Neck of femur fracture & Trochanteric femur fracture
•Als PPTX, PDF herunterladen•
23 gefällt mir•1,330 views

Neck of femur fracture, Intertrochanteric femur fracture classification, reduction, treatment, adverse outcome of treatment and management

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Neck of femur fracture & Trochanteric femur fracture
Ähnlich wie Neck of femur fracture & Trochanteric femur fracture (20)
Mehr von Yash Oza
Mehr von Yash Oza (12)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Neck of femur fracture & Trochanteric femur fracture
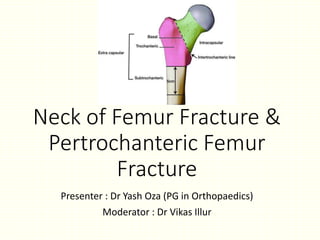
- 1. Neck of Femur Fracture & Pertrochanteric Femur Fracture Presenter : Dr Yash Oza (PG in Orthopaedics) Moderator : Dr Vikas Illur
- 2. Anatomy
- 3. Neck Shaft Angle Portion of neck that is intracapsular is deficient in cambium layer
- 6. Neck of femur Fracture
- 7. Assessment of Patient • MOI • Elderly female, Osteoporotic , Fall sideways • Young patients – High energy trauma – Associated with Shaft femur fracture • Military person – Stress fracture due to repetitive cyclic loading • Sign & Symptoms • Leg is shortened and externally rotated • All motions are painful • Neurovascular injury is extremely rare
- 8. Imaging studies • Xray • Diagnosis & treatment choice can be based on AP view only. • In equivocal cases lateral xray may be helpful determining displacement • AP xray with 10-15degree internal rotation taken to eliminate anteversion.
- 9. • Technetium bone scan • It was done in past In suspected NOF # cases with normal xray • CT Scan • More accurate in finding occult fracture • MRI is more accurate than CT finding occult fracture • PET-CT at 6 week could detect recovery of vascularity and could predict risk of ANV
- 10. • Pre Op Care • Role of traction • Reduces the perfusion of head by MCFA and also negatively influence venous circulation • No benefit in pain & Quality of reduction • So Not used • Medication • Pain killers
- 11. Classification • A number of classification system have been devised for NOF# but in any event location of the intracapsular fracture has not been shown to influence management or outcome. • Various classification are – • Anatomical Classification • Garden Classification • Pauwels Classification • AO/ATO Classification
- 12. Garden Classification Type 1: Incomplete fracture. So called abducted or impacted fracture. The trabecular pattern of inferior neck is not interrupted. They appear bent. Type 2: Complete fracture of femoral neck without displacement. Trabecular pattern of weight bearing portion of neck is interrupted but their alignment is undisturbed.
- 13. Garden’s classification • Type3: Complete fracture with partial displacement. The trabecular pattern of femoral head does not line up with trabecular pattern of acetabulum. • Type4: Complete fracture with complete displacement. Trabecular pattern of femoral head lines up with trabecular pattern of acetabulum.
- 14. Pauwels Classsification An increasing angle leads to a more unstable fracture and an increase in the shear stress at the fracture site. This shear leads to higher rates of nonunion.
- 16. Outcome measures for NOF# • Most commonly reported outcome is mortality • Studies on fixation provide outcome data on AVN, Fixation failure and nonunion • Arthroplasty complication include – dislocation, infection • There are many hip-specific outcome score – • Harris Hip Score • Oxford Hip Score • Johanson Hip Score • Charnley Score • Activities of Daily living (ADLs) Score • Functional Indenpendance Measure (FIM)
- 17. Treatment Options • Non-surgical • Surgical • Internal Fixation • Arthroplasty • Depends on • Age of the patient • Amount of displacement • Amount of comminution • Vascular impairment • Interval between injury and reduction
- 18. Non - surgical • It is an option for undisplaced NOF# in young and patient unfit for the surgery • Methods • skin traction • Derotation casts • Outcome • Displacement • Non Union • AVN
- 19. Methods to evaluate accuracy of reduction • Garden’s Alignment index • In AP view, the angle formed by central axis of medial trabecular system in capital fragment and the medical cortex of shaft • In Lateral view, the central axis of head and neck lie in straight line.
- 20. • Lowell Method • Femoral Head with the neck forms “S” or “inverted S” shaped curve in any projection • If fracture is not reduced it produces broken “C” curve
- 21. Surgical Treatment • CRIF • Multiple Pin (Knowles, Moore) • Cannulated Hip Screw ( ANIS) • AO Cannulated screw • Cannulated hip bolt • Sliding or telescopic screw (DHS) • SP Nailing • ORIF • Mayer’s muscle pedicle graft and internal fixation • Arthroplasty • Hemiarthroplasty • Austin Moore prosthesis • Thompson’s prosthesis • Bipolar • THR
- 22. Closed reduction and Internal fixation • For Garden I & II fractures • Garden I • Incomplete or impacted fractures • Least risk of displacement and AVN • Multiple Pin/CC Screw/Moore pins can be used • Garden II • Sliding hip screw or Knowles pin may be required due to bony instability
- 23. Open Reduction & Internal fixation • Indications are – • Failed CRIF after 2 attempts • Age >60yrs • Very young adults & children where absolute reduction is important • Advantages • Spinning of head can be controlled • Bone grafting can be done • Arthrotomy or joint aspiration can be done which may benefit reduction
- 24. • Disadvantages • Interference with blood supply • Higher rate of non union • Infection
- 25. Multiple pins • Cheap • Easy fixation • Chance of penetrating hip less • Rotation forces prevented • Chances of AVN less
- 26. Compression Hip screw and plates • Advantages • No rotation takes place at # site • Cheaper • Early weight bearing • Incidence of proximal migration and cut-out is less • Implant failure is less • Disadvantages • The screw has potential to rotate the femoral head during incursion ( placing an accessory pin above the screw prior to screw insertion prevents rotation)
- 27. AO CC Screw • Newer method • Widely used in children and young adults • Early mobilization possible
- 28. Mayer’s muscle pedicle graft and internal fixation • Indication : • Displaced NOF# after closure of epiphyseal plate • Impacted # with AVN • Late diagnosed # • Non Union cases • Impending AVN • Alternate procedure to arthroplasty in early age group Graft : 3 cm from the tip of GT ,which includes insertion of Quadratus femoris
- 29. • Advantages • In posterior comminution , fracture stability enhanced as graft is posterior • Additional source of blood supply to head • Direct visualization of neck • Permits accurate reduction since the capsule is opened • Disadvantages • Possible damage to remaining posterior blood supply of head • Risk of infection • Extensive soft tissue dissection • Contraindication • Short Life expectancy • Pathological fracture • Ispilateral arthritis hip
- 30. Hemi-Arthroplasty • Absolute indication • Age>65yrs , displaced # • NOF # that can’t be reduced • Fixation failure • Pathological NOF# • Old undiagnosed NOF#, >3week • NOF# with complete dislocation of head • Mentally retarded patient • Uncontrolled seizures
- 31. • Relative Indication • Advanced physiological age with life expectancy not more than 10-15 yrs • Parkinson’s Ds, Hemiplegia, other neurological Ds • Osteoporosis • Pauwel type 3 • # involving superior weight bearing surface of head • Contraindication • Active young adult • Severe osteoporosis • Acetabular involvement • Pre-Existing sepsis
- 32. • Advantages • Immediate mobilization with weight bearing • Eliminates AVN, Non union, Fixation failure • In failure cases revision arthroplasty can be done • Lesser reoperation rates • Disadvantages • More extensive procedure than internal fixation • Risk of infection • In case of mechanical failure, salvage procedure becomes complicated
- 33. • Types of Prosthesis • Austin Moore Prosthesis • Thompson’s Prosthesis • Bipolar Prosthesis ( Low friction Arthroplasty) AMP Thompson’s
- 34. THR • Performed to salvage complication of NOF# • Other indication – • Severe RA and OA • Active patient with age > 70yrs who suffers a stress # • NOF# Metastasis in acetabulum
- 35. Adverse Outcomes • Fixation failure • It increases risk of non-union • Diagnosis : Increasing pain, shortening of leg, xray • THR is best treatment option
- 36. • Non Union • Occurs in 10-20% • Diagnosis : • Pain at # site even after 6 month post-op • Xray • Causes • Vascular insufficiency • Shearing forces at # site • Increased intraarticular pressure • Inaccurate Reduction • Fixation failure • Arthroplasty is ideal treatment option in old patient • If patients is <40yrs age then • Revision fixation • Muscle pedicle graft • Vascularized fibula graft • Valgus osteotomy
- 37. • AVN • It leads to joint incongruity, pain, degenerative joint disease • Diagnosis : • Groin Pain on walking • Xray • Technitium-99m bone scan • MRI is sensitive in detecting aseptic necrosis ( Though not used as metallic implants are in situ) • Treatment • Analgesic & physiotherapy • Vascularized fibular grafting • Osteotomies of proximal femur • THR
- 38. • Prosthesis Dislocation • Choice of surgical approach and implant size influence the dislocation rates • Small Femur Head – More dislocation • Posterior Approach - More dislocation • Treatment : • Closed Reduction possible with Unipolar & THR implants • In bipolar prosthesis closed reduction is associated with risk of implant disassociation • In Bipolar prosthesis Open reduction may be required after failed closed reduction • Prosthesis Loosening • A late complication and not seen routinely because of limited life expectancy of patients
- 39. • Osteotomies • McMarray’s – Displacement osteotomy • Valgus Osteotomy Aim – Change the Femoral Neck angle to 150 degree
- 40. Intertrochanteric Femur Fracture • Most common fracture of the proximal femur • It is extracapsular fracture
- 41. • Mechanism of injury • Elderly patient – fall sideways • Young Patients – High velocity trauma • Clinical features • Limb is shortened and externally rotated • Swelling over hip region • Ecchymosis over GT may be seen later • Hip movements painful
- 42. • Xray • AP(with traction) & Lateral view • AP Views – usefull knowing # obliquity, quality of bone and allows comparison with normal side • Lateral View – help to assess size, location and comminution of posterior fragment and help determine fracture stability • Technetium bone scan • To diagnose occult #, it requires 2-3 days to become positive • MRI • To diagnose occult #, It reveals # within 24 hours of injury
- 43. Classification • Boyd & Griffin Classification • It includes all 3 from extracapsular NOF# to subtrochanteric #
- 44. • Evan’s Classification • Based on direction of fracture
- 46. Treatment • Non operative • Operative
- 47. Non operative Method • Indication • Unfit for surgery • Non-ambulatory patients • Protocol • Early mobilization – bed chair mobilization – but ambulation is delayed • Maintain traction until fracture union occurs , usually 10-12 weeks
- 48. • Methods • Buck’s Traction • Russell Skeletal traction • Balanced traction in Thomas splint • Plaster spica • Derotation boot • Complication • Pressure sores • UTI • Joint contractures • Pneumonia • Thromoembolism
- 49. Buck’s Traction Russell Skeletal traction Derotation boot
- 50. Operative Treatment • Goal of surgery is strong & Stable fixation • Factors determining strength of fracture fragment are – • Bone Quality • Fracture Geometry • Reduction • Implant Design • Implant placement
- 51. Reduction methods • Closed reduction • Fracture table is essential • Ideally slight valgus position on AP to be achived • In Lateral Femoral head neck and trochanteric area to be in straight line • Patella is always facing upwards
- 52. • Open reduction • Indication – • Failed closed reduction • Large posterior spike • Reverse oblique # • If gap exist medially or posteriorly Types : - • Anatomical reduction • With help of clamps & forceps anatomically stable reduction is achieved • Non-Anatomical reduction • In severely comminuted # where anatomical reduction even with open methods is difficult or impossible • Osteotomy is done to convert it into stable reduction 1. Medial Displacement Osteotomy ( Dimon-Hughston) 2. Valgus Osteotomy (Sarmiento) 3. Lateral Displacement osteotomy (Wayne county)
- 53. Implants • Nail Plate devices • S-P nail & Plates • Jewette Nail • Thornton Nail • Holt Nail • AO blade plate
- 54. Smith Peterson nail & plate Jewette Nail AO Blade plate
- 56. • Sliding Compression Screw plate devices • Richards • Calandruccio plate • Medoff sliding plate • DHS • Dynamic Condylar screw • Percutaneous compression plate
- 58. • Intramedullary devices • Condylo cephalic • Ender’s nail • Single rigid condylocephalic rods of Harris • Cephalomedullary Nail • Gamma nail • Russell taylor reconstruction nail • The uniflex nail • Proximal femoral nail • Recon nail
- 59. Ender’s nail Single rigid condylocephalic rods of Harris Gamma nail
- 61. Positioning of the Lag Screw • Correct fracture reduction is prerequisite for being able to correctly position the lag screw • An angle of 130 or 135 degree appears to be optimal • The lag screw position is low to the central in AP and central in lateral views. • Screw tip to apex distance should be twice the diameter of lag screw (8*2=16mm) . This prevents screw cutout
- 62. Trochanteric fracture with loss of lateral support • Loss of lateral support in IT fracture allows femur to displace medially. • Each degree of medialization increases risk of fixation failure by 1% • Mean degree of lateralization with slinding screw (10%) is more than intramedullary nail (2%) • So, IT fracture with loss of lateral support should be treated with intramedullary nailing
- 63. Arthroplasty • Indication • Pathological # • Severe osteoporotic bone • Renal Dialysis Patient • Pre-existing arthritis • Patient unsuitable for internal fixation • Hemiarthroplasty & THR both can be done
- 64. Post Op Care • Pain Control • Early mobilization • DVT prophylaxis ( Mechanical & Chemical) • Nutrition
- 65. Complication • Loss of fixation – mostly due to eccentric placement of the screw – Screw cutout • Medialization ( More with sliding hip screw) • Malrotation deformity ( more with intramedullary nail)
- 66. • Refracture around the implant • IM nail has more risk of # around implant • Common causes are • A large diameter nail • Large diameter distal screw • Distal screw lose to the tip • Overtightening of distal screw • Too short nail for subtrochanteric type fracture • Treatment – Exchange nail,Plate fixation • For refracture at proximal end Arthroplasty should be considered
- 67. • Non Union • Very rare • Head AVN • 1-2% risk • Limb shortening • Varus malunion may lead to limb shortening
- 68. Summary
- 70. Thank you