
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Multiple Myeloma and Plasma cell Dyscrasias
Ähnlich wie Multiple Myeloma and Plasma cell Dyscrasias (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Multiple Myeloma and Plasma cell Dyscrasias
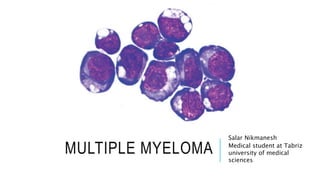
- 1. MULTIPLE MYELOMA Salar Nikmanesh Medical student at Tabriz university of medical sciences
- 2. WHAT IS MYELOMA? Multiple Myeloma (also known as Myeloma or Plasma Cell Myeloma) is a malignancy of plasma cells, which are the white blood cells responsible for the production of antibodies (proteins). MM is characterized by a proliferation of malignant plasma cells and a subsequent overabundance of monoclonal paraprotein (M protein). When plasma cells become cancerous and grow out of control, they can produce a tumor called a plasmacytoma. These tumors generally develop in a bone, but they are also rarely found in other tissues. If someone has only a single plasma cell tumor, the disease is called an isolated (or solitary) plasmacytoma. If someone has more than one plasmacytoma, they have multiple myeloma.
- 4. ETIOLOGY The precise etiology of MM has not yet been established. Roles have been suggested for a variety of factors, including genetic causes, environmental or occupational causes, MGUS, radiation, chronic inflammation, and infection. .Genetic .Environmental:agriculture, food, and petrochemical .MGUS-SMM .Radiation .Chronic inflammation .Infection:Human herpesvirus 8 (HH8) infection of bone marrow dendritic cells
- 5. PATHOPHYSIOLOGY AND CLINICAL PRESENTATION MM is characterized by neoplastic proliferation of plasma cells involving more than 10% of the bone marrow and overproduction of monoclonal immunoglobulin G (IgG), immunoglobulin A (IgA), and/or light chains, which may be identified with serum protein electrophoresis (SPEP) or urine protein electrophoresis (UPEP). The pathophysiologic basis for the clinical sequelae of MM involves the skeletal, hematologic, renal, and nervous systems.
- 6. 1.SKELETAL PROCESSES Plasma-cell proliferation causes extensive skeletal destruction with osteolytic lesions, anemia, and hypercalcemia. Destruction of bone and its replacement by tumor may lead to pain, spinal cord compression, and pathologic fracture. .Bone pain: Bone pain is the most common presenting symptom in MM. Most case series report that 70% of patients have bone pain at presentation. The lumbar spine is one of the most common sites of pain. .Spinal cord compression:The symptoms that should alert physicians to consider spinal cord compression are back pain, weakness, numbness, or dysesthesias in the extremities. . Hypercalcemia:Confusion, somnolence, bone pain, constipation, nausea, and thirst are the presenting symptoms of hypercalcemia.
- 8. 2.HEMATOLOGIC PROCESSES Bone marrow infiltration by plasma cells results in neutropenia, anemia, and thrombocytopenia. In terms of bleeding,a patient may come to medical attention for bleeding resulting from thrombocytopenia. Rarely, monoclonal protein may absorb clotting factors and lead to bleeding. .Anemia:Anemia, which may be quite severe, is the most common cause of weakness in patients with MM. .Hyperviscosity:This syndrome is infrequent in MM and occurs with IgG1, IgG3, or IgA. MM may involve sludging in the capillaries, which results in purpura, retinal hemorrhage, papilledema, coronary ischemia, or central nervous system (CNS) symptoms (eg, confusion, vertigo, seizure). .Cryoglobulinemia:causes Raynaud phenomenon, thrombosis, and gangrene in the extremities.
- 9. 3. RENAL PROCESSES The most common mechanisms of renal injury in MM are direct tubular injury, amyloidosis, or involvement by plasmacytoma.Renal conditions that may be observed include hypercalcemic nephropathy, hyperuricemia due to renal infiltration of plasma cells resulting in myeloma, light-chain nephropathy,amyloidosis,and glomerulosclerosis.
- 10. 3. RENAL PROCESSES Renal failure and insufficiency are seen in 25% of patients with MM,including the following manifestations: .Myeloma kidney syndrome with multiple etiologies .Amyloidosis with light chains .Nephrocalcinosis due to hypercalcemia
- 11. 4. NEUROLOGIC PROCESSES The nervous system may be involved as a result of radiculopathy and/or cord compression due to nerve compression and skeletal destruction (amyloid infiltration of nerves). Carpal tunnel syndrome is a common complication of myeloma. Meningitis (especially that resulting from pneumococcal or meningococcal infection) is more common in patients with MM. Some peripheral neuropathies have been attributed to MM. Long-term neurologic function is directly related to the rapidity of the diagnosis and the institution of appropriate therapy for MM.
- 12. 5. INFECTION Abnormal humoral immunity and leukopenia may lead to infection. Pneumococcal organisms are commonly involved, but shingles (ie, herpes zoster) and Haemophilus infections are also more common among patients with MM.
- 13. PHYSICAL EXAMINATION .On head, ears, eyes, nose, and throat (HEENT) examination, the eyes may show exudative macular detachment, retinal hemorrhage, or cotton-wool spots. Pallor from anemia may be present. Ecchymoses or purpura from thrombocytopenia may be evident. .Bony tenderness is not uncommon in MM. .Neurologic findings may include a sensory level change. .On evaluation of the abdomen, hepatosplenomegaly may be discovered. .Amyloidosis may develop in some patients with MM. The characteristic physical examination findings that suggest amyloidosis include the following: Shoulder pad sign Macroglossia Typical skin lesions
- 14. WORKUP .Blood Studies .Urine Collection .Electrophoresis and Immunofixation .Radiography .Magnetic Resonance Imaging .Positron Emission Tomography .Bone Scan .Aspiration and Biopsy .Histologic Findings .Cytogenetic Analysis
- 16. MGUS & SMM Risk factors for progression to MM are as follows: M protein concentration > 1.5 g/dL Non-IgG isotype An abnormal free light chain (FLC) ratio Risk factors for progression of SMM to MM include any of the following: M protein concentration > 3 g/dL Abnormal FLC ratio Bone marrow plasma cell concentration > 10%
- 17. STAGING
- 18. CHEMOTHERAPY In patients with symptomatic MM, chemotherapy is required. In asymptomatic patients with MM, treatment is delayed until disease clinically progresses or until serum or urine levels of M protein substantially increase. The first step before starting therapy in MM is to determine whether a patient is a candidate for an autologous stem cell transplant. Eligibility depends primarily on the patient’s age and comorbidities. Typically an age of 65 years is used as a cut-off point for transplant eligibility. Although a single drug may be used to treat multiple myeloma, more often different kinds of drugs are used in combination. For example: Melphalan and prednisone (MP), with or without thalidomide or bortezomib. Vincristine, doxorubicin (Adriamycin), and dexamethasone (called VAD)