Image of Thoracic Aortic Disease
•Als PPTX, PDF herunterladen•
6 gefällt mir•2,160 views

Image of Thoracic Aortic Disease Reference: 2010 Guidelines on Thoracic Aortic Disease Circulation. 2010;121:e266-e369

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Image of Thoracic Aortic Disease
Ähnlich wie Image of Thoracic Aortic Disease (20)
Mehr von Sun Yai-Cheng
Mehr von Sun Yai-Cheng (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Image of Thoracic Aortic Disease
- 1. Image of Thoracic Aortic Disease Circulation. 2010;121:e266-e369. 2010 Guidelines on Thoracic Aortic Disease
- 2. Precontrast image demonstrates a high attenuation aortic hematoma indicating an acute aortic event. Images obtained with contrast demonstrate the contrast- filled aortic lumen and the hematoma as a relatively lower attenuation band.
- 3. Traumatic aortic rupture Traumatic injury with pseudoaneurysm (T) in the proximal descending thoracic aorta, numerous bilateral rib fractures, and small bilateral pleural effusions, with no significant mediastinal hematoma.
- 4. Mimic of aortic dissection created by motion of the aortic root Image at the level of the right pulmonary artery demonstrates a normal descending thoracic aorta and pseudodissection of the ascending aorta due to motion artifact that occurs on non–ECG gated CT (arrow). Image at the aortic root shows a double contour to the aortic root that may simulate a dissection flap (arrow).
- 5. Axial CT image demonstrates a low attenuation crescent of material anterior to the innominate artery. Left brachiocephalic vein mimics an intramural hematoma
- 6. Normal anatomy of thoraco-abdominal aorta with standard anatomic landmarks for reporting aortic diameter as illustrated on CT 1. Aortic sinuses of Valsalva 2. Sinotubular junction 3. Mid ascending aorta (midpoint in length between Nos. 2 and 4) 4. Proximal aortic arch (aorta at the origin of the innominate artery) 5. Mid aortic arch (between left common carotid and subclavian arteries) 6. Proximal descending thoracic aorta (begins at the isthmus, approximately 2 cm distal to left subclavian artery) 7. Mid descending aorta (midpoint in length between Nos. 6 and 8) 8. Aorta at diaphragm (2 cm above the celiac axis origin) 9. Abdominal aorta at the celiac axis origin
- 7. Arch aneurysm with dissection flap Arch dissection, 2-D view Arch dissection (arrow) with color-flow Doppler margination.
- 8. Artifact mimicking dissection. Top left, 2-D view. Top right, Color-flow Doppler without margination. Bottom, Artifact not seen in this view.
- 9. Takayasu arteritis Note narrowing of the arterial lumen and circumferential soft tissue thickening of the walls of the great vessels and thoracic and abdominal aorta. Panel A, Image through the great vessels with narrowing of the left common carotid and left subclavian arteries. Panel B, Mid descending thoracic aorta (arrowheads). Panel C, Aorta just above the diaphragm (arrowheads). Panel D, Infrarenal aorta.
- 10. Classes of intimal tears I. Classic dissection with intimal tear and double lumen separated by septum. II. Intramural hematoma. No intimal tear or septum is imaged but is usually found at surgery or autopsy. DeBakey Types II and IIIa are common extent of this lesion. III. Intimal tear without medial hematoma (limited dissection) and eccentric aortic wall bulge. Rare and difficult to detect by TEE or CT. IV. Penetrating atherosclerotic ulcer usually to the adventitia with localized hematoma or saccular aneurysm. May propagate to Class I dissection, particularly when involving ascending aorta or aortic arch. V. Iatrogenic (catheter angiography or intervention)/ traumatic (deceleration) dissection.
- 11. Type A aortic dissection from the cranial to caudal direction Although the flap appears to disappear in the infrarenal, it is actually compressed against the anterior wall of the aorta in Panel G (arrowheads) and it is clearly present caudally in the common iliac arteries in Panel H. Hemopericardium (asterisk) is visible in Panel D. Bowel wall thickening (arrowheads) indicates ischemia in Panel I.
- 12. Type A Aortic dissection with thrombosed false lumen and left renal artery involvement Demonstrates marked narrowing of the true lumen, patent right renal artery arising from the true lumen (bottom left, arrow), and narrow left renal artery compressed by thrombus in the false lumen, with secondary decreased enhancement of the left kidney compared with the right kidney. *Thrombus in false lumen.
- 13. Aortic dissection classification: DeBakey and Stanford Classifications
- 14. Type B aortic dissection with mediastinal hematoma and pleural blood. Ruptured Type B aortic dissection with mediastinal hematoma (*) and pleural blood. Left, Flap arises in the proximal descending thoracic aorta, with faint contrast-enhanced blood adjacent to the site of rupture outside the confines of the aortic wall (arrow).
- 15. Intramural hematoma demonstrated as a low- attenuation band of hematoma (arrows) in the aortic wall on CT images.
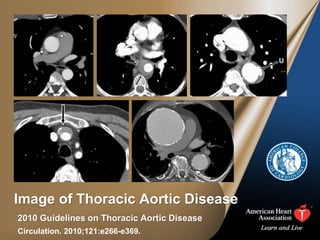
- 16. Penetrating atherosclerotic ulcer of the proximal descending thoracic aorta. Axial CT images at the level of the aortopulmonary window (left) and at the level of the left pulmonary artery (right) demonstrate a small penetrating ulcer (long arrow, U) that extends beyond the expected confines of the aortic lumen with adjacent intramural hematoma both at the level of the ulcer itself and that extends a few centimeters caudally in the wall of the descending thoracic aorta (short arrows).
- 17. Descending aneurysm classification. Descending aneurysms are classified as involving thirds of the descending thoracic aorta and various combinations. A involves the proximal third, B the middle third, and C as the distal third. Thoracoabdominal aneurysms are classified according to the Crawford classification: Type I extends from proximal to the 6th rib and extends down to the renal arteries. Type II extends from proximal to the 6th rib and extends to below the renal arteries. Type III extends from distal to the 6th rib but from above the diaphragm into the abdominal aorta. Type IV extends from below the diaphragm and involves the entire visceral aortic segment and most of the abdominal aorta. Juxtarenal and supraenal aneurysms are excluded.
- 18. Ultrasound image of aortic atheroma
- 19. Porcelain aorta. Top left and right, PA and lateral CXR show an anterior mediastinal mass with curvilinear calcifications most likely representing the wall of an ascending aortic aneurysm. Bottom left, CT scan slice at the level of the right pulmonary artery confirms a 10-cm aneurysm of the ascending aorta with dense mural calcifications. Bottom right, A maximum intensity projection in the oblique sagittal plane better demonstrates the fusiform aneurysm beginning at the sinotubular ridge and extending into the aortic arch. Dense mural calcification extends into the proximal descending aorta.