3. The uterus has central position in the pelvis
The external Os is at the level of the ischial spine
It is ante verted & ante flexed
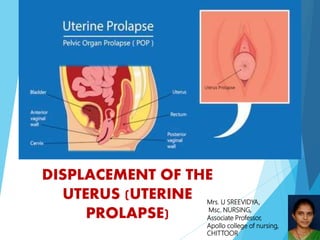
4. Prolapse of the uterus refers to the
downward displacement of the vagina
and uterus.
5. It is one of the common clinical condition met in day to day
gynecological practice
It is most often seen in multiparous women.
It is a form of herniation
Uterine prolapse can happen to women of any age, but it
affects post menopausal women who had one or more
vaginal deliveries.
The incidence of prolapse is about one in 250
pregnancies.
6. Uterine prolapse occurs when pelvic floor muscles and
ligaments stretch and weaken, providing inadequate support for
the uterus . The uterus then slips down into or protrudes out of
the vagina.
Weakening of the pelvic muscles that leads to uterine prolapse can
be caused by:
1) Damage to supportive tissue during pregnancy and child birth
2) Effects of gravity
3) Loss of oestrogen
8. Uterine prolapse means the uterus has
descended from its normal position in the
pelvis farther down into the vagina.
Uterine prolapse is a form of female genital
prolapse. It is also called pelvic organ
prolapse or prolapse of the uterus
(womb).
11. 1. Congenital – At birth
2.Acquired –
During Labour
1-Bearing down
2-Forceps delivery
3- Traction on cord
4- Breech extraction before fully
dilatation
12. During puerperium
Lack of exercises and
bodily weakness
Others: Repeated deliveries or
child birth
13. 1. Increase in intra - abdominal
pressure
Abdominal mass
Ascitis
Chronic cough,
constipation
2. Obesity
3. Uterine fibroid
14. 1. Uterovaginal prolapse:
It is the prolapse of uterus, Cx & upper vagina.
Commonest type
It is accompanied by Cystocele.
2. Congenital prolapse:
No cystocele
Often seen in nulliparous, so called as
nulliparous prolapse.
Cause-congenital weakness of supports of
Uterus.
22. 1.In first-degree prolapse- The uterus
descends down from its anatomical
position (external os at the level of
ischial spines) but the external os still
remains inside vagina.
2. In second-degree The external os
protrudes outside the vaginal introits
but the uterine body still remains
inside the vagina.
1
2
3
4
23.
24. 3. In third-degree prolapse or total prolapse or procidentia-
The uterine cervix and body descends to lie outside the
introitus. It is also known as Procidentia OR complete
prolapse.
4. In fourth degree or complex prolapse- Prolapse of the uterus
with eversion of entire vagina. It is inevitably associated with
cystocele and an enterocele.
25. Feeling of something coming
down per vaginum specially
while she is moving
Backache or Dragging pain in
the pelvis
Dysparenunia
26. Difficulty in passing urine, more
lessthe sternous effort
evacuation.
Incomplete evacuation
Urgency or frequency of
micturation
The woman
difficulty in
may experience
passing stools and
complete evacuation of bowels.
27. utero-vaginal prolapse may be visible during
inspection of the vulva.
In case of minor prolapse it may become visible on
straining.
Rectal examination also differentiate between
rectocele and enterocele.
28. Pelvic examination Both
dorsal & standing positions. The
patient is asked to strain , this helps
to demonstrate a prolapse which may
not be seen at rest
32. Adequate antenatal & intranatal care
To avoid injury to the supporting
structures during the time of vaginal
delivery
Adequate postnatal care
To encourage early ambulance
To encourage pelvic floor exercises
General measures
To avoid strenuous activities- heavy lifting
To avoid pregnancies too soon
33. Oestogen replacement therapy
Kegal exercise
Pessary treatment
A vaginal pessary is an object
inserted into the vagina to hold
the uterus in place.
34. Early cases of UV prolapse are helped by pelvic floor
exercises Particularly during puerperium and while
waiting to undergo surgical treatment.
Kegel exercises are used to tone up pelvic musculature
These exercises are done 3 times a day for 20 min each.
Kegal exercises
35.
36.
37. A mechanical device for correcting and controlling
UV prolapse
A pessary does not cure UV prolapse
It only holds the genital tract in position
Advised for patients who cannot undergo surgery
Types
1.Ring pessary
2.Hodge pessary
39. Management
Choice of pessary ( ring pessaries commonly used)
Select the Size (depends upon size of vagina)
Sterilize the pessary
Insertion- before insertion of the pessary, it is to be kept in
hot water for few minutes so that pessary become soft and
easy to insert
Follow up
pessary should be removed ,cleaned and reinserted at regular
intervals of 6-12 months.
40.
41. Surgery should wait until
symptoms are worse than
the risks of having
surgery. The surgical
approach depends on:
Degree of prolapse
Desire for future
pregnancies
Often, a vaginal
hysterectomy is used to
correct uterine prolapse.
42. Vaginal Hysterectomy – most common operation and its
indications are:
- Post-menopausal prolapse
-Uterine pathology like small fibroids or adenomyosis
-Menstrual disorders such as dysfunctional uterine bleeding
-Prolapse during childbearing age , after completion of
family
Burch Operation – for relief of symptoms of cystocele.
43. Anterior Colporrhaphy – for anterior vaginal wall
prolapse.
Posterior Colporrhaphy – for repair of the posterior
vaginal wall and perineum.
Manchester Repair (Fothergill’s Operation) – for repair of
uterovaginal prolapse. Carried out in women of child bearing
age and haven’t completed their families and insist on
preservation of uterus
44.
45. a)To assess the level of pain, cause, location, intensity to get base
line data
b)To provide comfortable position to the patient to relieve discomfort
i.e. lying down position
c)To provide diversion therapy to the patient to divert the mind of the
patient
d)To provide analgesics to patient as prescribed by physician to
relieve pain.
46. a) To assess the signs & symptoms of infection.
b) To assess the vital signs of the patient
c)To encourage the patient not to touch the
prolapsed area with unclean hands.
d) Provide prescribed antibiotics to patient
47. a) Explain all treatment and procedures
b) Encourage verbalization of feelings by patient
and family
c) Provide information on treatment modalities.
48. 1)Dutta D.C 'Textbook of obstetrics' 6th edition published
by new book agency (P) limited pp -312-313,421-422.
2)Jacob annamma ‘a comprehensive textbook of
midwifery ‘1st edition published by jitender p vij pp 539-
55
3) www.Google.com