Anatomy Of NECK.pptx
•Als PPTX, PDF herunterladen•
1 gefällt mir•221 views

Anatomy of neck is apt for Physiotherapy students or students of basic medical school.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Anatomy Of NECK.pptx
Ähnlich wie Anatomy Of NECK.pptx (20)
Mehr von sakshiupadhyay88
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Anatomy Of NECK.pptx
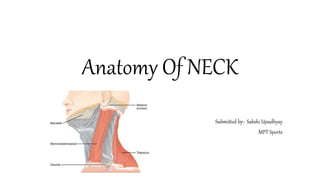
- 1. Anatomy Of NECK Submitted by:- Sakshi Upadhyay MPT Sports
- 2. Introduction • The neck is the bridge between the head and the rest of the body. It is located in between the mandible and the clavicle, connecting the head directly to the torso, and contains numerous vital structures. • Structures contained within the neck are responsible for breathing, speaking, swallowing, regulation of metabolism, support and connection of the brain and cervical spine, and circulatory and lymphatic inflow and outflow from the head.
- 3. Bone of the Neck • The skeleton of the neck is formed by the cervical vertebrae, hyoid bone, manubrium of the sternum, and clavicles. • These bones are parts of the axial skeleton except the clavicles, which are part of the appendicular skeleton.
- 4. Cervical Vertebrae • 7 cervical vertebrae form the cervical region of the vertebral column, which encloses the spinal cord and meninges.
- 5. Hyoid Bone (Hyoid) • Lies in the anterior part of the neck at the level of the C3 in the angle between the mandible and the thyroid cartilage. • Suspended by muscles that connect it to the mandible, styloid processes, thyroid cartilage, manubrium, and scapulae. • Does not articulate with any other bone.
- 6. • The hyoid consists of a body and greater and lesser horns and the lesser horn is the attachment for the stylohyoid ligament). • Functionally, the hyoid serves as an attachment for anterior neck muscles and a prop to keep the airway open.
- 7. Fascia of the Neck • Structures in the neck are surrounded by a layer of fascia but the two main divisions are superficial fascia and deep cervical fascia. The superficial cervical fascia extends from the head down to the thorax and axillae. In the neck, it contains the superficial lymph nodes, cutaneous nerves, external and anterior jugular veins, and the platysma muscle. It is arranged loosely to allow for neck movement.
- 8. The deep cervical fascia subdivides into the superficial layer of deep cervical fascia, the middle layer of deep cervical fascia, and the deep layer of deep layer of deep cervical fascia. • The superficial layer of deep cervical fascia, or investing layer, lies between the muscles of the neck and the superficial cervical fascia, encircling the sternocleidomastoid and trapezius muscles. It attaches inferiorly to the scapula, clavicle, and manubrium. Superiorly, it attaches to the mandible, mastoid process, superior nuchal line, and external occipital protuberance. • The middle layer of deep cervical fascia, or the pre tracheal layer, runs from the mediastinum inferiorly to the skull base superiorly. It has a muscular and visceral division. The muscular division encloses the strap muscles, sternohyoid, sternothyroid, omohyoid, and thyrohyoid muscles. The visceral division encloses the larynx, pharynx, esophagus, thyroid, parathyroid glands, trachea, and recurrent laryngeal nerve. • The deep layer of deep cervical fascia, or prevertebral layer, runs from the skull base to the mediastinum. Its two divisions are the alar and prevertebral layers. These layers surround the deep muscles of the neck and the cervical vertebrae, forming part of the retropharyngeal space.
- 9. Triangle of the Neck • The neck separates into two triangles: anterior and posterior, with these divided into additional triangles and anatomic areas. • The anterior triangle is surrounded inferiorly by the sternal notch and clavicle, laterally by the sternocleidomastoid, and medially by the trachea, thyroid, and cricoid cartilages. • The posterior triangle is bordered posteriorly by the trapezius muscle, anteriorly by the sternocleidomastoid muscle, and inferiorly by the clavicle.
- 11. Posterior triangle This is formed by : The Sternocleidomastoid muscle-anteriorly. The Trapezius muscle-posteriorly. The Clavicle-inferiorly. The apex of the triangle is formed by the occipital bone. The ROOF of the posterior triangle is formed by: Skin Superficial fascia Platysma Investing layer of the deep cervical fascia
- 12. • The FLOOR of the triangle is formed by the following muscles from above downwards: Splenius Capitis Levator scapulae Posterior scalene Middle scalene Anterior scalene
- 13. Subdivisions of the posterior triangle • The posterior triangle is further divided into two smaller triangles by the Inferior belly of the Omohyoid muscle . These are the Supraclavicular triangle and Occipital triangle. 1. Supraclavicular triangle - It is formed by the Inferior belly of the Omohyoid, the Clavicle and Sternocleidomastoid muscle. 2. The Occipital triangle is formed by the Inferior belly of the Omohyoid, the Trapezius muscle and Sternocleidomastoid muscle.
- 14. Nerves and Plexuses of the Posterior Triangle • Spinal accessory nerve • Branches of Cervical plexus • Roots and trunks of • brachial plexus
- 15. Muscles of the Posterior Triangle • Sternocleidomastoid • Splenius capitis • Levator scapulae • Scalenus medius • Scalenus anterior (may or may not be present) • Trapezius
- 16. Arteries of the Posterior Triangle • Subclavian (3rd part) • Superficial cervical & suprascapular (branches of thyrocervical trunk, a branch of 1st part of subclavian artery) • Occipital, a branch of external carotid artery
- 17. Veins of the Posterior Triangle
- 18. Anterior Triangle • BOUNDARIES: Anterior border of the SCM muscle Midline of the neck Inferior border of the mandible • ROOF: Skin Superfacial fascia and platysma muscle Investing layer of deep cervical fascia
- 19. SUBDIVISIONS OF ANTERIOR TRIANGLE • The anterior triangle is divided into four smaller triangles: SUBMENTAL TRIANGLE SUBMANDIBULAR TRIANGLE CAROTID TRIANGLE MUSCULAR TRIANGLE
- 20. 1.SUBMENTAL TRIANGLE formed by the : anterior midline of neck hyoid bone anterior belly of digastric muscle 2.SUBMANDIBULAR TRIANGLE formed by: Inferior border of the mandible Anterior belly of the digastric muscle Posterior belly of the digastric muscle 3.CAROTID TRIANGLE formed by : Superior belly of the Omohyoid muscle Sternocleidomastoid muscle Posterior belly of the digastric muscle 4.MUSCULAR TRIANGLE formed by : midline of the neck superior belly of the Omohyoid sternocleidomastoid muscle
- 21. Muscles of the Anterior Triangle • Suprahyoid muscles : (Digastric , Mylohyoid, Stylohyoid, Geniohyoid). These elevate the hyoid bone , and the floor of the mouth , and depress the mandible . • Infrahyoid muscles : (Sternohyoid, Sternothyroid, Thyrohyoid, Omohyoid). These depress the hyoid bone and the larynx.
- 22. Vessels and Nerve of the Anterior Triangle • VESSELS: carotid system(CCA,ICA, ECA) Internal Jugular vein • NERVES: Cranial nerves 7,9,10,11,12 Cervical plexus
- 23. Muscles of the Neck • Sternocleidomastoid • Scalene Muscles Anterior, Middle and Posterior • Masseter Muscle • Splenius Cervicis Muscle • Levator Scapulae Muscle • Trapezius Muscle
- 24. Sternocleidomastoid • Action Bilateral: Extends the head, assists in respiration when the head is fixed Unilateral: Tilts the head to the same side, rotates the head to the opposite side • Origin Sternal head: Manubrium Clavicular head: Medial third of the clavicle • Insertion Mastoid process and superior nuchal line • Innervation Accessory nerve and direct branches from the cervical plexus (C1-2)
- 25. Examine Sternocleidomastoid • Position of the patient is in Supine • Location: the mastoid process, medial • clavicle and the top of the sternum • Ask patient to raise his head very slightly off the table as you palpate SCM • Palpate along the borders of the SCM • Follow it behind the earlobe and then down to the clavicle and sternum.
- 26. Scalene muscles • Anterior scalene • Middle scalene • Posterior scalene • Actions of scalenes muscles Unilaterally: Laterally flex the head and neck to the same side, rotate head and neck to the opposite side Bilaterally: Elevate the ribs during inhalation, flex the head and neck
- 27. Anterior scalene • Origin TP of 3rd through 6th cervical vertebrae (ant. tubercle) • Insertion 1st rib • Innervation Cervical and brachial plexus (C3-6)
- 28. Middle scalene • Origin TP of 3rd through 7th cervical vertebrae (post. tubercle) • Insertion 1st rib • Innervation Cervical and brachial plexus (C3-6)
- 29. Posterior scalene • Origin TP of 5th through 7th cervical vertebrae (post. tubercle) • Insertion 2nd rib • Innervation Cervical and brachial plexus (C3-6)
- 30. Examine Scalenes • Position of the patient is in Supine • Cradle the head to allow for easier palpation • Place your finger pad along the ant. and lat. sides of the neck b/w SCM and trapezius.
- 31. Masseter • Position of the patient is in Supine • Location: zygomatic arch and angle of the mandible • Place your fingers b/w these bony landmarks and palpate the surface of the masseter • Ask pt. to alternately clench and relax her jaw
- 32. Splenius muscles • Action Entire muscle bilateral contraction extends the cervical spine and head, unilateral contraction flexes and rotates the head to the same side • Origin Splenius cervicis Spinous process of T3-T6 vertebrae Splenius capitis Spinous process of C3-T3 vertebrae • Insertion Splenius cervicis Transverse process of C1-2 Splenius capitis Lateral superior nuchal line, mastoid process • Innervation Lateral branches of dorsal rami of spinal nerves C1-6
- 33. Clinical Anatomy Torticollis • Torticollis, also known as wry neck, is a dystonic condition defined by an abnormal, asymmetrical head or neck position, which may be due to a variety of causes. • The term torticollis is derived from the Latin words tortus for twisted and collum for neck.
- 34. Signs and Symptoms • Torticollis can be a disorder in itself as well as a symptom in other conditions. • Other symptoms include: • Neck pain • Occasional formation of a mass • Thickened or tight sternocleidomastoid muscle • Tenderness on the cervical spine • Tremor in head • Unequal shoulder heights • Decreased neck movement
- 35. Torticollis may lead to additional problems : Flattening of the skull (plagiocephaly or brachycephaly) in infants. Movement that favors one side of the body, affecting the arms, trunk, and hips. This can lead to strength imbalances, such as an elevated shoulder and side- bending of the trunk. This movement pattern can lead to delayed gross motor development. Developmental hip dysplasia. Scoliosis. Limited ability to turn the head to see, hear, and interact with surroundings, which can lead to delayed cognitive development. Delayed body awareness or lack of self-awareness and interaction. Difficulty with balance. Asymmetrical vision changes.
- 36. Diagnosis • General History taking • Birth History • History of Trauma • Neurological examination • X-ray of cervical spine • MRI • USG - Muscular tissue, Colour Histogram • Optometrist evaluation
- 37. Assessment : • Observation of any asymmetries including facial, cranial, neck and positional preference and presence of plagiocephaly. • Observation of skin creases. • Observation of infant in developmentally appropriate positions to detect asymmetry and screen developmental milestones. • Cervical active and passive range of movement testing. • Upper and lower limb ROM screen, checking for hip dysplasia, which can be associated with CMT, and spine asymmetry. • Pain at rest and during movements. • Palpation of sternocleidomastoid for size and elasticity and presence of mass. • Screen of visual tracking. • Screen muscle tone. • Identification of Red flags and appropriate onward referral: 1. poor tracking 2. abnormal muscle tone 3. other features inconsistent with CMT 4. poor progress with treatment
- 38. Physiotherapy Management Goals • Improve child's ability to turn head between right and left sides • Improve child's ability to bring chin to chest • Improve child's ability to orient their head to midline against gravity • Encourage child to lift head against gravity while lying on stomach • Allow child to experience proper weight shifting during developmental activities including sitting, rolling, creeping and walking
- 39. Early mild cases Children with a mild degree of deformity reporting early for the treatment can be managed with physiotherapy. The physiotherapy procedures employed are: I. Evaluation: Careful evaluation of ROM and the degree of deformity. II. Massage: Massage can relax the muscle preceding the stretching maneuvers. III.Thermo Therapy Modality: Carefully administered thermo- therapy modality induces relaxation. IV.Passive movements: The child is placed in supine position with head beyond the edge of the table with the neck in extension by positioning a pillow under the thoracic region; Shoulders are stabilized by an assistant.
- 40. • To attain relaxation, all the movements of the cervical spine are done in a form of slow relaxed passive movements. • This should be followed by sustained passive stretching to the affected sternomastoid. E.g. when the right sternomastoid is involved the head should be gradually bent inside flexion to the left, held there for a while and then rotated gradually to the right. Try to gain as much overcorrection as possible by applying gradual traction to gain further stretching.
- 41. • Maintenance of Correction: Once the correction is achieved. It has to be maintained by passively holding or keeping a sandbag. E.g: Kineso taping, Cervical Brace, Cervical collars. • The same maneuver can be repeated during the subsequent visits. Active correction is best achieved by assisting the child head to follow an object moved in the proper arc of correction. The bright-colored sound producing object is ideal to attract the child attention. – PNF: patients with neck extension can be used to an advantage with emphasis on stretch and traction.
- 42. Post surgical PT management • Hot packs for pain relief. • Active movements of sternocleidomastoid to prevent post surgery weakness. • Free active movements in the direction of correction followed by resistive exercises. • Self correction in front of mirror. • Specially molded cervical collar and maintenance of correction during sleep.