
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Apophyseal injuries of elbow , medial epicondyle avulsion fractures
Ähnlich wie Apophyseal injuries of elbow , medial epicondyle avulsion fractures (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Apophyseal injuries of elbow , medial epicondyle avulsion fractures
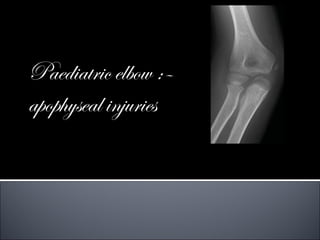
- 1. Paediatric elbow :– apophyseal injuries
- 3. COMMON AGE -9 AND 14 M:F = 4 : 1 during sports -Medial epicondyle avulsion #s most commonly affect adolescent baseball pitchers during periods of rapid growth, typically between 9 and 14 years of age. This is when the growth plate cartilage is most vulnerable to injury. One hard pitch can cause an avulsion fracture. The forearm muscles anchored to the elbow at the medial epicondyle growth plate contract forcefully during the pitching motion. ABOUT 50% ASSOCIATED WITH ELBOW DISLOCATION THE APOPHYSEAL FRAGMENT COULD BECOME ENTRAPPED WITHIN THE JOINT (15-18%)
- 4. Signs & symptoms The main symptom is sudden onset of severe pain on the inside of the elbow following a forceful pitch or throw. Some athletes feel or hear a pop at the time of the injury. There is usually swelling and some limitation of elbow motion. Occasionally the ulnar nerve, which sits next to the medial epicondyle, becomes irritated after an avulsion fracture, causing numbness and tingling in the forearm and fourth and fifth fingers.
- 5. As ossification progresses, parallel smooth sclerotic margins develop in each side of the physis. Because it is somewhat posterior, on a slightly oblique AP view the apophysis may be hidden behind the distal metaphysis. The concentric oval nucleus of ossification of the medial epicondylar apophysis .
- 6. Elbow ossification centers Order of Appearance of the individual ossification centers is C-R-I-T-O-E: (F/M) Capitullum 1 yo/2 yo Radial head 3 yo/4 yo Medial epicondyle 5 yo/6 yo Trochlea 7 yo/8 yo Olecranon 9 yo/10 yo Lateral epicondyle 11 yo/12 yo
- 7. The medial epicondyle is a traction apophysis does not contribute to the distal humerus overall length In the early ossification process –it is a part of the entire distal humeral epiphysis With growth and maturity - becomes separated arises from the posterior surface of the medial distal humeral metaphysis
- 8. Posteromedial location ossification center may be difficult to see on an AP x-ray best appreciated on a lateral x-ray on AP x-rays, the distal medial metaphyseal border may overlap the ossific nucleus of the apophysis - misinterpreted as a fracture
- 9. Effusion is associated with a fracture 70-90% kids Risk of occult fracture is approximately 30%-75% Posterior or elevated anterior fat pad abnormal
- 10. Soft Tissue Attachments The flexor mass, FCR, FCU, FDS, PL and part of the pronator teres. Capsule – In younger children, some of the capsule's origin extends up to the physeal line of the epicondyle - a fracture line involving the medial epicondylar apophysis can enter the joint
- 11. In older children and adolescents, as the epicondyle migrates more proximally, the capsule is attached only to the medial crista of the trochlea Ligamentous Structures The ulnar collateral ligament - three separate bands –anterior, oblique and posterior
- 12. Acute injuries - Three theories 1. A direct blow, posterior aspect / posterior medial aspect 2. Avulsion mechanisms, Avulsion in elbow extension (valgus stress) Avulsion with elbow flexed (pure muscle forces) – throwing base ball, arm wrestling. conservative treatment good results. Little League Elbow: medial epicondylar apophysitis secondary to repeated valgus stress from throwing; medial epicondyle has the longest exposure to medial distraction forces because it is the last ossification center to close. medial epicondylar avulsion fractures are the most common elbow injury during adolescence
- 13. 3. ASSOCIATION WITH ELBOW DISLOCATION - ulnar collateral ligament provides the avulsion force. an extreme valgus stress was applied to the joint, a vacuum was created within the joint . The normal valgus carrying angle tends to accentuate these avulsion forces when the elbow is in extension. These associated injuries like radial neck fractures with valgus angulation and greenstick valgus fractures of the olecranon confirms the valgus force theory.
- 14. fracture of the radial neck, olecranon, or coronoid process. If the epicondyle fragment is only rotated on its axis, the anterior band of the ulnar collateral ligament can become lax. This laxity can produce some medial elbow instability during extension
- 15. Acute injuries 1.Un-displaced -the physeal line remains intact. swelling and local tenderness over the medial epicondyle. On x-ray, the smoothness of the physeal line's edge remains intact. Although there may be some loss of soft tissue planes medially on the x-ray, displacement of the elbow fat pads may not be present because the pathology is extra- articular 2.Minimally displaced fractures -a stronger avulsion force- more soft tissue swelling. Palpating the fragment may elicit crepitus . On x-ray, there is a loss of parallelism of the smooth sclerotic margins of the physis . The radiolucency in the area of the apophyseal line is usually increased in width.
- 16. 3.Displaced fractures There may have been an elbow dislocation that reduced spontaneously or by manipulation On x-ray, the long axis of the epicondylar epiphysis is rotated medially .The displacement usually exceeds 5 mm, but the fragment remains proximal to the true joint surface. This fragment may contain a metaphyseal fragment
- 17. 4.Incarcerated#s(without elbow dislocation) The key clinical finding is a block to motion, especially extension On x-ray, totally or partially within the elbow joint until proven otherwise . Elbow is usually still found to be incompletely reduced. Due to an impingement of the fragment within the joint, a good AP view may be difficult to obtain caused by the inability to extend the elbow
- 18. If the fracture is old and if the fragment is fused to the coronoid process, widening of the medial joint space may be the only clue that the fragment is lying in the joint. The epicondylar ossification center may become fragmented and mistaken for the fragmented appearance of the medial crista of the trochlea. Absence of the apophyseal center on x-ray may be further confirmatory evidence that the fragment is within the joint. Comparison x-rays of the opposite elbow may be necessary to delineate the true pathology.
- 19. Even if the elbow is dislocated, the fragment can still lie within the joint and prevent reduction. Recognition of this fragment as being within the joint before a manipulation points a need for open reduction. An initial manipulation to extract the fragment from the elbow joint may need before a satisfactory closed reduction of the elbow
- 21. The function of the ulnar nerve must be carefully documented Valgus Stress Test: Because the ulnar collateral ligament's anterior oblique band may be attached to the medial epicondylar apophysis, the elbow may exhibit some instability after injury This test is performed with the patient supine and the arm abducted 90 degrees. The shoulder and arm are externally rotated 90 degrees. The elbow must be flexed at least 15 degrees to eliminate the stabilizing force of the olecranon. If the elbow is unstable, simple gravity forces will open the medial side. A small additional weight or sedation may be necessary to acquire an accurate assessment of the medial stability with this test.
- 22. Slightly displaced or non- displaced - Widening or irregularity of the apophyseal line If the fragment is totally incarcerated - hidden by the overlying ulnar or distal humerus - total absence of the epicondyle from its normal position If the fracture is only minimally displaced and if it is the result of an avulsion injury, there may be no effusion because all the injured tissues remain extra- articular.
- 23. Most avulsion fractures can be successfully treated with cast immobilization for 4-6 weeks. During this time ice can be placed on the elbow for 20-30 minutes every 3-4 hours while there is pain or swelling. After 4-6 weeks of immobilization, if X-rays show the fracture is healing do physiotherapy . While most avulsion fractures heal well with this treatment, those with a very wide separation on X-rays may require surgery. The recovery time after surgery is similar that for non-surgical treatment.
- 24. Absolute indication : Irreducible incarcerated fragment in the elbow joint Roberts' Manipulative Technique It involves placing a valgus stress on the elbow while supinating the forearm and simultaneously dorsiflexing the wrist and fingers to place the forearm muscles on stretch; theoretically, this maneuver should extract the fragment from the joint. To be effective, this procedure should be carried out within the first 24 hours after injury.
- 25. Failure to extract the fragment by manipulative techniques open extraction and reduction have been performed with screw fixation or sutures to secure the fracture in position. Excision has also been advocated, especially if the fragment is comminuted. On a long-term basis, intra- articular retention of the fragment may not be all that disabling. The epicondyle had fused to the semilunar surface of the ulna, producing a large bony prominence clinically. There was only minor loss of elbow motion, with little functional disability.
- 26. Relative indication: 1. Ulnar nerve dysfunction 2. Patient with high- demand upper extremity function A universal finding - a thick fascial band that binds the ulnar nerve to the underlying muscle The constriction is believed to be responsible for either the immediate or late dysfunction of the ulnar nerve.
- 27. medial condylar physis injuries . This is especially true if the secondary ossification centers are not present If there is a significant hemarthrosis or a significant piece of metaphyseal bone accompanying the medial epicondylar fragment, arthrography or MRI may be indicated to determine if there is an intra-articular component to the fracture
- 28. Major Failure to recognize incarceration in the elbow Ulnar nerve dysfunction Minor Loss of elbow extension Myositis ossificans Calcification of the collateral ligaments Loss of motion Cosmetic effects Nonunion in the high-performance athlete
- 29. most common indication for operative intervention is to ensure a stable elbow in patients participating in high-demand activities with their upper extremity 1. A longitudinal incision just anterior to the medial epicondyle. 2. The fragment is usually displaced distally and anteriorly 3. The periosteum is removed from the fracture site, and the clot is extracted by irrigation. It is important to identify and protect the ulnar nerve, but a complete dissection of the nerve is usually unnecessary 4. The elbow is flexed and the forearm is pronated. A towel clip is used to reduce the #. 5. The fragment is reduced and stabilized temporarily with one or two small K-wires 6. Final fixation by partially threaded and over drilled in the epicondylar fragment to compress it against the metaphysis/a cannulated 4 mm screw 7. After removal of the K-wires, the elbow is checked to ensure valgus stability and re- establishment of a full range of motion. 8. After the surgical incision is closed, the extremity is placed in a long-arm cast(bi-valved.) 9. At 5 to 10 days, active motion is initiated.
- 30. epicondyle is fragmented spike washer can be used to secure the multiple pieces to the metaphysis or excise the fragments and reattach the ligament to the bone and periosteum at the base of the epicondylar defect.
- 31. Preventing medial epipcondyle avulsion fractures Lots of pitching puts repetitive stress on the medial epicondyle growth plate, which can weaken it and make it more prone to avulsion fracture. The best way to prevent medial epicondyle avulsion fracture is to follow the attached guidelines for appropriate pitch count limits and proper rest between pitching appearances. DO NOT throw through pain. Pain is a sign of injury, stress, or overuse. Pushing through pain will only worsen the injury. Rest is required to allow time for the injured area to heal.
- 32. a rare injury begins to ossify around 10 to 11 years of age Mechanism of Injury In adults - a direct blow In children - avulsion forces
- 33. If between the origin of the common extensors and the extensor carpi radialis longus - little displacement. If the fracture lines enter the area of origin of the extensor carpi radialis longus - considerable displacement
- 34. X-Ray Findings The natural separation can be confused with an avulsion fracture The key to determining true separation is looking beyond the osseous tissues for the presence of associated soft tissue swelling
- 35. Simple immobilization for comfort. Surgery – if fragment is incarcerated within the joint Complications Entrapment of the fragment, either within the elbow joint or between the capitullum and the radial head
- 36. avulsion forces on the proximal ulna that occur with the elbow flexed occur more often in children with osteogenesis imperfecta - reason unknown. an isolated, displaced fracture of the olecranon apophysis – consider OI.
- 37. Operative treatment - for displaced fractures. Acceptable displacement ranges from 3 mm to 5 mm. 70% of children with OI who sustain an olecranon apophyseal fracture later have a fracture of the contralateral olecranon apophysis
- 38. Rarest form of epiphyseal detachment
- 39. Ossification of the olecranon develops in the area of the triceps insertion-9yrs Bipartite centers Traction centre-1st Enveloped by the triceps insertion Second smaller- articular centre
- 40. classification Type1-apophysitis Type2-incomplete stress# Type3-complete # A-pure apophyseal avulsions B-apophyseal-metaphyseal combination
- 41. UN DISPLACED INJURIES Rest, selective muscle exercise programme. Persistent non union Cannulated compression screw across the apophysis to stimulate healing DISPLACED FRACTURES Minimal displacement closed reduction by extension then long arm cast/percutaneous pinning Complete dis. small children K-wire TB with strong absorbable sutures. Older do TB with steel wire Large ossif. centretreated same like meta #s.
- 42. SPUR FORMATION Overgrowth of epiphysis Symptomatic-removed Non union Apophyseal arrest
- 43. Isolated meta #rare CLASSIFICATION Group A-flexion injuries Group B- extension injuries 1. valgus pattern 2.varus pattern Group C-shear injuries
- 44. Most common Even if the fracture is severely displaced- immobilization in full/partial extension heal satisfactorily Displaced/comminuted ORIF Fixation devices- absorbable sutures/axial screw/TBW with axial K- wire Combination of screw+fig of eight is best If axial wires used the disadvantage is s/c prominence
- 45. Often in varus the olecranon angulation corrected with elbow in extension ,also reduces radial head. If there is Painful subluxation of the radial head present -a delayed osteotomy of the proximal ulna/olecranon.
- 46. Distal fragment displaced anteriorly with Posterior periosteum intact best reduced in hyperflexion If Periosteum torned Fix it with an oblique screw so that you can start mobilization earlier.
- 47. IRREDUCIBILITY Proximal frag. entrapped in the joint Non union/Delayed union Compartment syndrome Nerve injuries Elongation Loss of reduction
- 48. Up to 6 yrs coronoid epiphyseal 1%-2% Most fractures occur with dislocations of elbow
- 49. Type1-avulsion of the tip of the coronoid process only Type2-a single/comminuted fragment <=50% Type3->50% Type 1 and 2Conservatively with early motion if no associated injuries With elbow dislocation- forearm full supination elbow 100 degrees of flexion.
- 50. Large fragment and marked displacement- ORIF Hentry anterior approach to the elbow. The fragment can be fixed with a mini fragment screw or sewn in place through 2 drill holes to the posterior aspect of the ulna. COMPLICATIONS Large fragment the elbow may be unstable and prone to recurrent dislocations. Non union with the production of a free fragment in the joint occurs rarely in children.
- 51. Thank you