1. CHEST Radiology
อ.พญ.วิรณา อางทอง
ภาควิชารังสีวิทยา มหาวิทยาลัยศรีนครินทรวิโรฒ
1.Pneumothorax.
1.2 Simple pneumothorax.
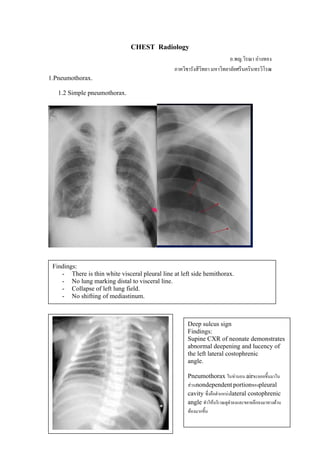
Findings:
- There is thin white visceral pleural line at left side hemithorax.
- No lung marking distal to visceral line.
- Collapse of left lung field.
- No shifting of mediastinum.
Deep sulcus sign
Findings:
Supine CXR of neonate demonstrates
abnormal deepening and lucency of
the left lateral costophrenic
angle.
Pneumothorax ในทานอน airจะลอยขึ้นมาใน
สวนnondependent portionของpleural
cavity ซึ่งคือตําแหนงlateral costophrenic
angle ทําใหบริเวณดูดําลงและขยายลึกลงมาทางดาน
ทองมากขึ้น
2. 1.2 Tension pneumothorax:
Findings:
- There is thin white visceral
pleural line at left side
hemithorax.
- Marked collapse and distortion
of let lung.
- Shifting of mediastinum to the
right side which is compatible
with tension pneumothorax.
***Small pneumothorax is easier seen on an expiration film, due to reduce lung
volume which make pneumothorax look relatively larger.
2. Pneumomediastinum
Findings:
-There is linear radiolucency of air density outlining the left subclavian
artery and the left carotid artery (tubular arterysign). (จะเห็นairอยูรอบ ๆหลอดเลือดที่อยูใน
mediastinum)
-Lateral radiograph demonstrates the “ring around the artery” sign. (จะเห็นair density
โอบลอมรอบหลอดเลือดในmediastinumเปนรูปวงแหวน ภาพดานบนโอบรอบright pulmonary artery.
3. The continuous diaphragm
sign (เห็นเปนair density ทางดานลาง
ของmediastinum ซึ่งair นี้จะเซาะอยู
ทางดานหนาของpericardial cavity จึง
เห็นเหมือนเปนเงาของdiaphragmที่
ตอเนื่อง)
Findings:
-Air in the subcutaneous
tissues of the neck (subcutaneous
emphysematous)
-Thymic sail sign: thymus is out line
by air. (airในmediastinumเซาะตามขอบของ
thymus)
3. Pleural effusion.
Findings:
-Homogeneous density
-Concave at upper border
-Meniscus shape at edge of
right pleural effusion ( Higher
lateral than medial)
-If large amount of pleural
effusion will displace the
mediastinum towards the
contralateral side.
4. 4. Loculated pleural effusion
Findings:
- Haziness of right hemithorax (density not corresponding to lobar
anatomy ).
- Lateral film below shows loculated fluid overlying vertebral column
Findings:
- Unusual shape (lentiform) or unusual
position in the thorax cavity.
Large right pleural effusion
Findings:
-The right hemithorax is
opaque.
- There is shift of heart and
trachea away from the side of
opacification.
5. 5. Hydropneumothorax
-There is opacification at left lower thorax with air-fluid level.
6. CHF
6.1 Pulmonary interstitial edema
- Kerley B lines
- Kerley A lines
(Kerley – thicken connective
tissue septa )
- Peribronchial cuffing:
thicken bronchial wall and
peribronchial sheath.
- Thickening of the fissures
- Pleural effusion
- Perihilar haze: blurring of
hilar shadows.
- Blurring of pulmonary
vascular markings
6. Kerley B line:
-Faint multiple white lines
perpendicular to the pleural
surface and 1-2 cm long.
Kerley A line:
-Relatively long linear
shadows in upper lung, deep
within lung parenchyma.
Peribronchial cuffing:
-Bronchial wall thickening
7. Fluid in minor fissure
6.2 Pulmonary alveolar edema
Findings:
-Symmetrical bilateral opacification
spreading from the hilar regions into
the lungs with sparing of peripheral
lung fields is called butterfly or bat
wing configuration.
-Cardiomegaly.
Findings:
-Bilateral air space infiltration
(or alveolar infiltration) at
bilateral perihilar region
-Air bronchogram is seen.
-Cardiomegaly.
8. 7. Metastasis
Findings:
-Multiple well-defined pulmonary nodules scatter both lung
fields which are vary in size.
8. Bronchiectasis
Findings:
-There are multiple thin wall cystic areas at perihilar region of both lung
fields which some of them show air-fluid level.
9. 9. Emphysema
Findings:
-Over expanded lungs
-Flat diaphragms lying below the 6th rib anteriorly.
-Increase retrosternal airspace on lateral film
-Decreased vascular markings of lung fields
-Increase AP diameter of cheast and anterior bowing of sternum
-Narrow mediastinum
10. Mediatinal mass
10.1 Anterior mediastinal mass
-The anterior mediastinum is bounded anteriorly
by the sternum; posteriorly by the pericardium,
aorta, and brachiocephalic vessels; superiorly by
the thoracic inlet; and inferiorly by the diaphragm
-Its contents include the thymus, lymph
nodes, adipose tissue, and internal mammary vessels
10. Findings: lymphoma in anterior mediastinal mass
-There is a large lobulated mass causes obliteration of cardiac shadow which
could be anterior mediastinal mass.
-The descending aorta is clearly seen which indicating that this mass not within
posterior mediastinm.
10.2 Middle mediastinal mass
11. -The middle mediastinum is bounded anteriorly by the pericardium, posteriorly by the
pericardium and posterior tracheal wall, superiorly by
the thoracic inlet, and inferiorly by the diaphragm
-Its contents include the heart and pericardium; the ascending and transverse aorta; the
superior vena cava (SVC) and inferior vena cava (IVC); the brachiocephalic vessels;
the pulmonary vessels; the trachea and main bronchi; lymph nodes; and the phrenic,
vagus, and left recurrent laryngeal nerves.
Findings: lymph node in
middle mediastinum
-There is right paratracheal
soft tissue mass.
10.3 Posterior mediastinal mass
-The posterior mediastinum is bounded anteriorly by the posterior trachea and
pericardium, anteroinferiorly by the diaphragm, posteriorly by the vertebral column,
and superiorly by the thoracic inlet.
-The contents include the esophagus, descending aorta, azygos and hemiazygos
veins, thoracic duct, vagus and splanchnic nerves, lymph nodes, and fat.
12. Findings: Descending aortic aneurysm in posterior mediastinum.
-There is lateral displacement of lateral margin of descending thoracic aorta
due to aortic aneurysm.
11. Atelectasis
Pattern of pulmonary collapse or atelectasis
General signs of lobar collapse
- Decrease lung volume
- Displacement of fissure
- Local increase in density of lobar collapse due to non-aerated lung
- Elevation of hemidiaphragm
- Displacement of hilar vessel
- Displacement of mediastinum
- Compensatory overinflation of adjacent lobes.
Specific sign of lobar collapse
1. RUL-Collapse upwards and anteriorly
Minor fissure
Findings:
-Opacity in right upper lung due to reduce volume of non-areated lung
-Elevation of minor fissure
-Elevation of right hilum
-Tracheal deviation to the right
13. 2. RML
Minor f
Major f
Findings:
-Increase density in right middle lung zone with loss of definition of right cardiac border
-Lateral film: triangular shape opacity projected over the heart
(Triangular shapeเกิดจากการdisplacementของminorและmajor fissureเขาหาlobar collapse)
3. LUL-Collapses upwards and anteriorly
Major fissure
Findings:
PA film
-Decrease volume with increase density of LUL
-Loss of definition of left cardiac border and of left hilum
-Elevation of left hilum
-Tracheal deviation to the left
Lateral film
-Increase opacity anteriorly (due to collapse lobe), which has well-defined posterior
margin due to left major fissure
14. 4. LLL-Collapses downwards and posteriorly
12 Abnormal infiltration
12.1 Air space/ alveolar infiltration
Findings:
-Fluffy, ill-defined areas of opacification
(เห็นเปนปุยๆที่มีขอบเขตไมชัด)
-Area of consolidation tend to coalesce
-Air bronchograms: airที่อยูในbronchus ถูก
ลอมรอบดวยconsolidated lung การเห็นair
bronchogramsนั้นบงบอกวาdieseaseนั้นอยูใน
lung parenchyma ไมใช pleura หรือ
mediastinum.
แบงออกเปน
-Segmental/lobar alveolar pattern:
DDx
-Pneumonia
-Segmental/lobar collapse
-Pulmonary infarction
-Alveolar carcinoma
-Contusion (associated with
rib fracture, pneumothorax ect)
15. -Diffuse pattern:
DDx
-Cardiogenic pulmonary edema
-ARDS
-Fluid overload
-Pulmonary hemorrhage
-Pneumonia: PCP, Mycoplasma
12.2 Interstitial infiltration
- Linear pattern
Findings: fine lines running to the
lung
-Kerley A lines.
-Kerley B lines.
(ดูในเรื่องCHF)
-Nodular pattern
Findings:
-intersitial nodules are small
(1-5mm), well-defined border
-Not associated with air
bronchograms
16. -Honeycomb pattern
-Represent end-stage of disease
-Imply extensive pulmonary
destruction.
-There are multiple cysts that
range in size from tiny up to 2 cm.
-Very thin wall cysts
-Normal vasculature cannot be
seen.
13 Pulmonary TB
-Primary TB
-Usually asymptomatic
-Heal pulmonary lesion
Findings:
-Heal tiny calcific pulmonary nodule
(Calcific granuloma at LUL)
-Heal calcific hilar lymph node
-Post-primary pulmonary TB (reactivation TB)
Findings:
-Cavitation: Thick-walled,
irregular cavity with/or
without air-fluid level
17. Findings:
-Reticulonodular infiltration at apical and posterior segment of upper lobe and
superior segment of lower lobe.
-Volume loss at both upper lobes from fibrotic change
-Calcification may occur in fibrosis
18. NEURORADIOLOGY
1.Epidural hematoma
Finings:
-There is lens shape (or biconcex
shape) hyperdensity fluid
(HU=50-100) at left parietal
region.
-Displacement of left lateral
ventricle
-Usually not cross suture except
associated with diastatic fracture
.
2. Subdural hematoma
Findings:
-There is crescentric shape
hyperdensity fluid at left
fronto-parieto-temporal region.
- Can cross suture
- Not cross falx or dura
3. Subarachnoid hemorrhage
Findings:
-There is hyperdensity fluid in
sulci and cistern (eg suprasella
cistern, sylvain cistern)
-There is intraventricular
hemorrhage
-Communicating hydrocphalus
19. 4.Hypertensive hemorrhage
Findings:
-There is hyperdensity of acute hematoma at right basal ganglia and
thalamus and extends to ventricular system (intraventricular
hemorrhage).
-Displacement of right lateral ventricle
-Midline shifting to the left side
5.Acute cerebral infarction
Findings:
-Hyperdense artery sign on noncontrast CT scan represented of
intraluminal thrombus in middle cerebral artery
20. Insular ribbon sign
Findings:
-There is wedge shape hypodensity area involving both gray
and white matter at left frontoparietal region
-Loss of gray white differentiation
-Insular ribbon sign: loss of gray white differentiation at left
insular cortex.
Findings:
-There is wedge shape of hypodensity area of both gray and white
matter at left fronto-parietotemporal region which compatible with
left MCA territory
-Pressure effect to left lateral ventricle and midline shifting
21. 6.Subacute cerebral infarction
Findings:
-There is well-defined hypodensity area at left parietal region.
-Decrease degree of pressure effect-After contrast administration reveals
gyral enhancement (abnormal enhancementตามgyri จากการสูญเสียblood brain
barrier)
7. Chronic cerebral infarction
Findings:
-There is very low density area at
right basal ganglia which compatible
with old basal ganglia infarction.
-Sign of volume loss: Ipsilateral
dilatation of right ventricular system