Review Paper-Gene Therapy for the Treatment of Cystic Fibrosis
•Als DOC, PDF herunterladen•
3 gefällt mir•3,098 views


Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Ähnlich wie Review Paper-Gene Therapy for the Treatment of Cystic Fibrosis
Ähnlich wie Review Paper-Gene Therapy for the Treatment of Cystic Fibrosis (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Review Paper-Gene Therapy for the Treatment of Cystic Fibrosis
- 1. Stephanie M. Delgado BIOL 3095, Section 140, No. 804-09-2123 Dra. Eneida Díaz December 13, 2009 REVIEW Gene Therapy for the Treatment of Cystic Fibrosis Abstract Cystic fibrosis is an autosomal recessive genetic disorder caused by various mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene. It affects over 70, 000 people worldwide, mostly of Caucasian descent. It should be possible to treat an autosomal recessive disease such as cystic fibrosis with insertion of one copy of normally functioning DNA into the affected cells, independent of the class of mutation the recipient had before gene therapy. Although easy in concept (and in vitro), in practice gene therapy has proven to be quite difficult in treating Cystic Fibrosis. There are biological barriers that must be surmounted as well as different vectors that have been tried without encouraging results. This article focuses on these aspects of gene therapy for Cystic fibrosis as well as the human clinical trials that have been performed. Table of Contents 1. Introduction 1 2. Degree of correction required 2 3. Barriers for gene delivery 2 4. Vectors 3 4.1 Viral Vectors 4 4.2 Nonviral vectors 4 5. Clinical studies successes and failures 4 6. Conclusions 9 7. References 10 1. Introduction Cystic Fibrosis (CF) is an autosomal recessive genetic disorder. It’s caused by various mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene on chromosome 7q31.2. These mutations cause imbalanced ion and water movement across the
- 2. 2 airway epithelium, resulting in accumulation of sticky mucus, chronic bacterial infection and inflammation. Although this disease also affects other organs, lung disease contributes mainly to morbidity and mortality in CF patients. Gene therapy is a treatment that consists of using genetic material with a curative purpose. Gene therapy aims to get rid of genetic diseases at their source by targetting the faulty gene.The objective of this treatment for Cystic Fibrosis is to insert a normal copy of the CFTR gene into the affected cells in order to restore normal functions (Davies, 2006). With the discovery and cloning of the CFTR gene in 1989, CF was one of the first diseases chosen to be treated with gene therapy. There are several reasons for this, but mainly it’s because CF is a monogenic disease (caused by only one gene), the CFTR gene is relatively large, and small quantities of the CFTR protein are needed to correct the chloride transport. Although fairly simple in concept, after twenty years of intense research and clinical trials, there are still many obstacles that must be overcomed before gene therapy for this disease is successful. (Ostrowski, 2007). 2. Degree of correction required One of the most important things to consider when administering gene therapy is the minimal percentage of cells with a non-CF phenotype that will be required to normalize the functions of the CF bronchial epithelial layer. One study concludes that only 10% of non-CF cells are sufficient to normalize the abnormal Na+ absorption and Cl- secretion associated with CF (Dannhoffer, 2009). This study is consistent with previous research that found that only about 5-10% of corrected cells are needed to correct the abnormal Cl- transport, although by measuring the IL-8 secretion and the basal Isc they also concluded that this percentage is enough to correct the inflammation and Na+ transport (Ziady, 2006). Although we know the percentage of cells needed to normalize the CFTR dependant functions in vitro, it’s still not clear the percentage necessary in vivo or which specific cells should be transduced.
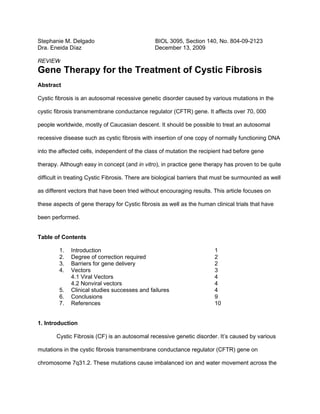
- 3. 3 3. Barriers for gene delivery Humans are well protected against the invasion of introduced genetic material by intracellular and extracellular barriers. This has been an evolutionary adaptation designed to maintain our genetic stability. That’s why genetic transfer agents (GTA’s) or vectors have to be used for gene therapy in cystic fibrosis. These delivery systems usually are made of a polynucleotide, encoding the therapeutic gene, and a carrier which “should facilitate transport of the therapeutic gene from the extracellular space into the nuclear compartment, where transcription can take place” (Conese et al, 2007). But depending on the method of administration these vectors have to penetrate many defense mechanisms like circulating antibodies in the bloodstream, a mucus layer that is constantly cleared by cilliae in the airway, macrophages, and immune responses which can clear the positively transduced cells (Price et al, 2007). 4. Vectors The target of CF gene therapy is the airway epithelium. Gene delivery systems have been developed to reach this site. A carrier molecule called a vecto is used to deliver the therapeutic gene to the patient's target cells in the airway epithelium. The vector then unloads its genetic material containing the CFTR gene into the target cell. The generation of a functional protein product from the therapeutic gene restores the target cell to a normal state. Example of gene delivery system. From Eubanks, 2001.
- 4. 4 4.1 Viral vectors Some gene transfer agents have been developed from viruses. These include adenoviral vector, adeno-associated viral vectors, lentivirus vectors, and poxvirus and, Sendai and herpes virus (Buckley et al, 2008; Ferrari et al, 2007; Rogers et al, 2008). Most of these viral vectors have currently limited use for CF gene therapy because of inefficient gene expression after repeat administration, but lentiviral vectors may be an exception (Buckley et al, 2008). Lentiviruses transfect non-dividing cells and may, therefore, be suitable for transfection of terminally differentiated airway epithelial cells. The virus stably integrates into the genome of transfected cells and expression is therefore likely to last for the life-time of the cell, but still present some problems like risk of insertional mutagenesis and proto-oncogene activation (Yu, 2007). 4.2 Nonviral vectors Non-viral gene transfer agents are generally less efficient than viral vectors in transfecting lung epithelium. However, if free of “non-human” protein components, they are less likely to induce an immune response, thereby allowing for repeat administration, which is a crucial for the treatment of CF and other chronic diseases that will require life-long treatment (Griesenbach and Eric, 2008). These synthetic vectors consist generally of DNA encoding the therapeutic gene in the form of a plasmid, combined with a carrier generally of a synthetic compound, which mimics the functions of a viral capsid, but should lack its immunogenicity. While this development is of major interest, much work needs to be done to accomplish its full therapeutic potential. 5. Clinical studies successes and failures Since 1993, twenty-five phase I/II safety clinical trials have been carried out using a variety of viral and nonviral gene transfer agents (GTA’s). These trials have involved around 450
- 5. 5 CF patients (Griesenbach and Alton, 2008). As we can see on Table # 1 on the appendix the first trials mostly focused on the nasal epithelium, as it’s more secure and allows easy access and sampling. When an acceptable safety profile had been achieved, the GTA’s were administered directly into the lung. Adenovirus vectors were first used, until it was clear that these were not efficient transducing into the human airway epithelial cells (target cells for CF gene therapy) because there was no adenoviral receptor in their membrane. Also these adenoviral vectors could not be administered repeatedly, something necessary for a life-long chronic disease like CF (Griesenbach and Alton, 2007). The adenoviral vectors were replaced with adeno-associated (AAV) vectors, but the most recent phase I/II trials were unsuccessful. Other nine clinical trials have used nonviral GTA’s. These have shown more promise as they are more likely to be repeatedly administrable and have shown approximately 25% correction of the molecular defect in CF patients. Groups like the UK CF Gene Therapy Consortium and Copernicus Inc. are currently preparing clinical trials focusing on nonviral GTA’s. It is hoped that next-generation vectors will lead to effective gene transfer and sustained cure of the pulmonary disease associated with cystic fibrosis (O’Sullivan and Freedman, 2009). 6. Conclusions Cystic Fibrosis is a disease that affects over 70,000 individuals worldwide. It’s a single gene disorder with insufficient treatment options and non-invasive access to the target organ, which is the lung. For these reasons and because of its genetic features, it was one of the first diseases considered for gene therapy. Although very promising at first, gene therapy for CF has encountered many problems like the absence of an appropriate vector. But significant progress is currently being made in the development of viral and nonviral vectors that are more effective. It can be concluded that new and longer clinical trials are needed as well as the development of new vectors to be tested in these clinical trials. Until then, gene therapy as a cure for the basic
- 6. 6 defect that could normalise the functions and life expectancy for those born with CFTR mutations is still a great hope more than a reality. 7. References Buckley SMK , Howe SJ, Sheard V, Ward NJ, Coutelle C, Thrasher AJ, Waddington SN, McKay TR. 2008. Lentiviral transduction of the murine lung provides efficient pseudotype and developmental stage-dependent cell-specific transgene expression. Gene Therapy 15: 1167–1175 Conese M, Boyd C, Di Gioia S, Auriche C, Ascenzioni F. 2007. Genomic Context Vectors and Artificial Chromosomes for Cystic Fibrosis Gene Therapy. Current Gene Therapy 7: 175-187 Dannhoffer L, Blouquit-Laye S, Regnier A, Chinet T. 2009. Functional Properties of Mixed Cystic Fibrosis and Normal Bronchial Epithelial Cell Cultures. American Journal of Respiratory Cell and Molecular Biology 40: 717–723. Davies JC. 2006. Gene and cell therapy for cystic fibrosis. Paediatric Respiratory Reviews 7(1):S163-S165. Eubanks M. 2001. Gene Therapy for CF. Environmental Health Perspectives 109: A16 Ferrari S, Griesenbach U, Iida A, Farley R, Wright AM, Zhu J, Munkonge FM, Smith SN, You J, Ban H, Inoue M, Chan M, Singh C, Verdon B, Argent BE, Wainwright B, Jeffery PK, Geddes DM, Porteous DJ, Hyde SC, Gray MA, Hasegawa M, Alton EW. 2007. Sendai virus- mediated CFTR gene transfer to the airway epithelium. Gene Therapy 14: 1371–1379. Griesenbach U, Alton EW. 2007. Progress and Prospects: Gene Therapy Clinical Trials (Part 1). Gene Therapy 14: 1439–1447. Griesenbach U, Eric WF. 2008. Gene transfer to the lung: Lessons learned from more than 2 decades of CF gene therapy. Advanced Drug Delivery Reviews 61: 128–139. Hyde SC, Pringle IA, Abdullah S, Lawton AE, Davies L, Varathalingam A, Nunez-Alonso G, Green A, Bazzani RP, Sumner-Jones SG, Chan M, Li H, Yew NS, Cheng SH, Boyd C, Davies JC, Griesenbach U, Porteous DJ, Sheppard DN, Munkonge FM, Walton EW, Gill DR. CpG-free plasmids confer reduced inflammation and sustained pulmonary gene expression. 2008. Nature Biotechnology 26: 549-551 Liu X, Luo M, Guo C, Yan Z, Wang Y, Engelhardt JF. 2007. Comparative biology of rAAV transduction in ferret, pig and human airway epithelia. Gene Therapy 14: 1543–1548. O’Sullivan BP, Freedman SD. 2009. Cystic fibrosis. Lancet 373: 1891–904 Ostrowski LE, Yin W, Diggs PS, Rogers TD, O’Neal WK, Grubb BR. 2007. Expression of CFTR from a ciliated cell-specific promoter is ineffective at correcting nasal potential difference in CF mice. Gene Therapy 14: 1492–1501 Price AR, Limberis MP, Wilson JM, Diamond SL. 2007. Pulmonary delivery of adenovirus vector formulated with dexamethasone–spermine facilitates homologous vector re- administration. Gene Therapy 14: 1594–1604. Rogers CS, Hao Y, Rokhlina T, Samuel M. 2008. Production of CFTR-null and CFTR- [Delta]F508 heterozygous pigs by adeno-associated virus-mediated gene targeting and somatic cell nuclear transfer. Journal of Clinical Investigation 118 (4): 1571-1577 Sumner-Jones SG, Davies LA, Varathalingam A, Gill DR, Hyde SC. 2006. Long-term persistence of gene expression from adeno-associated virus serotype 5 in the mouse airways. Gene Therapy 13: 1703–1713. Yu Z, McKay K, Asperen P, Zheng M, Fleming J, Ginn SL, Kizana E, Latham M, Feneley M, Kirkland PD, Rowe P, Lumbers ER, Alexander IE. 2007. Lentivirus vector-mediated gene transfer to the developing bronchiolar airway epithelium in the fetal lamb. The Journal of Gene Medicine 9: 429–439.
- 7. 7 Ziady AG, Davis PB. 2006. Current prospects for gene therapy of cystic fibrosis. Current Opinion in Pharmacology 6(5):515-521.
- 8. 8 Appendix Table 1. List of clinical trials Reference Route Trial design Results Adenovirus clinical trials Zabner et al. (1993) Nose Dose-escalation 2 × 106– NPD: decreased baseline towards non- 5 × 107 pfu n = 1/dose CF values mRNA: − ve, protein: − ve Crystal et al. (1994) Nose Dose-escalation 2 × 105– NPD: inconclusive, too variable 5 × 107 pfu n = 2/dose mRNA: 1/4 + ve, protein: 1/4 + ve Lung Dose-escalation 2 × 106– mRNA: − ve, protein: 1/4 + ve 5 × 109 pfu n = 1–2/dose Safety: no vector shedding. At highest dose transient inflammation. Knowles et al. (1995)Nose Dose-escalation 2 × 107– NPD: no change mRNA: 5/12 + ve 5 × 1010 pfu n = 3/dose Vehicle control applied on Safety: no toxic effects at low doses. At contralateral nostril highest dose mild mucosal inflammation 2/3 patients Hay et al. (1995) Nose Dose-escalation 2 × 105– NPD: decreased baseline + amiloride 5 × 108.5 pfu n = 1–2/dose towards non-CF values. Partial correction of Cl− transport Zabner et al. (1996) Nose Dose-escalation repeat NPD: partial correction of Cl− in some administration 2 doses patients, but reduced effect with 2 × 107–1 × 1010 pfu n = 4– subsequent administration. All patients 6/dose developed serum antibodies to vector, but not CFTR Bellon et al. (1997) Nose Dose-escalation 1 × 105– DNA: 6/6 + ve 4 × 108 pfu n = 2/dose Dose-escalation 1 × 107– 5.4 × 108 pfu n = 2/dose mRNA: 4/6 + ve, protein: 4/6 + ve Lung Dose-escalation 1 × 107– DNA: 1/6 + ve 5.4 × 108 pfu n = 2/dose mRNA: 1/6 + ve, protein: 2/6 + ve Expression was transient in both nose and lung Harvey et al. (1999) [ Lung Dose-escalation Sampled 3 and 30 days after each administration mRNA: Repeat administration 3 1st administration + ve only with highest doses 106–1 × 109 pfu dose, transient (− ve by day 30) n = 2/dose 2nd administration + ve only with intermediate dose, − ve by day 30 3rd administration no expression Anti- Ad neutralising antibodies detected but no close correlation with loss of expression
- 9. 9 Zuckerman et al. Lung Dose-escalation 2 × 109– DNA: + ve on day 4, transient (1999) 2 × 1011 pfu n = 2–3/dose Immune response: Ad-specific T-cells, mild humoral response Safety: mild flu-like symptoms observed, resolved about day 10 Joseph et al. (2001) Lung Dose-escalation 8 × 106– DNA: 4/5 + ve on day 2 2.5 × 1010 pfu n = 2–3/dose mRNA: 3/5 + ve on day 2 Perricone et al. DNA: all + ve on day 2 (2001) mRNA: 4/13 + ve on day 2 Expression transient, undetected by day 7. < 3% of airway epithelial cells transfected. Safety: Mild, non-specific inflammatory response (fevers, myalgia). Cleared within 24 h. AAV2 clinical trials Wagner et al. (1999) Nose Dose-escalation 1 × 102– DNA: 7/10 + ve day 14 1 × 105 RU Single and two doses n = 5/ 1/10 + ve day 41 group 1/10 + ve day 70 CFTR mRNA: − ve NPD: partial Cl− correction in some cases, effect transient Aitken et al. (2001) Lung Dose escalation 1010 DRP– DNA: 6/6 + ve up to day 30 with two 1013 DRP n = 3/group highest doses mRNA: − ve Safety: several adverse effects, three of which possible related to study (pneumonia, exacerbation) Wagner et al. (2002) Nose 1 nostril 105 RU, No change in: rate of sinusitis relapse, contralateral nostril placebo NPD, histopathology and IL-8. (n = 23) IL-10: increased vs. placebo at day 90 Flotte et al. (2003) Nose Dose escalation Nose: Lung 3 × 101 RU–1 × 109 RU NPD: no change placebo (n = 25) contralateral nostril Vector DNA: 2/25 + ve Lung: Vector DNA: some + ve, but cross- contamination from nose Safety: generally well tolerated, one adverse effect possible linked to treatment (pulmonary exacerbation) Moss et al. (2004) Lung Repeat admin: 3 doses, DNA: 6/6 + ve (only assessed after 3rd 30 days apart 1 × 1013 DRP dose) (n = 37)
- 10. 10 mRNA: − ve FEV1: trend in improvement day 30 IL-8 and IL-10: sputum IL-8 reduced after 1st dose, IL-10 no change Safety and immune response: well tolerated, active group developed AAV2-neutralising antibodies Moss et al. (2007) Lung Repeat admin: 3 doses No changes in spirometry, days of 30 days apart 1 × 1013 DRP antibiotic use or induced sputum (n = 102) markers (IL-8 + neutrophil elastase) Safety: well tolerated Non-viral clinical trials Caplen et al. (1995) DC- Dose escalation 10–300 mg Vector DNA: 7/8 + ve (some problems Chol/ DNA n = 3/dose with false + ves) DOPE Nose CFTR mRNA: − ve NPD: partial correction (20%) of Cl− defect towards normal at day 3, undetected by day 7 Safety: well tolerated Gill et al. (1997) DC- 40 + 400 μg DNA/nostril NPD: 2/8 transient correction of Cl− for Chol/ n = 4/dose 7–15 days DOPE nose SPQ: 5/8 showed CFTR function Hyde et al. (2000) DC- Repeat administration 3 DNA: 6/9 + ve after ≥ one dose Chol/ doses 400 μg DNA/nostril DOPE nose 1/9 + ve for all 3 mRNA: 7/9 + ve after ≥ one dose 1/9 + ve for all 3 protein: 6/9 + ve after ≥ one dose; 2– 15% epithelial cells transfected NPD: partial Cl− correction in individual patients SPQ: 5/9 showed CFTR function after ≥ one dose Bacterial adherence: no difference, but technical problems Immune responses: no response to CFTR Importantly, no loss of efficacy with repeated dosing Porteous et al. DOTA 400 μg DNA DNA: 7/8 + ve on days 3 and 7 (1997) P nose 2/7 + ve on day 28 mRNA: 2/8 + ve on days 3 and 7
- 11. 11 NPD: 2/8 partial Cl− correction up to 4 weeks SPQ: − ve Noone et al. (2000) EDM Dose escalation 0.4–4 mg DNA: all + ve (some cross- PC DNA placebo in contamination to placebo) nose contralateral nostril mRNA: − ve NPD: no change Zabner et al. (1997) GL67 1.25 mg DNA/nostril GL67/ DNA: 8/9 + ve vs. DNA to one nostril, pDNA to naked contralateral nostril pDNA nose pDNA to one nostril, empty RNA: − ve, technical problems plasmid to contralateral NPD: statistically significant correction of Cl− with both GL67 and naked pDNA. No difference between vectors Alton et al. (1999) GL67 Lung: 42.2 mg DNA Lung: lung and nose DNA: 8/8 + ve Nose: 11.8 mg DNA RNA: − ve PD: statistically significant Cl− correction in active group, 25% of normal values Lipid only SPQ: CFTR function in 5/6 patients Placebo Bacterial adherence: 5/6 patients in active group reduced bacterial binding compared to pre-treatment values (n = 16) Inflammation: significant reduction of inflammatory cells in sputum in active group similar results (DNA, mRNA, PD, SPQ, bacterial adherence ) in the nose Safety: 7/8 patients in active group developed flu-like symptoms (fever, headache), resolved within 36 h. 6/8 patients in both groups had mild airway symptoms. Ruiz et al. (2001) GL67 7.9–21.12 mg DNA mRNA: 4/8 + ve, 3/4 received highest lung dose Inflammatory response: 4/8 pronounced fever, myalgia within 6 h post- administration. Serum IL-6 increased, but no changes in IL-8, IL-1, TNF-α or IFN-γ. No antibodies to lipid or plasmid. (n = 2–4/dose) Lipid and DNA have synergistic effect on inflammation. Konstan et al. (2004) DNA Dose escalation 0.8–8.0 mg DNA: 12/12 + ve in active but cross- nanop DNA n = 2–6/dose contamination in placebo article contralateral nostril placebo
- 12. 12 s nose NPD: partial to complete Cl− correction 8/12, up to day 6 Safety: well tolerated, no adverse effects related to treatment Table # 1. From Griesenbach and Eric, 2008.