💕SONAM KUMAR💕Premium Call Girls Jaipur ↘️9257276172 ↙️One Night Stand With Lo...
LPR Laryngopharyngeal Reflux
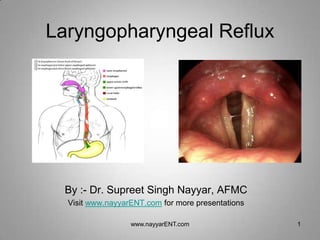
1. Laryngopharyngeal Reflux
By :- Dr. Supreet Singh Nayyar, AFMC
Visit www.nayyarENT.com for more presentations
www.nayyarENT.com 1
2. Introduction
• The term REFLUX comes from the Greek word meaning
“backflow,” usually referring to the contents of the
stomach
• AAOHNS adopted the terminology LPR- “Laryngopharyngeal
Reflux” in 2002
• GERD: an abnormal amount of reflux up through the
lower sphincters and into the esophagus.
• LPRD: when the reflux passes all the way through the
upper sphincter reaching the larynx and pharynx without
belching or vomiting
www.nayyarENT.com 2
3. Epidemiology
• Incidence 4%-10% in various studies
• No racial predilection
• Common in age > 40 yrs
• Upto 55%- with hoarseness *
• 75% - with subglottic stenosis
• 20%-45%-shows Heartburn, Regurgitation and
indigestion
* Koufman JA et al : Reflux Laryngitis and its sequela:the diagnostic role of ambulatory
24-hr pH monitoring. J Voice 2:78-79,1994
www.nayyarENT.com 3
4. Relevant anatomy and physiology
• Lower
– Various mechanisms
acts
– 3 cm in length
• Upper
– Cricopharyngeus + circular
muscle fibers of esophagus
– 3 cm in length
www.nayyarENT.com 4
5. Anti reflux barrier
• Oesophageal Acid Clearance
– Increased by peristalsis of oesophagus & salivary bicarbonate
– Decreased by abnormal oesophageal motility & xerostomia
– Oesophageal peristalsis
• Primary
• Secondary
• Oesophageal Epithelial Resistance
– Mucus : barrier to pepsin
– Cell membrane, intercellular bridge
– Metabolic buffering capacity of mucosa
www.nayyarENT.com 5
6. Cause of symptoms
• Retrograde reflux of gastric acid
• Damage to cilia from reflux contents - mucous stasis
• Gastroesophageal reflux - neurally mediated
chronic cough
• Defect in carbonic anhydrase iso enzyme III
• Deglutitive pharyngo laryngeal abnormalities
www.nayyarENT.com 6
20. Diagnosis
• Why is diagnosis of LPR often missed??
– Low index of suspicion
– Patients often don’t have heartburn (esophagitis)
– Variable / unrecognized findings
– Chronic intermittent nature of LPR leads to decreased
sensitivity of pH monitoring
– Inadequate duration &/or dosage of PPI
www.nayyarENT.com 20
29. Treatment
Antireflux therapy
• Phase I : Lifestyle-dietary modification
Antacid therapy
• Phase II : Prokinetic
H2-blockers, PPI
• Phase III : Antireflux surgery
www.nayyarENT.com 29
30. Lifestyle modifications
• Stop smoking
• Elevate the head of the bed on blocks(15-20cm)
• Reduce body weight
• Avoid tight-fitting clothing
• Avoid lying down after meals
www.nayyarENT.com 30
31. Dietary modification
• Avoid fat, caffeine, chocolate, mints,
carbonated drinks, fat, mints chocolate, milk
product, onion, cucumber
• Avoid alcohol
• Avoid overeating
• Avoid ingestion of food and drink 2 hours before
bed time
www.nayyarENT.com 31
32. Voice Therapy
Vocal Hygiene
-Reduce/eliminate throat clearing and
coughing.
-Encourage conservative voice use
-Initiate new functioning voicing
behaviors.
-Production of voice with an extreme
forward focus.
Resonant voice therapy (RVT): most often employed for
LPR/granulomas
www.nayyarENT.com 32
33. Voice therapy
• Developed by Verdolini & Lessac.
• Resonant Voice: involves oral vibratory sensations in the
context of easy phonation.
• Goal: “…to achieve the strongest, cleanest possible
voice with the least effort and impact between the vocal
folds to minimize the likelihood of injury and maximize
the likelihood of vocal health (Stemple et al., 2000)”.
• How? Pt. Is asked to monitor the “feel” and to
concentrate on auditory feedback
www.nayyarENT.com 33
35. Drug therapy
• Antisecretory
– H2 Blockers
• Ranitidine, Famotidine,
• Reversibly reduces acid secretion, not helps in healing
– PPI’s
• Near total acid suppression, promotes healing
• Omeprazole (20-40mg OD)
• Mucosal protective
– Sucralfate, alginic acid
www.nayyarENT.com 35
36. • Antacids
– Immediate relief of symptoms
– Reduces acidity
– Not helps in healing
– Antacid mixture
• Prokinetic
– Symptomatic relief, not helps in healing
– Increases gastric emptying
– Metoclopramide (5-10mg tds), Domperidone
(10-20mg tds)
www.nayyarENT.com 36
37. Evaluation and Management
of Laryngopharyngeal Reflux
Charles N. Ford, MD
JAMA. 2005;294:1534-1540. www.nayyarENT.com 37
38. Surgery
Laparoscopic Nissen Fundoplication
Indications
Failed drug treatment
Complications
Goal
Restore natural integrity of
LES & maintain normal
deglutition
www.nayyarENT.com 38
39. PAEDIATRIC LPR
• Incidence - 18% of all
infants
• 70% in TO fistula,
neurological diseases
• Children < 3y more
prone for reflux
www.nayyarENT.com 39
40. Natural history of reflux
• In majority it is self limited
• Improves by 1st yr of life others can be
benefited by positional treatment
• If persists after 3 yrs of age needs medical
or surgical treatment
www.nayyarENT.com 40
43. Treatment
• Similar as adult except
– Burping
– Positional management
– PPIs – lack of long term experience
– No surgical intervention before 3 years
www.nayyarENT.com 43
44. What’s new
• Pepsin detection in throat sputum by
immunoassay
– 100% sensitive & 89% specific
• Reflux laryngitis is associated with down-
regulation of mucin gene expression.
• Bifurcated, triple-sensor pH probe allows
identifying true hypopharyngeal reflux episodes
• Oropharyngeal aerosol-detecting pH probe
www.nayyarENT.com 44