Acyanotic congenital heart diseases: 2
•Als DOCX, PDF herunterladen•
4 gefällt mir•2,121 views

Presentation Precordial findings ECG findings CXR findings Prognosis Management of Coarctation of aorta Pulmonary valve stenosis Aortic Stenosis

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Acyanotic congenital heart diseases: 2
Ähnlich wie Acyanotic congenital heart diseases: 2 (20)
Mehr von Yapa
Mehr von Yapa (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Acyanotic congenital heart diseases: 2
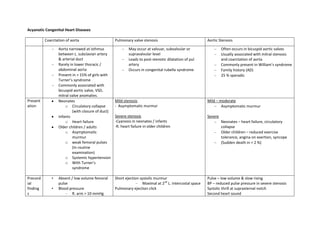
- 1. Acyanotic Congenital Heart Diseases Coarctation of aorta Aorta narrowed at isthmus between L. subclavian artery & arterial duct Rarely in lower thoracic / abdominal aorta Present in > 15% of girls with Turner’s syndrome Commonly associated with bicuspid aortic valve, VSD, mitral valve anomalies. Neonates o Circulatory collapse (with closure of duct) Infants o Heart failure Older children / adults o Asymptomatic murmur o weak femoral pulses (In routine examination) o Systemic hypertension o With Turner’s syndrome Present ation Precord ial finding s • • Absent / low volume femoral pulse Blood pressure – R. arm > 10 mmHg Pulmonary valve stenosis Aortic Stenosis May occur at valvuar, subvalvular or supravalvular level Leads to post-stenotic dilatation of pul artery Occurs in congenital rubella syndrome Often occurs in bicuspid aortic valves Usually associated with mitral stenosis and coarctation of aorta Commonly present in William’s syndrome Family history (AD) 25 % sporadic Mild stenosis - Asymptomatic murmur Mild – moderate Asymptomatic murmur Severe stenosis -Cyanosis in neonates / infants -R. heart failure in older children Severe Short ejection systolic murmur – Maximal at 2nd L. intercostal space Pulmonary ejection click Pulse – low volume & slow rising BP – reduced pulse pressure in severe stenosis Systolic thrill at suprasternal notch Second heart sound Neonates – heart failure, circulatory collapse Older children – reduced exercise tolerance, angina on exertion, syncope (Sudden death in < 2 %)
- 2. ECG CXR higher than in legs – BP in left arm depends on site of coarctation • Prominent left ventricular impulse • Short ejection systolic murmur – Maximal at 2nd L. intercostal space & below left scapula posteriorly • Continuous murmur heard in older children due to development of collateral arteries L. ventricular hypertrophy and strain pattern in older children “3” sign- due to abnormal aortic contour Rib notching- due to collateral arteries Ba swallow may show narrowing of the oesophagus “E” sign Echocardiography & Doppler studies In severe stenosis • Jugular venous pulse – Prominent “a” wave • parasternal heave • Thrill at 2nd L. intercostal space • Soft, delayed P2 Soft aortic component Single P2 or paradoxical splitting Ejection systolic murmur Radiates to neck & down the L.sternal border Apical ejection click R. ventricular hypertrophy p pulmonale L. ventricular hypertrophy +/- strain pattern Post-stenotic dilatation of pul. Artery R. ventricular hypertrophy Echocardiography Post stenotic dilatation of ascending aorta L. ventricular hypertrophy may be present
- 3. (Demonstrates the site of coarctation ) MRI Cardiac catheterization & angiography Progno sis Manag ement Surgical correction 1. Excision of narrowed segment with end-to-end anastomosis of aorta (Rarely a patch / tube graft is necessary) 2. L. subclavian flap procedure Surgical mortality < 2 % < 4 % incidence of restenosis Risk of recurrent laryngeal / phrenic nerve damage, spinal cord ischaemia Balloon dialatation (Is used to prevent / treat restenosis ) Thickened pulmonary valve Pulmonary artery dilatation R. ventricular hypertrophy Tricuspid regurgitation R. atrial enlargement • Often decreases spontaneously • • In 27 % progressive obstruction Pressure gradient > 50 mmHg →Surgery – Balloon dilatation is the treatment of choice – Long term results excellent – Risk of pul. regurgitation, restenosis & rarely IE • • Progresses with time Regular clinical & echocardiographic assessment of disease progress is necessary • Mild stenosis – no restriction of activities • Surgery If clinically severe stenosis or pressure gradient across valve is > 50 mmHg – Transcatheter balloon dilatation – surgical valvotomy – Valve replacement (if unrelievable obstruction or AR)