Peripheral Neuropathies (Guillian Barre & Myasthenia Gravis)
•Als PPT, PDF herunterladen•
41 gefällt mir•2,136 views

Peripheral Neuropathies in Critical Care Nursing

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Peripheral Neuropathies (Guillian Barre & Myasthenia Gravis)
Ähnlich wie Peripheral Neuropathies (Guillian Barre & Myasthenia Gravis) (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Peripheral Neuropathies (Guillian Barre & Myasthenia Gravis)
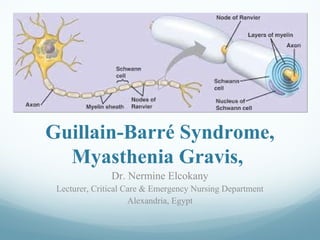
- 1. Guillain-Barré Syndrome, Myasthenia Gravis, Dr. Nermine Elcokany Lecturer, Critical Care & Emergency Nursing Department Alexandria, Egypt
- 2. Guillain-Barré Syndrome It is an acute inflammatory demyelinating polyneuropathy, is a rapidly evolving illness that commonly presents as symmetrical weakness, sensory loss, and areflexia. This condition is an inflammatory peripheral neuropathy in which lymphocytes and macrophages strip myelin from axons.
- 3. ETIOLOGY The etiology of Guillain-Barré syndrome is unclear, but an autoimmune response is strongly suspected. There is a preceding event or trigger that is often an infection. Occasionally, vaccinations have been known to trigger Guillain-Barré syndrome.
- 4. The febrile infection is usually respiratory or gastrointestinal. Other predisposing factor (surgery, lymphoma, trauma)
- 5. PATHOPHYSIOLOGY In Guillain-Barré syndrome, the myelin sheath surrounding the axon is lost. Loss of the myelin sheath in Guillain-Barré syndrome makes nerve impulse transmission is aborted. Demyelination is initiated by an antibody attack on the myelin early in the course of the disease
- 9. CLINICAL MANIFESTATIONS Muscle weakness and diminished reflexes of the lower extremities. Quadrilegia Deep tendon reflexes are usually lost, even in the earliest stages. Neuromuscular respiratory failure. Paresthesias N.B. Weakness usually begins in the legs and progresses upward.
- 10. DIAGNOSIS Signs and symptoms include- motor weakness, paresthesia. A history of a viral illness ascending weakness Declining pulmonary function capacity Lumbar puncture reveals elevated CSF protein level Electromyography (EMG) Nerve conduction studies (NCS)
- 11. CLINICAL MANAGEMENT Preventive measures need to be established to prevnt DVT and pulmonary embolism do not develop. Heparin 5000 units subcutaneously may be given along with antiembolism stockings and sequential compression devices
- 12. The first therapy proven to benefit patients with Guillain-Barré syndrome is plasmapheresis. This procedure mechanically removes humoral factors. Intravenous immunoglobulin (IVIG) is also useful in managing Guillain-Barré syndrome.
- 13. Nursing management Goals of management 1.Prevent infections and complications of immobility 2.Provide proper nutrition 3.Provide functional maintenance of body systems
- 14. Goals of management 4.Treat life threatening problems 5.Provide comfort and emotional support. 6.Patient education
- 15. Myasthenia Gravis Myasthenia gravis (from Greek "muscle", "weakness", and Latin gravis "serious"; abbreviated MG) is an autoimmune neuromuscular disease leading to fluctuating muscle weakness and fatigability. It is an autoimmune disorder, in which weakness is caused by circulating antibodies that block acetylcholine receptors at the post-synaptic neuromuscular junction, inhibiting the stimulative effect of the neurotransmitter acetylcholine.
- 16. ETIOLOGY Myasthenia gravis is an autoimmune disorder. The factors that trigger the autoimmune process are not known, but the thymus gland is involved. The thymus lies behind the sternum and may extend down to the diaphragm or up to the neck. This gland plays a role in the responsiveness of T cells to foreign antigens.
- 17. The thymus gland is large in children and small in adults. By adulthood, the gland has shrunken and has nearly been replaced by fat. Abnormalities in the thymus gland frequently occur in patients with myasthenia gravis. Eighty percent of patients with myasthenia gravis have thymal hyperplasia.
- 19. PATHOPHYSIOLOGY Myasthenia gravis is a result of circulating antibodies directed toward the skeletal muscle acetylcholine receptors. This leads to a decrease in end plate depolarization, which may be insufficient to generate an action potential. This results in a failure of the muscle to contract.
- 21. CLINICAL MANIFESTATIONS The hallmark of myasthenia gravis is fatigability. Muscles become progressively weaker during periods of activity and improve after periods of rest. Muscles that control eye and eyelid movement, facial expressions, chewing, talking, and swallowing are especially susceptible. The muscles that control breathing and neck and limb movements can also be affected.
- 24. Symptoms, which vary in type and severity, may include asymmetrical ptosis (a drooping of one or both eyelids), diplopia (double vision) due to weakness of the muscles that control eye movements, an unstable or waddling gait, weakness in arms, hands, fingers, legs, and neck, a change in facial expression, dysphagia (difficulty in swallowing), shortness of breath and dysarthria (impaired speech).
- 25. In myasthenic crisis a paralysis of the respiratory muscles occurs, necessitating assisted ventilation to sustain life. In patients whose respiratory muscles are already weak, crises may be triggered by infection, fever, an adverse reaction to medication, or emotional stress. Since the heart muscle is only regulated by the autonomic nervous system, it is generally unaffected by MG.
- 26. DIAGNOSIS patient’s history Patients may present with complaints of double vision or drooping eyelids. Also, myasthenia gravis causes weakness of the shoulder girdle muscles.
- 27. The cranial nerve examination may reveal ptosis and diplopia Motor weakness may be exhibited Blood is drawn for acetylcholine receptor antibodies Electromyography (EMG)
- 28. CLINICAL MANAGEMENT • The clinical management of myasthenia gravis includes the following strategies: 1.use of medications to enhance neuromuscular transmission; such as anticholinesterases (Pyridostigmine (Mestinon), and steroids (Prednisone)
- 29. Long-term immunosuppression with corticosteroids, azathioprine (Imuran), cyclophosphamide (Cytoxan), or cyclosporine; Short-term immunomodulation with plasmapheresis or IVIG; or thymectomy.
- 30. Nursing management 1. Assessment 2. Provide proper nutrition 3. Provide functional maintenance of body systems 4. Provide comfort and emotional support. 5. Patient education
- 31. THANK YOU