Chronic renal failure (CRF)
•Als DOCX, PDF herunterladen•
5 gefällt mir•962 views

Chronic renal failure (CRF)

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Chronic renal failure (CRF)
Ähnlich wie Chronic renal failure (CRF) (20)
Mehr von ROMAN BAJRANG
Mehr von ROMAN BAJRANG (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Chronic renal failure (CRF)
- 1. RELIANCE INSTITUTE OF NURSING TOPIC PRESENTED BY :- MR. ROMAN BAJRANG BASIC BS.C NURSING 2ND YEAR RELIANCE INSTITUTE OF NURSING
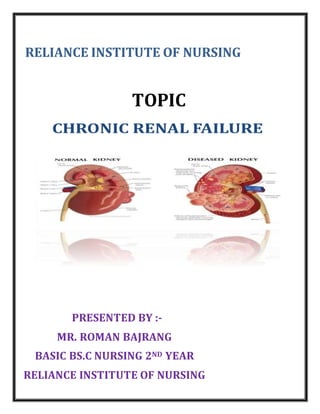
- 2. INTRODUCTION Chronic renal failure is a gradual and progressive loss of the ability of the kidneys to function normally. The change is irreversible and is due to loss of nephrons of the kidney. The nephrons are basic functioning unit of the kidney and there are normally about one million nephrons in each kidney. The kidney is no longer able to clean toxins & waste product from blood and concentrate the urine. When patients begin to experience symptoms of kidney failure, most of their kidney function is lost. Simply it can be interpreted as kidneys gradually stopping to working. Alternative Names Kidney failure - chronic; Renal failure - chronic; Chronic renal insufficiency; Chronic kidney failure; Chronic renal failure
- 3. DEFINITION:- Chronic kidney disease (CKD), also known as chronic renal disease, is a progressive loss of renal function over a period of months or years. The symptoms of worsening kidney function are unspecific, and might include feeling generally unwell and experiencing a reduced appetite. www.crfindia.com Chronic kidney disease (CKD), also known as chronic renal disease, is a progressive loss in renal function over a period of months or years. Wikipedia, the free encyclopedia When a patient has sustained enough kidney damage to require renal replacement therapy on permanent basis, the patient has moved into the fifth or final stage CKD (Chronic Kidney Disease) also referred to as Chronic Renal Failure (CRF) or ESRD. Brunner & Suddarth
- 4. STAGES All individuals with a Glomerular filtration rate (GFR) <60 mL/min/1.73 m2 for 3 months are classified as having chronic kidney disease, irrespective of the presence or absence of kidney damage. Patients with kidney damage are at increased risk of the two major outcomes of chronic kidney disease: loss of kidney function and development of cardiovascular disease.[1] Stage 1 Slightly diminished function kidney damage with normal or relatively high GFR (≥90 mL/min/1.73 m2). Kidney damage is defined as pathological abnormalities or markers of damage, including abnormalities in blood or urine test or imaging studies.[1] Stage 2 Mild reduction in GFR (60–89 mL/min/1.73 m2) with kidney damage. Kidney damage is defined as pathological abnormalities or markers of damage, including abnormalities in blood or urine test or imaging studies.[1] Stage 3 Moderate reduction in GFR (30–59 mL/min/1.73 m2).[1] British guidelines distinguish between stage 3A (GFR 45–59) and stage 3B (GFR 30–44) for purposes ofscreening and referral.[4] Stage 4 Severe reduction in GFR (15–29 mL/min/1.73 m2)[1] Preparation for renal replacement therapy Stage 5 Established kidney failure (GFR <15 mL/min/1.73 m2, permanent renal replacement therapy (RRT),[1] or end stage renal disease (ESRD)
- 5. ETIOLOGY Diabetes mellitus 28% Hypertension 25 % Glomerulonephritis 21% Polycystic kidney disease 4% Others 23% – obstruction, infection etc. Many other diseases and conditions can damage the kidneys, including: Autoimmune disorders (such as systemic lupus erythematosus and scleroderma) Birth defects of the kidneys (such as polycystic kidney disease) Certain toxic chemicals Glomerulonephritis Injury or trauma Kidney stones and infection Problems with the arteries leading to or inside the kidneys Some pain medications and other drugs (such as cancer drugs) Reflux nephropathy (in which the kidneys are damaged by the backward flow of urine into the kidneys) Other kidney diseases Chronic kidney disease leads to a buildup of fluid and waste products in the body. This condition affects most bodysystems and functions, including: Blood pressure control Red blood cell production Vitamin D and bone health
- 6. PATHOPYSIOLOGY:- Due to etiological factors Renal function declines Accumulation of urea, creatinine & other waste products uremia decreased GFR upto 50% increased creatinine increasedGlomerular capillary pressure leads damages ofcapillaries focal& segmental glomerulosclerosisglobal glomerulosclerosis different stages ofChronic renal Diseases
- 7. CLINICAL MANIFESTSTION:- Neurologic Weakness and fatigue, confusion, inability to concentrate, disorientation, Tremors, seizures, asterixis, restlessness of legs, burning of soles of feet, behavior changes. Integumentary Gray-bronze skin color; dry, flaky skin; pruritus; ecchymosis; purpura; thin, brittle nails; coarse, thinning hair Cardiovascular Hypertension; pitting edema (feet, hands, sacrum); periorbital edema; pericardial friction rub; engorged neck veins; pericarditis; pericardial effusion; pericardial tamponade; hyperkalemia; hyperlipidemia Pulmonary Crackles; thick, tenacious sputum; depressed cough reflex; pleuritic pain; shortness of breath; tachypnea; Kussmaul-type respirations; uremic pneumonitis; “uremic lung” Gastrointestinal Ammonia odor to breath (“uremic fetor”); metallic taste; mouth ulcerations and bleeding; anorexia, nausea, and vomiting; hiccups; constipation or diarrhea; bleeding from gastrointestinal tract. Hematologic Anemia; thrombocytopenia Reproductive Amenorrhea; testicular atrophy; infertility; decreased libido Musculoskeletal Muscle cramps;loss of muscle strength; renal osteodystrophy;bone pain; bone fractures; foot drop
- 8. Electrolyte imbalance Electrolyte balance may be upset by impaired excretion and utilization. The salt wasting properties of some failing kidney in addition to vomiting and diarrhea may cause hyponatremia because of dilutional effect of water retention. Because the kidney are very efficient potassium excretors, however hyperkalemia occur late in disease because of catabolism, potassium containing medication, trauma, blood transfusion and acidosis contribute to potassium excess. Hypocalamia and hyperphosphatemia occur. Metabolic changes:- In advancing renal failure BUN and serum creatinine level rise as waste product of protein metabolism accompanying renal disease and inadequate dietary intake of protein often cause hypoproteinemia. Immunological change:- Impairment of the immunologic system makes the client very susceptible to infection.
- 9. DIAGNOSTIC FINDING Physical examination : - High blood pressure is almost always present during all stages of chronic kidney disease. A nervous system exam may show signs of nerve damage. Abnormal heart or lung sounds when listening with a stethoscope. A urinalysis may show protein or other changes. These changes may appear 6 months to 10or more years before symptoms appear. Tests that check how well the kidneys are working include: Creatinine clearance Creatinine levels BUN Chronic kidney disease changes the results of several other tests. Every patient needs tohave the following checked regularly, as often as every 2 - 3 months when kidney disease gets worse: Albumin Calcium Cholesterol Complete blood count (CBC) Electrolytes Magnesium Phosphorous Potassium Sodium Causes of chronic kidney disease may beseen on: Abdominal CT scan Abdominal MRI Abdominal ultrasound Kidney biopsy Kidney scan
- 10. This disease may also change the results of the following tests: Erythropoietin PTH Bone density test Vitamin D GLOMERULAR FILTRATION RATE Decreased GFR can be detected by obtaining a 24-hour urinalysis for creatinine clearance. As Glomerular filtration decreases (due to nonfunctioning glomeruli), the creatinine clearance value decreases, whereas the serum creatinine and BUN levels increase. ACIDOSIS With advanced renal disease, metabolic acidosis occurs becausethe kidney cannot excrete increased loads of acid. Decreased acid secretion primarily results from inability of the kidney tubules to excrete ammonia (NH3−) and to reabsorb sodium bicarbonate (HCO3−). There is also decreased excretion of phosphates and other organic acids. ANEMIA Anemia develops as a result of inadequate erythropoietin production, the shortened life span of RBCs, nutritional deficiencies and the patient’s tendency to bleed, particularly from the G.I- tract. kidney cannot excrete increased loads of acid. CALCIUM AND PHOSPHORUS IMBALANCE With decreased filtration through the glomerulus of the kidney, there is an increase in the serum phosphate level and a reciprocal or corresponding decrease in the serum calcium level. The decreased serum calcium level causes increased secretion of parathormone from the parathyroid glands. Other Tests The Cockcroft-Gault formula for estimating CrCl should be used routinely as a simple means to provide a reliable approximation of residual renal function in all patients with chronic kidney disease. The formulas are as follows:
- 11. CrCl (male) = ([140-age] X weight in kg)/(serum creatinine X 72) CrCl (female) = CrCl (male) X 0.85 MANAGEMENT :- Medical :- The goal of management is to maintain kidney function and homeostasis for as long as possible. OTHERTREATMENTSMAY INCLUDE: Special medicines called phosphate binders,to help prevent phosphorous levels from becoming too high Treatment for anemia, such as extra iron in the diet, iron pills,iron through a vein (intravenous iron) special shots of a medicine called erythropoietin, and blood transfusions Antacids Hyperphosphatemia and hypocalcemia are treated with aluminum-based antacids that bind dietary phosphorus in the GI tract. Both calcium carbonate and phosphorus binding antacids must be administered with food to be effective. Magnesium-based antacids must be avoided to prevent magnesium toxicity. Anti-hypertensive and Cardiovascular Agents. Hypertension is managed by intravascular volume control and a variety of antihypertensive Agents. Heart failure and pulmonary edema may also require treatment with fluid restriction, low- sodium diets, and diuretic agents, inotropic agents such as digitalis or dobutamine, and dialysis. The metabolic acidosis of chronic renal failure usually Produces no symptoms and requires no treatment; however, sodium bicarbonate supplements or dialysis may be needed to correct the acidosis if it causes symptoms
- 12. Anti-seizure Agents Neurologic abnormalities may occur, so the patient must be observed for early evidence of slight twitching, headache, delirium, or seizure activity. Intravenous diazepam (Valium) or phenytoin (Dilantin) is usually administered to control seizures. The side rails of the bed Should be padded to protect the patient. Erythropoietin Anemia associated with chronic renal failure is treated with recombinant human erythropoietin (Epogen). Anemic patients (hematocrit less than 30%) present with nonspecific symptoms, such as malaise, general fatigability, and decreased activity tolerance. Epogen therapy is initiated to achieve a hematocrit of 33% to 38%, which generally alleviates the symptoms of anemia. Epogen is administered either intravenously or subcutaneously 3 times a week. It may take 2 to 6 weeks for the hematocrit to rise; therefore, Epogen is not indicated for patients who need immediate correction of severe anemia. Blood volume expander Dopamine administer in low doses byintravenous infusion, increase renal blood flow. Diuretics If restoration of renal blood flow does not improved urinary output, a potent loop diuretic suchas furosemide (lasix) or an osmotic diuretic such as mannitol may be given with intravenous fluids. DIALYSIS :- In dialysis, blood is separated from a dialysis solution (dialysate) by a semipermeable membrane. Each type of dialysis may be used to relieve symptom of renal failure temporarily until the client regain kidney function or to sustain life in the client with the irreversible kidney disease. In the letter case, the dialysis must continue for the rest of the client’s life unless successful kidney transplantation is done. Dialysis is usually accomplished through both ultra filtration and diffusion. When
- 13. dialysis is used as a substitute for kidney function, the semi permeable membrane used is either the peritoneal membrane (for peritoneal dialysis) or an artificial membrane (for Hemodialysis). A specially prepared electrolyte solution called dialysate is placed in a compartment on one side of the membrane while the clients’ blood is on the other side. There are two types of dialysis: 1. Hemodialysis;a procedurein which blood passes through a semi permeable membrane filter outside the body. 2. Peritoneal dialysis;which uses the peritoneum surrounding the abdominal cavity. TYPES OF PERITONEAL DIALYSIS:- There are three types of peritoneal dialysis- a) Continuous ambulatory peritoneal dialysis. (CAPD) b) Continuous cycle peritoneal dialysis. (CCPD) c) Intermittent peritoneal dialysis. (IPD) SURGICAL MANAGEMENT:- Kidney transplantation is a surgical management of CRF. It is the surgical implantation of a human kidney from one person to another, is performed for client with irreversible kidney failure. Appendix presents a sample clinical pathway for client undergoing kidney transplantation. Selection of the transplant recipient is based on careful evaluation the client’s medical, immunologic, psychological and social statuses. The decision is usually made by the client. Significant others, and physician working together. Recipient selection is usually from the group less than 70 years of age who have an estimated life expectancy of 2 years or more and in whom the transplant will improve the quality of life. The transplant kidney surgically placed extra peritoneal the iliac fossa. The renal artery is anastmosed to the recipient’s hypogastric artery and the renal vein to the
- 14. recipient’s iliac vein. Usually the kidney begins to function immediately. Sometime adequate functioning is delayed a few days. Hemodialysis may be performed until good function is established. NUTRITIONAL THERAPY When patient have chronic kidney disease, he need to make changes in his diet, including: Limiting fluids Eating a low-protein diet (this may be recommended) ing salt, , and other electrolytes Getting enough calories CARBOHYDRATES If pt is overweight or have diabetes, he may need to limit the amount of carbohydrates. Fruits, breads, grains, and vegetables. These foods provide energy, as well as fiber, minerals, and vitamins. High-calorie desserts such as candies, sugar, honey, and jelly pies, cakes, or cookies FATS Fats can be a good source of calories. Make sure to use monounsaturated and polyunsaturated fats (olive oil, canola oil, safflower oil) to help protect your arteries PROTEIN Low-protein diets may be helpful before patient starts dialysis. He should take moderate- protein diet (1 gram of protein per kilogram of body weight per day). Once patient starts dialysis, he will need to eat more protein. In fact, a high- protein diet with fish, poultry, pork, or eggs at every meal may be recommended. This will help to replace muscles and other tissues that he lose. People on dialysis should eat 8 - 10 ounces of high-protein foods each
- 15. Top 15 Healthy Foods for People with Kidney Disease 1. Red bell peppers 9. Raspberries 10. Strawberries CALCIUM AND PHOSPHOROUS Calcium and phosphorous, two other important minerals in the body, are also monitored closely. Patient will need to limit the amount of dairy foods, because they contain large amounts of phosphorous. This includes milk, yogurt, cheese, tub margarine, butter, cream cheese, heavy cream, ricotta cheese, brie cheese, sherbet, and nondairy whipped toppings. Fruits and vegetables contain only small amounts of phosphorous, but may contain large amounts of potassium. Patient may need to take calcium supplements to prevent bone disease, and vitamin D to control the balance of calcium and phosphorous in his body. SALT OR SODIUM Reducing sodium in diet helps control high blood pressure, keeps from being thirsty, and prevents body from holding onto extra fluid IRON Patients with advanced kidney failure also have anemia and usually need extra iron. Many foods contain extra iron (liver, beef, pork, chicken, lima and kidney beans, iron-fortified cereals). 2. Cabbage 7. Cranberries 8. Blueberries 11. Cherries 12. Red grapes 13. Egg whites 14. Olive oil 3. Apples 4. Cauliflower 5. Garlic 6. Onions
- 16. Possible Complications Anemia Bleeding from the stomachor intestines Bone, joint, and muscle pain Changes in blood sugar Damage to nerves of the legs and arms (peripheral neuropathy) Dementia Fluid buildup around the lungs (pleural effusion) Heart and blood vessel complications o Congestive heart failure o Coronary artery disease o High blood pressure o Pericarditis o Stroke High phosphorous levels High potassium levels Hyperparathyroidism Increased risk of infections Liver damage or failure Malnutrition Miscarriages and infertility Seizures Swelling (edema) Weakening of the bones and increased risk of fractures PREVENTION Treating the condition that is causing the problem may help prevent or delay chronic kidney disease. Other tips for protecting the kidneys and preventing heart disease and stroke: Do not smoke. Eat meals that are low in fat and cholesterol. Get regular exercise (talk to your doctor or nurse before starting to
- 17. exercise). Take drugs to lower your cholesterol, if needed. Keep your blood sugar under control. Avoid eating too much salt or potassium. Always talk to your kidney doctor before taking any over-the- counter medicine, vitamin, or herbal supplement. Make sure all of the doctors you visit know you have chronic kidney disease. Everyone with chronic kidney disease should be up-to-date on important vaccinations, including: H1N1 (swine flu) vaccine Hepatitis A vaccine Hepatitis B vaccine Influenza vaccine Pneumococcal polysaccharide vaccine (PPV) Nursing Management The patient with chronic renal failure requires astute nursing care to avoid the complications of reduced renal function and the stresses and anxieties of dealing with a life-threatening illness. Examples of potential nursing diagnoses for these patients include the following: o Excess fluid volume related to decreased urine output, dietary excesses, and retention of sodium and water o Imbalanced nutrition: less than bodyrequirements related to anorexia, nausea and vomiting, dietary restrictions, and altered oral mucous membranes o Deficient knowledge regarding condition and treatment regimen o Activity intolerance related to fatigue, anemia, retention of waste products, and dialysis procedure o Low self-esteem related to dependency, role changes, changes in bodyimage, and sexual dysfunction.
- 18. SUMMARY:- Chronic Kidney Disease (CKD), also known as Chronic Renal Disease, orESRD, is a progressive, irreversible deterioration in renal function in which the body’s ability to maintain metabolic and fluid and electrolyte balance fails, resulting in uremia or azotemia (retention of urea and other nitrogenous wastes in the blood).
- 19. BIBLIOGRAPHY 1. Brunner and Suddharth’s, Medical Surgical Nursing, Volume -1,11th edition, page no: 1762. 2. Joyce .m. black, Medical Surgical Nursing, Volume-1, 7th edition , page no:714 3. Lewis Medical Surgical Nursing, 4th edition, Mosby publication, page no: 94. 4. Phipps Medical Surgical, 8th edition, Mosby publication, page no: 256-258. 5. Website: http://www.wikipedia.com/tss. Website