
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Cementum: Structure, Formation and Functions
Ähnlich wie Cementum: Structure, Formation and Functions (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Cementum: Structure, Formation and Functions
- 2. Introduction • It was first demonstrated microscopically in 1853 by Frankel and Raschkow. • Periodontium = Gingiva, PDL, alveolar bone & cementum. 2
- 3. • Cementum = from latin word “cement” (means quarried stone). • Cementum is the calcified mesenchymal tissue that forms the outer covering of the anatomic root. 3
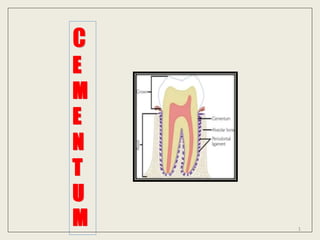
- 4. • It is considered as part of periodontium (supporting & attachment apparatus of tooth) • it gives attachment to the PDL fibers. • It shows some similarities with bone, but it is avascular. 4
- 5. Definition • It is a mineralized dental tissue covering the anatomic roots of human teeth (Orbans). 5
- 6. Physical properties • Colour – yellowish & lighter than dentin. • Hardness – less than enamel, dentin & bone. • Permeability – to H2O & inorganic ions (decrease with age & affected by plaque/calculus) 6
- 7. • Thickness – thinnest at cervical region (20-50um) & thickest towards root apex (150-200um). • EXTENSION: Begins at the cervical portion of the tooth at the CEJ and continues to the apex 7
- 8. • Less readily resorbed than bone • Softer and lighter than dentin • Lacks luster and is dark, and is therefore differentiated from enamel 8
- 9. Chemical composition • Organic content – 50 – 55% • Inorganic content - 45 – 50 % • and water 9
- 10. Inorganic components • Consists of - 45-50% • similar - to bone & dentin. • Shows – Ca & PO4 ions (in hydroxyl apatite crystals), - trace elements – Cu, Fe, F, Mg Na, Zn, Si & K 10
- 11. • F- ion content is highest among all body hard tissues • Mg content is half of the dentin. 11
- 12. Organic components • Consists of - 50-55%. • Proteins Collagenous • mainly type 1 collagen fibers (90%), other types (3, 5, 6, 12, 14). 12 Collagenous Non collagenous
- 13. Non-collagenous proteins • help in formation & mineralization of cementum • alkaline phosphates, osteonectins, osteocalcin, sialoproteins, osteopontin, proteoglycans & GFs (BMPs, FGF & PDGF) • Cementum attachment proteins (CAP) & Cementum derived GFs – promote cementum formation 13
- 14. 14
- 15. 15
- 16. 16
- 18. Cementogenesis = Process of formation of cementum • It takes place in two phases: – Matrix formation – Mineralization • There are 3 cell types responsible for the cementogenesis: – Cementoblasts – Cementocytes – Fibroblasts 18 All of these cells are differentiated ectomesenchymal cells.
- 19. • Cementum formation starts during root formation and continues throughout the life. • Under the influence of IEE cells of HERS, the outer most cells of dental papilla differentiate into odontoblasts which deposits dentin. 19
- 20. • Later, HERS is invaded by cells of dental follicle • Just before degeneration of the HERS, a thin cell-free layer of cementum is formed on the surface of dentin - INTERMEDIATE CEMENTUM. • D.sac cells come in contact with newly formed root dentin & get differentiated into cementoblasts. 20
- 21. Cementoblasts – • polygonal cells that secrete collagen & protein polysaccharides. • They contribute to formation of organic matrix of cementum (called cementoid). • Have numerous RER, GC, with vesicular nucleus. 21
- 22. • Newly deposited cementum called Cementoid (organic matrix that contains collagen bundles & ground substances) which later undergoes mineralization. • Cementoblasts move outwards during cementum formation and some of them entrapped in the matrix during deposition & are called cementocytes. 22
- 23. • Cementocytes are seen in the lacunar space in the mineralized cementum. • Cementocytes shows processes in the canaliculi which are directed towards PDL.(because through this processes cementocytes gets nutrition from PDL) 23
- 24. • After matrix deposition, mineralization of cementum occurs in the form of fine crystals and matrix vesicles near the calcifying fronts. (these crystals are parallel to root surface at – apical region & perpendicular to root surface – at lateral and coronal regions) 24
- 25. • During cemental formation, fibers from PDL (sharpeys fibers) are inserted into cementum matrix & provides attachment B/W tooth & alv bone. 25
- 26. Classification of cementum Based upon – • Presence or absence of cementocytes • on the basis of types of fibers & the presence or absence of cementocytes. 26
- 27. Presence or absence of cells Acellular cementum/ Primary cementum- • 1st formed cementum • Is formed before the tooth reaches the occlusal plane. Cellular cementum /secondary cementum • Is formed after the tooth reaches the occlusal plane. • Formed later & during repair —secondary cementum 27
- 28. Acellular Cementum Cellular Cementum Also called Also called as primary cementum Also called as secondary cementum cells Embedded cementocytes are absent Embedded cementocytes are present Rate of deposition Deposition rate is slower Deposition rate is faster Formed It is the first formed layer Formed after acellular cementum Width Width is more or less - constant Width can be highly variable Found Found more at cervical third of tooth Mainly seen at apical third & interradicular area though a thin layer is present all over the root Sharpeys fibers Sharpey’s fibers are well mineralized Sharpey’s fibers are partially mineralized Incremental lines Incremental lines are regular & closely placed Incremental lines are irregular & placed wide apart with variable thickness between them 28
- 29. Cementum shows 2 types of fibers— extrinsic fibers intrinsic fibers 29
- 30. Extrinsic fibers (Sharpey’s fibers) • derived from PDL fibroblasts. • larger diameter bundles (5–7 microns) • oriented perpendicular to root surface. 30
- 31. Intrinsic fibers • derived from cementoblasts. • Smaller in diameter (1–2 microns) • Run parallel to the root surface and at right angles to the extrinsic fibers. 31
- 32. on the basis of types of fibers & the presence or absence of cementocytes. (1) Acellular afibrillar cementum (AAC) (2) Acellular extrinsic fiber cementum (AEFC) (3) Cellular intrinsic fiber cementum (CIFC) (4) Cellular mixed fiber cementum (CMFC) (5) Cellular mixed stratified cementum (CMSC) 32
- 33. Acellular afibrillar cementum (AAC) • It shows Mineralized ground substance containing no cells and is devoid of extrinsic & intrinsic collagen fibers. • seen as coronal cementum, • with a thickness of 1 to 15 um. 33
- 34. Acellular extrinsic fiber cementum (AEFC) • extends from cervical margin to apical 1/3rd. • Seen mostly in single rooted teeth. • extrinsic fibers seen perpendicular to surface of cementum. • Thickness = 10 to 50 μm wide near CDJ. • Noncollagenous proteins—tenascin, fibronectin, osteocalcin absent. • Growth factors - TGFβ and IGF not seen 34
- 35. • formed slowly and regularly. • Incremental lines are placed parallel to tooth surface and closer than in cellular cementum. • Cementoid is usually absent. • Function = anchorage especially in single rooted teeth. 35
- 36. Cellular Intrinsic Fiber Cementum (CIFC) • contains cells and intrinsic fibers & has no extrinsic fibers. • intrinsic fibers are secreted by the cementoblasts. • Located in apical 3rd & furcations of root • Formed later (2ry cementum) & during repair • Cementoid seen on the surface 36
- 37. • Main function is adaptation & repair • Rapidly formed • Cementoblasts of this express parathormone receptor (PTH) • Incremental lines - apart 37
- 38. Cellular mixed fiber cementum (CMFC) • formed at a faster rate with less mineralized fibers. • Fibers are derived from PDL fibroblasts & cementoblasts. • Number of intrinsic fibers are comparatively less than extrinsic fibers. 38
- 39. Cellular mixed stratified cementum (CMSC) • In this, the cellular intrinsic fiber cementum alternates with acellular extrinsic fiber cementum. • It is formed by cementoblasts & fibroblasts. • appears primarily on apical 3rd of root and furcation areas. • thickness varies from 100–1000 um. 39
- 40. CEMENTOENAMEL JUNCTION (CEJ) • Is the junction B/W cementum & enamel at the cervical portion of the tooth & its variable. • Three types of joints are seen – sharp (butt), gap & over lap joints. • Rarely, enamel overlaps the cementum. 40
- 41. 41
- 42. Overlap junction • cementum overlaps the enamel. • Occurs when the REE covering the crown degenerates near cervical portion, permitting cells of dental sac come in contact with enamel & form cementum over it. • most common type & seen in 60% of teeth. 42
- 43. Sharp (Butt) joint • Or edge to edge joint. • cementum meets enamel in a sharp line. • Seen in 30% of teeth. 43
- 44. Gap joint • cementum doesn’t meet the enamel & gap is present B/W both. • Some part of root is devoid of cementum. • This is due to delay in degeneration of HERS, that prevents contact b/w dental sac cells & dentin, lead to lack of differentiation of cementoblasts. • Seen in 10% of teeth. 44
- 45. CEMENTODENTINAL JUNCTION (CDJ) • Is the jn b/w cementum & dentin. • Is straight – in permanent teeth, but scalloped in 1ry teeth. • More prominent in cellular cementum than in acellular. • At this jn, dentinal fibers intermingle with cemental fibers. 45
- 46. 46
- 47. INTERMEDIATE CEMENTUM • sometimes, cementum is separated from dentin by a layer of intermediate cementum. • The exact nature of intermediate layer is a subject of controversy • Is structureless & doesn’t show features of cementum or dentin. • As it appears hyaline (structureless), it is also known as Hyaline layer (HYALINE LAYER OF HOPEWELL SMITH) • It is mostly seen in the apical 2/3rd of molars, premolars & is rarely observed in incisors or deciduous teeth. 47
- 48. • It is believed that this layer represents areas where cells of HERS trapped in a rapidly deposited dentin or cementum matrix. Function - seals root dentin. 48
- 49. INCREMENTAL LINES OF CEMENTUM (LINES OF SALTER) • Cemental annulations • Formed by fiber-free amorphous substance • Represent intervals between successive deposition of cement • In both types of cementum incremental lines run roughly parallel with the root surface. • Not have regular rhythmic distribution & Unevenly spaced. 49
- 50. • Comparatively, Acellular cementum - show more regular lines than cellular cementum. • Counting of these lines shown to be 1. indicators of age & 2. disturbances in metabolism. 50
- 52. 1. Anchorage (attachment) • cementum provides medium for attachment of PDL fibers b/w tooth & alv bone, there by it provides anchorage to teeth. • Acellular cementum mainly involved in attachment process. 52
- 53. 2. Adaptation • Masticatory forces → cause occlusal wearing → thereby reduces tooth length. • By continuous deposition of cellular cementum at apical region of root, tooth length is maintained. 53
- 54. 3. Repair • fractures /resorption in the roots are repaired by the deposition of cellular cementum. • cementum is more resistant to resorption than bone. • But, In case of excessive trauma, resorption of cementum can take place. • In such case cementum is repaired by the dep of cellular cementum. 54
- 55. • Cementum repair is of two types 55
- 56. . 56 Anatomical repair Functional repair Occur when degree of damage to cementum is low Occur when degree of damage to cementum is high Resorbed area is completely filled with cementum Resorbed area is partially filled with cementum, resulting in bay-like defect on root surface the continuity of root and PDL is re- established. Alv bone forms a bony projection in to damaged cementum establish normal width of PDL. bone root Bay like defect
- 57. Clinical considerations of cementum 1. Orthodontic treatment 2. Tooth sensitivity and root caries 3. Cementicles 4. Hypercementosis 5. Hypophosphatasia 6. Cemental spurs 57
- 58. Orthodontic treatment • when compared to bone cementum show more resistant towards resorption as it is avascular. (This feature of tooth made used in orthodontic movement of tooth.) • Controlled application of pressure on tooth makes toot movement. • The pressure exerted during orthodontic movements causes resorption of bone towards the direction of force & teeth shows desired movements. 58
- 59. 59
- 60. 60
- 61. Tooth sensitivity • apical migration of gingiva leads to exposure of root & exposed part of root shows cemental wearing & this exposes underlying dentin. • These events leads to tooth sensitivity and these areas have more chances of developing root caries. 61
- 62. 62
- 63. Cementicles • these are small masses of cementum attached to the root surface or located freely in the PDL. • Occurs due to microtrauma causing cemental tear. • more common in apical & middle 3rd of root and in furcation areas. 63
- 64. Hypercementosis • Excessive formation of cementum is called hypercementosis. • It can be localized (involve single tooth) or generalized (involve multiple teeth ) • occurs due to physiological causes like in accelerated eruption of teeth or pathological causes like 2ry to chronic periapical infections, Paget’s disease. • Makes difficulty in extraction of tooth. 64
- 65. • When excessive dep of cementum that improves the function of tooth – Cemental hypertrophy. • Excessive dep of cementum in non-functional tooth – Cemental hyperplasia. 65
- 66. Hypophosphatasia • reduction/absence of cementum on root as seen. • no proper attachment b/w tooth and alv bone. 66
- 67. Cemental spurs • dep of more cementum on the root surface and is appear as attached spheres called cemental spheres. • Misinterpreted as calculus clinically & radiologically. 67
- 68. 68
- 69. 69