
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Ähnlich wie Diseases of the breast
Ähnlich wie Diseases of the breast (20)
Mehr von raj kumar
Mehr von raj kumar (20)
Diseases of the breast
- 3. LYMPHATIC DRAINAGE AXILLARY (MOSTLY) INTERNAL MAMMARY SUPRACLAVICULAR www.freelivedoctor.com
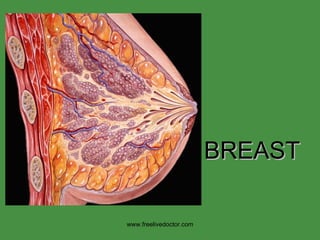
- 13. The most important thing to understand breast pathology is to get a solid IMAGE of the “NORMAL” breast lobule----ACINI, STROMA, BOUNDARIES www.freelivedoctor.com
- 16. ACCESSORY (axillary) BREAST TISSUE www.freelivedoctor.com
- 17. 1) CONGENITAL 2) ACQUIRED: CARCINOMA 3) ACQUIRED: PIERCING www.freelivedoctor.com
- 23. www.freelivedoctor.com Intraductal and periductal inflammatory cells, mostly neutrophils in acute mastitis.
- 24. www.freelivedoctor.com Pap smear of nipple exudate in acute mastitis. What are most of these cells?
- 25. INFLAMMATION? Peau d’orange www.freelivedoctor.com
- 26. www.freelivedoctor.com The tumor cells are INSIDE the skin dermal lymphatic spaces.
- 29. Ductesia CYSTS www.freelivedoctor.com
- 30. CUBOIDAL COLUMNAR RED COLUMNAR i.e. “APOCRINE” www.freelivedoctor.com
- 33. LYMPHOYCYTIC MASTITIS (DIABETIC MASTOPATHY ) www.freelivedoctor.com
- 39. www.freelivedoctor.com Breast cyst, filled with fluid, in the ultrasound lab.
- 40. CYST, GROSS CYST, MICROSCOPIC www.freelivedoctor.com
- 42. FIBROSIS + CYSTS = FIBROCYSTIC DISEASE www.freelivedoctor.com
- 45. “ SCLEROSING” ADENOSIS www.freelivedoctor.com
- 46. “ COMPLEX” SCLEROSING ADENOSIS (RADIAL SCAR) www.freelivedoctor.com
- 48. 1) EXTREMELY WELL DEFINED 2) YOUNGER WOMEN 3) ALWAYS BENIGN 4) CAN FIBROSE OR CALCIFY WITH AGE www.freelivedoctor.com FIBROADENOMA:
- 54. NORMAL DUCT NORMAL ACINUS ATYPICAL HYPERPLASIA of DUCT ATYPICAL HYPERPLASIA, LOBULE www.freelivedoctor.com
- 58. DCIS, microcalcifications www.freelivedoctor.com Microcalcifications, seen on mammograms, are often the result of necrotic intraductal crud which has calcified.
- 59. DCIS, microcalcifications www.freelivedoctor.com
- 61. www.freelivedoctor.com A whole lobule filled with monotono0us cells of the same type can be called LCIS, or lobular carcinoma in situ.
- 67. www.freelivedoctor.com Total Cancers Per Cent In Situ Carcinoma 15–30 Ductal carcinoma in situ, DCIS 80 Lobular carcinoma in situ, LCIS 20 Invasive Carcinoma 70–85 No special type carcinoma ("ductal") 79 Lobular carcinoma 10 Tubular/cribriform carcinoma (Better prognosis than average) 6 Mucinous (colloid) carcinoma (Better prognosis than average) 2 Medullary carcinoma (Better prognosis than average) 2 Papillary carcinoma 1 Metaplastic carcinoma, (Squamous)
- 70. INFILTRATING LOBULAR CA.,INDIAN” FILE PATTERN www.freelivedoctor.com
- 71. INFILTRATING DUCTAL CA., “TUBULAR” PATTERN or TYPE www.freelivedoctor.com
- 72. INFILTRATING DUCTAL CA., MUCINOUS (COLLOID) PATTERN or TYPE www.freelivedoctor.com
- 73. INFILTRATING DUCTAL CA., MEDULLARY PATTERN or TYPE www.freelivedoctor.com
- 77. GYNECOMASTIA (NO lobules) www.freelivedoctor.com
Hinweis der Redaktion
- Know the 2 major arteries (lateral and internal thoracic) and three lymph node groups which supply the breast.
- Know the 2 major arteries (lateral and internal thoracic) and three lymph node groups (axillary, internal thoracic (mammary) and supraclavicular) which supply the breast.
- Confusion between lobe, lobule, acini, alveolus, and duct is rampant in clinical medicine, but should never be confusing for you.
- Ther are an average of about 10 LOBES per breast. The suspensory ligament separates lobes.
- A lobule is part of a lobe composed of many acini. Lobules are separated from each other by bands of connective tissue.
- Acini are also known as alveoli.
- Active
- Pregnancy/Lactation
- Atrophic, i.e., post menopausal
- Breast tissue that is ~90% glandular and/or looks like “thyoid”, i.e., filled with milk, are lactating breasts
- Breast tissue ALWAYS extends to the axilla, and when it does form an actual protuberance, it can be called an accessory breast. Breasts are modified apocrine sweat glands embryologically.
- Nipple retraction can be congenital or acquired, when acquired, it represents suspicion for underlying fibrosis due to neoplasm or inpflammation.
- Macromastia.
- Atrophy is a NORMAL feature of postmenopausal breasts (estrogen withdrawal).
- Stroma>>>>>glands in atrophy, but lobules and acini are still present architecturally.
- All 4 of the classical signs of inflammation, heat redness, swelling, pain. What the the fifth?
- Intraductal and periductal inflammatory cells, mostly neutrophils in acute mastitis.
- Pap smear of nipple exudate in acute mastitis. What are most of these cells?
- Inflammatory carcinoma with its classic peau d’orange appearance.
- The tumor cells are INSIDE the skin dermal lymphatic spaces.
- Most of the inflammation here is PERI- ductal rather than INTRA- ductal. Acute or chronic? Why? Ans: Lymphocytes.
- Ductesia means dilated ducts.
- Dilated ducts are the same as cysts.
- Classic cheesy appearance of fat in fat necrosis. Fat necrosis is usually due to mechanical trauma, surgical or otherwise.
- Giant cells and hemosiderin are usually easily found in fat necrosis.
- What is the principal inflammatory cell here? Ans: Lymphocyte.
- The appearance is 100% exemplary of the diagnosis.
- “ Fibrocystic disease” is the waste basket term for benign breast disease characterized by fibrosis, cysts, inflammation, and a host of other benign changes. Certain features such as hyperplasia and papillomatosis, put it in a somewhat higher risk category for future carcinoma.
- Breast cyst, filled with fluid, in the pathology lab.
- Breast cyst, filled with fluid, in the ultrasound lab.
- This image speaks for itself.
- Adenosis is defined as an increased number of acini per lobule.
- Hence the name, “fibrocystic” disease.
- “ Benign” hyperplasia is characterized by, NO necrosis, the presence of MYOEPITHELIAL cells, and NO ATYPIA.
- Sclerosing adenosis is often confused with malignancy. Why? Ans: the “sclerosis” can be mistaken for desmoplasia.
- VERy very very scary, but 100% benign, lesion.
- Note the myoepithelial cell. The presence of myoepithelial cells, means, BENIGN!!!
- Our old friend the papillopma, i.e., a fingerlike proliferation of epithelium, growing over a fibrovascular core.
- Number 1 commandment in pathology: NEVER diagnosis a malignant papilloma on a frozen section!!!!! NEVER.
- The asterisked items, are more suspicious than the non-asterisked items. Intraductal NECROSIS is the most suspicious feature of all.
- Note the INTRADUCTAL NECROSIS.
- Note the atypia, “swiss cheese” hyperplasia, and early necrosis.
- Note the extreme artypia.
- Microcalcifications, seen on mammograms, are often the result of necrotic intraductal crud which has calcified.
- This type of calcification represents about a 20% chance of malignancy and should be biopsied. This device helps pathologists to sample the areas of greatest concern more heavily.
- A whole lobule filled with monotono0us cells of the same type can be called LCIS, or lobular carcinoma in situ.
- A whole lobule filled with monotono0us cells of the same type can be called LCIS, or lobular carcinoma in situ.
- HER2 is a proto-oncogene located at the long arm of human chromosome 17(17q11.2-q12). Approximately 25-30 percent of breast cancers have an amplification of the HER2/neu gene or overexpression of its protein product. Overexpression of this receptor in breast cancer is associated with increased disease recurrence and worse prognosis. Because of its prognostic role as well as its ability to predict response to trastuzumab , breast tumors are routinely checked for overexpression of HER2/neu. Overexpression also occurs in other cancer such as ovarian cancer and stomach cancer.
- 90% of infiltrating breast carcinomas are simply called “Infiltrating Ductal Carcinoma” on the pathology report.
- The “tubular” pattern is somewhat better in behavior.
- The mucinous variant is also somewhat better in behavior.
- The medullary variant (i.e., lots of immune calls or lymphocytes) is also somewhat better in behavior.
- Note that no matter how big a male’s breasts may get, they should never for m lobules, but just end as blunt ducts.