Mumps & Rubella.pptx
•Als PPTX, PDF herunterladen•
0 gefällt mir•45 views

infectious epidemiology

Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie Mumps & Rubella.pptx
Ähnlich wie Mumps & Rubella.pptx (20)
Mehr von Rahul Netragaonkar
Mehr von Rahul Netragaonkar (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Mumps & Rubella.pptx
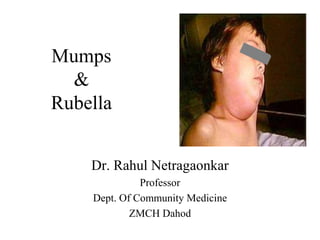
- 1. Mumps & Rubella Dr. Rahul Netragaonkar Professor Dept. Of Community Medicine ZMCH Dahod
- 2. • Mumbling Speech - Mumps : • Name "mumps" comes from "lump" or "mumble."
- 3. Mumps • Acute viral illness • Parotitis and orchitis described by Hippocrates in 5th century BC • Viral etiology described by Johnson and Goodpasture in 1934 • Frequent cause of outbreaks among military personnel in pre vaccine era
- 4. MUMPS • Acute infectious disease due to “myxovirus parotiditis” ; RNA paramyxovirus (Genus Rubulavirus) affecting mainly glands and nervous system • Clinically the disease is recognized by enlargement of one or both parotid glands with tenderness. • Worldwide distribution. • Morbidity is high. Mortality is less.
- 5. Mumps Epidemiology • Reservoir Human Asymptomatic infections may transmit • Transmission Respiratory drop nuclei • Temporal pattern Peak in late winter and spring • Communicability Three days before to four days after onset of active disease
- 6. MUMPS • AGENT FACTORS: • A)Agent: Myxovirus parotiditis is a RNA virus of the myxovirus family. The virus can be grown in chick embryo or tissue culture. There is only one serotype.
- 7. Mumps Virus • Paramyxovirus • RNA virus • One antigenic type • Rapidly inactivated by chemical agents, heat, and ultraviolet light
- 8. MUMPS • The virus can be • A)Isolated from the saliva or from swabs taken from the surface of STENSON’S DUCT. • Virus has also been found in the blood, urine, human milk, and in the CSF. • A) PERIOD OF COMMUNICABILITY: • Usually 4-6 days before the onset of symptoms and a week thereafter. The period of maximum infectivity is just before and at the onset of parotitis.
- 9. • SOURCE OF INFECTION: Both clinical and sub clinical cases. • Sub clinical cases accounts for 30-40% of all cases.
- 10. MUMPS • A) SECONDARY ATTACK RATE: • Estimated to be about 86%
- 11. HOST FACTORS • a)AGE AND SEX: Mumps is the most frequent cause of parotitis in children in the age group of 5-15 years. The average age of incidence of mumps is higher than with measles, chicken pox or whooping cough.
- 12. MUMPS • MODE OF TRANSMISSION:The disease is spread mainly by droplet infection and after direct contact with an infected person. • INCUBATION PERIOD; Varies from 2-3 weeks usually 18 days. • CLINICAL FEATURES:30-40% of cases are sub clinical characterized by pain and swelling in either one or both parotid glands and involves the sublingual submandibular glands.
- 13. Mumps Pathogenesis • Respiratory transmission of virus • Replication in nasopharynx and regional lymph nodes • Viremia 12-25 days after exposure with spread to tissues • Multiple tissues infected during viremia
- 14. Mumps Clinical Features • Incubation period 14- 18 days • Nonspecific prodromal phase of myalgia, malaise, headache, low-grade fever • Parotitis in 30%-40% • Up to 20% of infections asymptomatic
- 15. Mumps Clinical Case Definition • Acute onset of unilateral or bilateral tender, self-limiting swelling of the parotid or other salivary gland lasting more than 2 days without other apparent cause
- 16. MUMPS The disease tends to be more severe in adults than in children. IMMUNITY: One attack clinical or sub clinical will induce life long immunity. ost infants < 6 months of age are immune because of maternal antibodies. • ENVIRONMENTAL FACTORS: • Mumps is largely an endemic disease. Cases occur throughout the year – but peak incidence in wintertime of the year – but peak incidence in winter and spring. Over crowding linked to epidemics
- 17. 17 Complications of Mumps Frequent but not serious: • Orchitis (25-40%): 7-10 days after parotitis,with high fever (Unilateral in 75% orchitis cases, Most common extra-salivary gland manifestation in adults) • Epididymitis • Pancreatitis (4%) • Mild form of meningitis • Thyroiditis, Neuritis, Hepatitis,Ovaritis, • Oophoritis (5% adult women) • Spontaneous abortion(25% in pregnancy) Rare: Hearing loss, Polyarthritis, Encephalitis, Cerebellar ataxia
- 18. • Mumps infection in post-pubertal males can result in swelling of the testicles in 22-30% of affected individuals. • Such swelling may then lead to marked atrophy (shrinkage) of the testicle with poor sperm production as the result.
- 19. Mumps Laboratory Diagnosis • Isolation of mumps virus • Detection of mumps antigen by PCR • Serologic testing – positive IgM antibody – significant increase in IgG antibody between acute and convalescent specimens
- 20. MUMPS • PREVENTION: VACCINE: • Recommended for children over one year of age. • Its use may be considered in susceptible adults, especially males. • Mumps vaccine should not be administered to pregnant women, who are severely ill or who are on Immuno suppressive therapy
- 21. Mumps Vaccine • Composition Live virus (Jeryl Lynn strain) • Efficacy 80% (1 dose) • Duration of Immunity Lifelong • Schedule At least 1 Dose should be administered with measles and rubella as MMR or with measles, rubella and Varicella as MMRV
- 22. Mumps (MMR) Vaccine Indications • One dose (as MMR) for preschool-age children 12 months of age and older and persons born during or after 1957 not at high risk of mumps exposure • Second dose (as MMR) for school-age children and adults at high risk of mumps exposure (i.e., healthcare personnel, international travelers and students at post-high school educational institutions
- 23. MMR Adverse Reactions • Fever 5%-15% • Rash 5% • Joint symptoms 25% • Thrombocytopenia <1/30,000 doses • Parotitis* rare • Deafness* rare • Encephalopathy <1/1,000,000 doses *reactions usually attributed to the mumps component
- 24. MMR Vaccine Contraindications and Precautions • Severe allergic reaction to vaccine component or following a prior dose • Pregnancy • Immunosuppression • Moderate or severe acute illness • Recent blood product
- 25. Vaccine Storage and Handling MMR Vaccine • Store 35o - 46o F (2o - 8o C) (may be stored in the freezer) • Store diluent at room temperature or refrigerate • Protect vaccine from light • Discard if not used within 8 hours reconstitution
- 26. MIG • a) IMMUNO GLOBULIN: • A specific Immuno globulin (MIG) is available. • CONTROL: The control of mumps is difficult because the disease is infectious before a diagnosis can be made. Due to long I.P, sub clinical cases, - it is difficult to control mumps. • Isolation of cases. • Disinfection of the articles. • Contacts kept under surveillance
- 27. RUBELLA (GERMAN MEASELS • RUBELLA or German Measles is an acute child hood infection usually mild of short duration (3 days) and accompanied by low- grade fever, lymphadenopathy and a maculopapular rash. Infection in early pregnancy may result in serious congenital defects like PDA, cataract and deafness. Rubella in pregnancy can also cause spontaneous abortion and stillbirth.
- 28. RUBELLA HISTORY • HISTORY: • 1941 – Norman Gregg – reported rubella infection in pregnancy WHICH IN TURN linked to congenital anomalies including congenital cataracts. • 1962 – The virus was isolated. • 1967 – Live attenuated vaccine was developed.
- 29. Epidemiological Determinants AGENT: • It is a RNA virus of the Toga virus family. • Virus can be recovered from the cases of Rubella, from naso- pharynx, throat, blood, CSF and urine. • It can be propagated in cell culture.
- 30. SOURCE OF INFECTION • Clinical or sub clinical cases of rubella. Most of the infections are sub clinical. Infants born with infection may shed the virus, for many months. Vaccine virus is not communicable.
- 31. AGENT&HOST FACTORS: • Period of Communicability • Less communicable than measles. • Probably one week prior to symptoms to a week after appears.
- 32. HOST FACTORS • a) AGE: Mainly a disease of child hood in age group of 3 – 10 yrs. • - Persons aged > 15. Yrs now account for over 70% of cases in developed countries. This is changing epidemiological pattern with wide coverage of immunization. • IMMUNITY: One attack results life long immunity. 40% women of childbearing age may remain susceptible to rubella
- 33. EPIDEMIOLOGY • ENVIRONMENTALFACTORS: Seasonal variation is present, temperate zones every 4-9 yrs. • TRANSIMISSION: Droplets from nose and throat and droplet nuclei transmit the virus directly from person to person during communicability period. • -The portal of entry is via respiratory route. • - Vertical transmission is also present.
- 34. CLINICALF EATURES • CLINICAL FEATURES: 50-65% of infections are asymptomatic. • a)PRODROMAL: Symptoms like coryza, sore throat, and low-grade fever – herald the onset of viraemia. • b)LYMPHADENOPATHY:Posterior auricular lymph nodes, and posterior cervical group will be enlarged 7 days before rash appearance and it continues 10-14 days after the rash. Some times no lymphadenopathy.
- 35. CLINICALFEATURES • a) RASH: Appears first on face. Rash is like minute, discrete, pinkish, macular rash and not confluent. Rash spreads to trunk and extremities. Rash disappears by 3 rd day. • b) COMPLICATIONS: • - Arthralgia • - Encephalitis (rare) • - Thrombocytopenia purpura • Congenital anomalies of newborn baby
- 36. DIAGNOSIS OF RUBELLA • By virus isolation and serology. 1. - Throat swabs should be cultured for virus isolation. Most widely used test is haemagglutination inhibition test (HAI). • - 4-fold rise in HI antibody titer in paired sera or presence of – IgM in a single serum sample after 2 weeks of rash is diagnostic of rubella. • - More sensitive serological tests include Elisa test and radio immune assay.
- 37. Congenital Rubella Syndrome • Refers to infants born with defects secondary to intrauterine infection or with defects some time after birth. Congenital infection is diagnosed by - Rubella infection inhibits cell division. – reason for congenital malformation and low birth weight.
- 38. CONGENITAL RUBELLA SYNDROME • - Common congenital defects are deafness, cardiac malformations, cataracts, glaucoma, retinopathy, microcephalus, cerebral palsy, IUGR, hepato – splenomegaly and mental and motor retardation. • The first trimester of pregnancy infection affects the fetus and newborn baby with congenital defects, > abortion, stillbirth, PDA, cataract and deafness
- 39. PREVENTION • Active immunization with live attenuated vaccine. • RUBELLA VACCINE: 1979 – RA 27/3 vaccine (human diploid fibroblast) – produces higher antibody titer with good immune response. • Administration in a single dose 0.5 ml S.C • Sero conversion occurs in more than 95% vaccinees. Immunity persists for 14-16 yrs. • Infant should not be vaccinated. • Pregnancy – is contra indication for immunization. • Recipients of the vaccine should be advised not to become pregnant for next 3 months
- 40. Vaccination strategy • Combined vaccine MMR. VACCINATION STRATEGY: • - First to protect women of child bearing age (15-34/39) • Then interrupt transmission of rubella by vaccinating all children 1-14 yrs. • Subsequently all children at one-year age.
- 41. 41 Prevention of Rubella Immunization • Rubella vaccine: RA 27/3 strain,0.5 ml, SC,Life long immunity in 95% • C/I for immunization: Pregnancy • Recipients of vaccine should be advised not to become pregnant in 3 months after getting vaccine • MMR vaccine
- 42. 42 Vaccination strategy for Rubella • First protect women in 15-39 yr age • Second interrupt transmission by vaccinating children aged 1-14 years • Third, all children at age 1
- 45. 45 Global Measles and Rubella Strategic Plan 2012-2020 In 2012, the M&R Initiative launched a new Global Measles and Rubella Strategic Plan which covers the period 2012-2020. • By the end of 2015 the plan aims: to reduce global measles deaths by at least 95% compared with 2000 levels; • To achieve regional measles and rubella/congenital rubella syndrome (CRS) elimination goals. • By the end of 2020 the plan aims: to achieve measles and rubella elimination in at least 5 WHO regions.
- 46. 46 The strategy focuses on the implementation of 5 core components: • Achieve and maintain high vaccination coverage with 2 doses of measles- and rubella-containing vaccines; • Monitor the disease using effective surveillance, and evaluate programmatic efforts to ensure progress and the positive impact of vaccination activities; • Develop and maintain outbreak preparedness, rapid response to outbreaks and the effective treatment of cases; • Communicate and engage to build public confidence and demand for immunization; and • Perform the research and development needed to support cost- effective action and improve vaccination and diagnostic tools.