-B). Not only does it stimulate cell migration, invasion, and angiogenesis, but it also appears to play an important role in the disruption of afferent and efferent immune responses. [81] Several in vitro systems, as well as rodent glioma models, delineate the potential therapeutic impact of TGF-B antagonism, employing not only antisense strategies, but also specific TGF-B receptor kinase antagonists. In particular, the use of such agents in conjunction with vaccines, or perhaps novel approaches of cellular immunotherapy, bears further study. Another molecular marker of interest is the O6-methylguanine- DNA methyltransferase (MGMT) promoter gene, also known as O6-alkylguanine-DNA alkyltransferase or AGT. The gene itself expresses alkyltransferase, which plays a role in resistance to alkylating and methylating agents. Methylation of this gene disrupts the expression of alkyltransferase and thus renders the cell more susceptible to alkylating and methylating chemotherapy agents such as temozolomide. Hegi et al. analyzed tissue from newly diagnosed patients with glioblastoma enrolled into the EORTC 26981 trial, and documented a significant correlation between MGMT methylation and outcome from treatment. [82] Methylation of the MGMT promoter was demonstrated in 45% of 206 tumors analyzed, and this was associated with a 46% survival rate at two years compared with only 13.8% in those patients with non-methylated promoter status. [82] Although the preliminary conclusion from this translational study is that MGMT promoter methylation may be predictive of outcome to multimodality treatment in glioblastoma, validation from additional prospective studies is required. A novel oral protein kinase C inhibitor that initially appeared to have activity in recurrent glioblastoma was enzastaurin. This agent, an oral inhibitor of PKCß and PI3K/AKT pathways, is well tolerated, possesses antiangiogenic properties in pre- clinical models, and induces tumor cell apoptosis. [83] Enzastaurin is currently being evaluated in phase II trials for the treatment of patients with recurrent high-grade gliomas. Initial results in 87 evaluable patients with recurrent high-grade gliomas showed that enzastaurin treatment was well tolerated and objective radiographic responses were seen in 22% of patients with GBM. The exposure to enzastaurin was significantly lower in patients treated with enzyme-inducing antiepileptic drugs (EIADs). [84] Enzastaurin also appears to be safe in conjunction with radiation therapy and temozolomide in patients with newly diagnosed GBM. [85] GBM is highly angiogenic, and vascular endothelial growth factor (VEGF) is amplified in most GBM tumors. [86] Over the last three years, there has also been an evolution in the understanding of the ‘brain tumor stem cell.’ If the concept of a brain tumor stem cell proves to be a real entity, identifiable perhaps by CD-133 expression, and correlated with a significant angiogenic effect associated with VEGF expression and production, this could confirm an important role for antiangiogenic therapy in this cancer. [87] This prompted the evaluation of the recombinant humanized anti-VEGF monoclonal antibody bevacizumab in patients with malignant gliomas. A recent phase II trial studied the effect of bevacizumab in combination with the cytotoxic agent irinotecan in patients with recurrent high-grade astrocytic neoplasms. [26] The investigators demonstrated a radiographic response rate of 63% with the combination therapy and six- month overall survival was estimated at 72%. A randomized phase II study in patients with recurrent glioblastomas evaluating bevacizumab alone versus bevacizumab with irinotecan was recently completed and the results are anxiously awaited . Additional agents with antiangiogenic properties such as the multitargeted agents sorafenib and sunitinib are also being investigated in malignant gliomas. [89,90,91] Conclusion Significant advances are being made in the understanding of the biology of high-grade gliomas, which are contributing to the development of promising targeted therapies and treatment modalities. Over the last couple of years, there has been an evolution in the understanding of the ‘brain tumor stem cell.’ If the concept of a brain tumor stem cell proves to be a real entity identifiable by CD-133 expression, and if this correlates with a significant angiogenic effect associated with VEGF expression and production, it opens new possibilities for targeted therapy. [89] Multitargeted therapy is a necessity to manage high-grade brain tumors optimally. The potential of quadruple multimodality therapy for the management of brain tumors, which includes surgery, radiotherapy, systemic therapy, and localized chemotherapy, needs to be further investigated. Furthermore, with the promising results seen with bevacizumab, there is the possibility of a fifth modality—an antiangiogenesis inhibitor. Addendum A new version of this PDF file (with a new case) is uploaded in my web site every week (every Saturday and remains available till Friday.) To download the current version follow the link "http://pdf.yassermetwally.com/case.pdf". You can also download the current version from my web site at "http://yassermetwally.com". To download the software version of the publication (crow.exe) follow the link: http://neurology.yassermetwally.com/crow.zip The case is also presented as a short case in PDF format, to download the short case follow the link: http://pdf.yassermetwally.com/short.pdf
- 10. At the end of each year, all the publications are compiled on a single CD-ROM, please contact the author to know more details. Screen resolution is better set at 1024*768 pixel screen area for optimum display. Also to view a list of the previously published case records follow the following link (http://wordpress.com/tag/case- record/) or click on it if it appears as a link in your PDF reader To inspect the patient's full radiological study, click on the attachment icon (The paper clip icon in the left pane) of the acrobat reader then double click on the attached file. Click here to download the short case version of this case record in PDF format REFERENCES References 1. Kleihues P, Cavanee W K, Pathology and Genetics of Tumours of the Nervous System, International Agency for Research on Cancer (IARC) Press, Lyon:WHO/IARC (2000). 2.Bailey P, Cushing H, A classification of the tumors of the glioma group on a histo-genetic basis with a correlated study of prognosis, Philadelphia: J B Lippincott Co. (1926). 3.Jelsma R K, Bucy P C, “The treatment of glioblastoma multiforme”, Trans.Am. Neurol. Assoc. (1967);92: pp. 90-93. 4.Stupp R et al., “Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma”, N. Engl. J. Med. (2005);352(10): pp. 987-996. 5.Dandy W E,”Removal of right cerebral hemisphere for certain tumors with hemiplegia”, JAMA (1928);90: pp. 823-825. 6.Gardner W J et al., “Residual functioning following hemispherectomy for tumouir and for infantile hemiplegia”, Brain (1955);78(4): pp. 487-502. 7.Peiffer J, Kleihues P,”Hans-Joachim Scherer (1906-1945), Pioneer in Glioma Research, Brain Pathol. (1999);9(2): pp. 241- 245. 8.Scherer H J, “Structural development in gliomas”, Am. J. Cancer (1938);34(3): pp. 333-351. 9.Scherer H J, “The forms of growth in gliomas and their practical significance”, Brain (1940);63(part 1): pp. 1-35. 10.Kleinberg L R et al., “Clinical course and pathologic findings after Gliadel and radiotherapy for newly diagnosed malignant gliama: implications for patient management”, Cancer Invest. (2004);22(1): pp. 1-9. 11.Sampson J H et al.,”Sustained radiographic and clinical response in patient with bifrontal recurrent glioblastoma multiforme with intracerebral infusion of the recombinant targeted toxin TP-38: case study”, Neuro-oncol. (2005);7(1): pp. 90-96. 12.Lassman A B, Holland E C, “Molecular Biology and Genetic Models of Gliomas and Medulloblastomas”, in Russell and Rubinstein s Pathology of Tumors of the Nervous System 7th Edition, McLendon et al. (eds) (2005), Arnold Health Sciences: London (in press). 13.Schlegel J et al.,”Amplification and differential expression of members of the erbB-gene family in human glioblastoma”, J. Neurooncol. (1994);22(3): pp. 201-207. 14.Wikstrand C J et al., “Monoclonal antibodies against EGFRvIII are tumor specific and react with breast and lung carcinomas and malignant gliomas”, Cancer Res. (1995);55(14): pp. 3,140-3,148. 15.Mishima K et al., “Heparin-binding epidermal growth factor-like growth factor stimulates mitogenic signaling and is highly expressed in human malignant gliomas”, Acta. Neuropathol. (Berl) (1998);96: pp. 322-328. 16.Ekstrand A J et al.,”Genes for epidermal growth factor receptor, transforming growth factor and their expression in human gliomas in vivo”, Cancer Res. (1991);51(8): pp. 2,164-2,172. 17.Di Rocco F et al., “Platelet-derived growth factor and its receptor expression in human oligodendrogliomas”, Neurosurgery (1998);42(2): pp. 341-346.
- 11. 18.Robinson S et al., “Constitutive Expression of Growth-related Oncogene and Its Receptor in Oligodendrogliomas”, Neurosurgery (2001);48(4): pp. 864-873; discussion pp. 873-874. 19.Shoshan Y et al., “Expression of oligodendrocyte progenitor cell antigens by gliomas: implications for the histogenesis of brain tumors”, Proc. Natl. Acad. Sci. USA (1999);96(18): pp. 10,361-10,366. 20.Guha et al., “Proliferation of human malignant astrocytomas is dependent on Ras activation”, Oncogene (1997);15(23): pp. 2,755-2,765. 21.Rajasekhar V K et al., “Oncogenic Ras and Akt signaling contribute to glioblastoma formation by differential recruitment of existing mRNAs to polysomes”, Mol. Cell. (2003);12(4): pp. 889-901. 22.22. Holland E C et al., Combined activation of Ras and Akt in neural progenitors induces glioblastoma formation in mice”, Nat. Genet. (2000);25(1): pp. 55-57. 23.Sano T et al., “Differential Expression of MMAC/PTEN in Glioblastoma Multiforme: relationship to localization and prognosis”, Cancer Res. (1999);59(8): pp. 1,820-1,824. 24.Choe G et al.,”Analysis of the phosphatidylinositol 3 -kinase signaling pathway in glioblastoma patients in vivo”, Cancer Res. (2003);63(11): pp. 2,742-2,746. 25.Ermoian R P et al., “Dysregulation of PTEN and protein kinase B is associated with glioma histology and patient survival”, Clin. Cancer Res. (2002);8(5): pp. 1,100-1,106. 26.Takenaka N et al.,”Immunohistochemical detection of the gene product of Rous sarcoma virus in human brain tumors”, Brain Res. (1985);337(2): pp. 201-207. 27.Fulci G et al.,”p53 gene mutation and ink4a-p14 deletion appear to be two mutually exclusive events in human glioblastoma”, Oncogene (2000);19(33): pp. 3,816-3,822. 28.Ding H et al.,”Astrocyte-specific expression of activated p21-ras results in malignant astrocytoma formation in a transgenic mouse model of human gliomas”, Cancer Res. (2001);61(9): pp. 3,826-3,836. 29.Weissenberger J et al., “Development and malignant progression of astrocytomas in GFAF-v-src transgenic mice”, Oncogene (1997);14(17): pp. 2,005-2,013. 30.Hu X et al.,”PTEN loss is equivalent to Akt and cooperates with Ras in the formation of GBMs”, Neoplasia (2005); in press. 31.Dai C et al., “PDGF autocrine stimulation dedifferentiates cultured astrocytes and induces oligodendrogliomas and oligoastrocytomas from neural progenitors and astrocytes in vivo”, Genes Dev. (2001);15(15): pp. 1,913-1,925. 32.Shih A H et al., “Dose-dependent effects of platelet-derived growth factor-B on glial tumorigenesis”, Cancer Res. (2004);64 (14): pp. 4,783-4,789. 33.Uhrbom L et al., “Ink4a-Arf loss cooperates with KRas activation in astrocytes and neural progenitors to generate glioblastomas of various morphologies depending on activated Akt”, Cancer Res. (2002);62(19): pp. 5,551-5,558. 34.Holland laboratory, unpublished results. 35.Mischel P S, Cloughesy T F,”Targeted molecular therapy of GBM”, Brain Pathol. (2003);13(1): pp. 52-61. 36.Lieberman F S et al.,”Phase I-II study of ZD-1839 for recurrent malignant gliomas and meningiomas progressing after radiation therapy”, J. Clin. Oncol. (2003);22: p. 105 (abstract 421). 37.Rich J N et al., “Phase II Trial of Gefitinib in Recurrent Glioblastoma”, J. Clin. Oncol. (2004);22(1): pp. 133-142. 38.Vogelbaum M A et al., “Phase II trial of the EGFR tyrosine kinase inhibitor erlotinib for single agent therapy of recurrent Glioblastoma Multiforme: Interim results”, J. Clin. Oncol. (2004);22(14S): p. 1,558 (abstract). 39.Raizer J J et al., “A phase II trial of erlotinib (OSI-774) in patients (pts) with recurrent malignant gliomas (MG) not on EIAEDs.”, J. Clin. Oncol. (2004);22(14S): p. 1,502 (abstract). 40.Yung A et al., “Erlotinib HCL for glioblastoma multiforme in first relapse, a phase II trial”, J. Clin. Oncol. (2004);22(14S):
- 12. p. 1,555 (abstract). 41.van den Bent M et al., “Multicentre phase II study of imatinib mesylkate (Gleevec) in patients with recurrent glioblastoma”, Neuro-oncol. (2004);6(4): p. 383 (abstract). 42.Wen P Y et al., “Phase I/II study of imatinib mesylate (STI571) for patients with recurrent malignant gliomas (NABTC 99- 08)”, Neuro-oncol. (2004);6(4): p. 385 (abstract). 43.Yung W K A et al., “A phase I trial of PTK787/ZK 222584 (PTK/ZK), a novel oral VEGFR TK inhibitor in recurrent glioblastoma”, Proc.Am. Soc. Clin. Oncol. (2004), abstract no. 315. 44.Conrad C et al.,”A phase I/II trial of single-agent PTK 787/ZK222584 (PTK/ZK), a novel, oral angiogenesis inhibitor, in patients with recurrent glioblastoma multiforme (GBM)”, J. Clin. Oncol. (2004);22(14S): p. 1,512 (abstract). 45.Chang S et al.,”Phase II/pharmacokinetic study of CCI-779 in recurrent GBM”, Neuro-oncol. (2003);5(4): p. 349 (abstract). 46.Yung W K et al., “A phase II study of temozolomide vs. procarbazine in patients with glioblastoma multiforme at first relapse”, Br. J. Cancer (2000);83(5): p. 588-593. 47.Brada M, Hoang-Xuan K, Rampling R, “Multicenter phase II trial of temozolomide in patients with GBM at first relapse”, Ann. Oncol. (2001);12(2): pp. 259-266. 48.Chang S M,Theodosopoulos P, Lamborn K, Malec M, Rabbitt J, Page M et al., “Temozolomide in the treatment of recurrent malignant glioma”, Cancer (2004);100(3): p. 605-611. 49.Brandes A A,Tosoni A, Amista P, Nicolardi L et al., “How effective is BCNU in recurrent glioblastoma in the modern era? A phase II trial”, Neurology (2004);63(7): pp. 1,281-1,284. 50.Cairncross J G, Ueki K, Zlatescu M C et al., “Specific genetic predictors of chemotherapeutic response and survival in patients with anaplastic oligodendrogliomas”, J. Natl. Cancer Inst. (1998);90(19): p. 1,473-1,479. 51.Louis D N, Holland E C, Cairncross J G et al.,”Glioma classification: a molecular reappraisal”, Am. J. Pathol. (2001);159 (3): pp. 779-786. 52.Sasaki H et al.,”PTEN is a target of chromosome 10q loss in anaplastic oligodendrogliomas and PTEN alterations are associated with poor prognosis”, Am. J. Pathol. (2001);159(1): p. 359-367. 53.Zhou Y H et al., “The expression of PAX6, PTEN, vascular endothelial growth factor, and epidermal growth factor receptor in gliomas: relationship to tumor grade and survival”, Clin. Cancer Res. (2003);9(9): pp. 3,369-3,375. 54.Hill C, Hunter S B, Brat D J,”Genetic markers in glioblastoma: prognostic significance and future therapeutic implications”, Adv. Anat. Pathol. (2003);10(4): pp. 212-217. 55.Hegi M E, Diserens A C, Gorlia T et al.,”MGMT gene silencing and benefit from temozolomide in glioblastoma”, N. Engl. J. Med. (2005);352(10): p. 997-1,003. 56.Paez J G et al., “EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy”, Science (2004);304(5676): pp. 1,497-1,500. 57.Lynch T J, Bell D W, Sordella R et al.,”Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib”, N. Engl. J. Med. (2004);350(21): p. 2,129-2,139. 58.Pao W, Miller V, Zakowski M et al., “EGF receptor gene mutations are common in lung cancers from never smokers and are associated with sensitivity of tumors to gefitinib and erlotinib”, Proc. Natl.Acad. Sci.USA (2004);101(36): p. 13,306-13,311. 59.Barber T D et al.,”Somatic mutations of EGFR in colorectal cancers and glioblastomas”,N.Engl. J.Med. (2004);351(27): p. 2,883. 60.Rich J N, Rasheed B K,Yan H et al., “EGFR mutations and sensitivity to gefitinib”, N. Engl. J. Med. (16 September 2004);351(12): p. 1,260. 61.Dresemann G, “Imatinib (STI571) plus hydroxyurea: Safety and efficacy in pre-treated, progressive glioblastoma
- 13. multiforme (GBM) patients (pts)”, J. Clin. Oncol. (2004);22(14S): p. 1,550 62. Metwally, MYM: Textbook of neuroimaging, A CD-ROM publication, (Metwally, MYM editor) WEB-CD agency for electronic publication, version 11.2a. April 2010 63.American Cancer Society, Cancer Facts and Figures 2006, Atlanta, American Cancer Society, 2006. Available at: http://www.cancer.org/downloads/STT/CAFF2006PWSecured.pdf 64.Westphal M, Ram Z, Riddle V, et al., on behalf of the Executive Committee of the Gliadel Study Group, Gliadel wafer in initial surgery for malignant glioma: long-term follow-up of a multicenter controlled trial, Acta Neurochir (Wien), 2006;148:269–75. 65.Stupp R, Mason WP, van den Bent MJ, et al., Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma, N Engl J Med, 2005;352:987–96. 66.Westphal M, Hilt DC, Bortey E, et al., A phase III trial of local chemotherapy with biodegradable carmustine (BCNU) wafers (Gliadel wafers) in patients with primary malignant glioma, Neuro-oncol, 2003;5:79–88. 67.LaRocca RV, Hodes J, Villaneuva WG, et al., A phase II study of radiation with concomitant and then sequential temozolomide (TMZ) in patients (pts) with newly diagnosed supratentorial high grade malignant glioma (MG) who have undergone surgery with carmustine (BCNU) wafer insertion, Annual Meeting of the Society of Neuro-Oncology, Neuro-Oncol, 2006;8:445, Abstract TA-28. 68.Souhami L, Seiferheld W, Brachman D, et al., Randomized comparison of stereotactic radiosurgery followed by conventional radiotherapy with carmustine to conventional radiotherapy with carmustine for patients with glioblastoma multiforme: report of Radiation Therapy Oncology Group 93-05 protocol, Int J Radiat Oncol Biol Phys, 2004;60:853–60. 69.Gabayan AJ, Green SB, Sanan A, et al., GliaSite brachytherapy for treatment of recurrent malignant gliomas: a retrospective multiinstitutional analysis, Neurosurgery, 2006;58(4):701–9. 70.Kunwar S, Prados MD, Chang SM, et al., Direct intracerebral delivery of cintredekin besudotox (IL13-PE38QQR) in recurrent malignant glioma: a report by the Cintredekin Besudotox Intraparenchymal Study Group, J Clin Oncol, 2007;25 (7):837–44. 71.Cairncross JG, Ueki K, Zlatescu MC, et al., Specific genetic predictors of chemotherapeutic response and survival in patients with anaplastic oligodendrogliomas, J Natl Cancer Inst, 1998;90:1473–9. 72.van den Bent MJ, Carpentier AF, Brandes AA, et al., Adjuvant procarbazine, lomustine, and vincristine improves progressionfree survival but not overall survival in newly diagnosed anaplastic oligodendrogliomas and oligoastrocytomas: a randomized European Organisation for Research and Treatment of Cancer phase III trial, J Clin Oncol, 2006;24:2715–22. 73. Intergroup Radiation Therapy Oncology Group Trial 9402, Cairncross G, Berkey B, Shaw E, et al., Phase III trial of chemotherapy plus radiotherapy compared with radiotherapy alone for pure and mixed anaplastic oligodendroglioma: Intergroup Radiation Therapy Oncology Group Trial 9402, J Clin Oncol, 2006;24:2707–14. 74.Halatsch ME, Schmidt U, Behnke-Mursch J, et al., Epidermal growth factor receptor inhibition for the treatment of glioblastoma multiforme and other malignant brain tumors, Cancer Treat Rev, 2006;32:72–89. 75.Rich JN, Reardon DA, Peery T, et al., Phase II trial of gefitinib in recureent glioblastoma, J Clin Oncol, 2004;22:133–42. 76.Vogelbaum MA, Peereboom D, Stevens G, et al., Response rate to single agent therapy with the EGFR tyrosine kinase inhibitor erlotinib in recurrent glioblastoma multiforme: results of a phase II trial, Neuro-Oncol, 2004;6(4):384, Abstract TA- 59. 77.Vogelbaum MA, Peereboom D, Stevens G, et al., Phase II trial of the EGFR tyrosine kinase inhibitor erlotinib for single agent therapy of recurrent Glioblastoma Multiforme: Interim results, J Clin Oncol, 2004 ASCO Annual Meeting Proceedings, 2004;22(14S):Abstract 1558. 78.Raizer JJ, Abrey LE,Wen P, et al., A phase II trial of erlotinib (OSI- 774) in patients (pts) with recurrent malignant gliomas (MG), not on EIAEDS, J Clin Oncol, 2004 ASCO Annual Meeting Proceedings, 2004;22(14S):Abstract 1502. 79.Van Den Bent MJ, Brandes A, Rampling R, et al., Randomized phase II trial of erlotinib versus temozolomide or BCNU in recurrent glioblastoma multiforme (GBM): EORTC 26034, J Clin Oncol, 2007 ASCO Annual Meeting Proceedings Part I,
- 14. 2007;25:Abstract 2005. 80.Mellinghoff IK,Wang MY, Vivanco I, et al., Molecular determinants of the response of glioblastomas to EGFR kinaase inhibitors, N Engl J Med, 2005;353:2012–24. 81.Wick W, Naumann U and Weller M, Transforming growth factorbeta: a molecular target for the future therapy of glioblastoma, Curr Pharm Des, 2006;12:341–9. 82.Hegi ME, Diserens AC, Gorlia T, et al., MGMT gene silencing and benefit from temozolomide in glioblastoma, N Engl J Med, 2005;352:997–1003. 83.Graff JR, McNulty AM, Hanna KR, et al., The protein kinase Cbeta-selective inhibitor, Enzastaurin (LY317615.HCl), suppresses signaling through the AKT pathway, induces apoptosis, and suppresses growth of human colon cancer and glioblastoma xenografts, Cancer Res, 2005;65:7462–9. 84.Fine HA, Kim L, Royce C, et al., Results from phase II trial of enzastaurin (LY317615) in patients with recurrent high grade gliomas, J Clin Oncol, 2005 ASCO Annual Meeting Proceedings, 2005;23(16S Pt I of II):Abstract 1504. 85.Butowski NA, Lamborn K, Chang S, et al., Study of enzastaurin plus temozolomide during and following radiation therapy in patients with newly diagnosed glioblastoma multiforme (GBM) or gliosarcoma, J Clin Oncology, 2007 ASCO Annual Meeting Proceedings, 2007;25(18S):Abstract 12511. 86.Kaur B, Tan C, Brat DJ, et al., Genetic and hypoxic regulation of angiogenesis in gliomas, J Neurooncol, 2004;70:229–43. 87.Bao S,Wu Q, Sathornsumetee S, et al., Stem cell-like glioma cells promote tumor angiogenesis through vascular endothelial growth factor, Cancer Res, 2006;66:7843–8. 88.Vredenburgh JJ, Desjardins A, Herndon JE 2nd, et al., Phase II trial of bevacizumab and irinotecan in recurrent malignant glioma, Clin Cancer Res, 2007;13(4):1253–9. 90.Farhadi MR, Capelle HH, Erber R, et al., Combined inhibition of vascular endothelial growth factor and platelet-derived growth factor signaling: effects on the angiogenesis, microcirculation, and growth of orthotopic malignant gliomas, J Neurosurg, 2005;102:363–70. 91. Kesari S, Ramakrishna N, Sauvageot C, et al., Targeted molecular therapy of malignant gliomas, Curr Neurol Neurosci Rep, 2005;5:186–97.