pelvis finjury
•Als PPTX, PDF herunterladen•
6 gefällt mir•3,647 views

pelvis injury Taiz University,faculty of medicine and health sciences By Dr : Afrah Alalemi

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (11)
Ähnlich wie pelvis finjury
Ähnlich wie pelvis finjury (20)
Mehr von MONTHER ALKHAWLANY
Mehr von MONTHER ALKHAWLANY (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
pelvis finjury
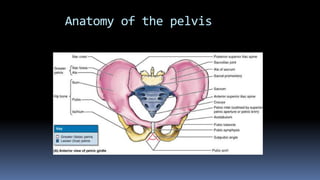
- 1. Anatomy of the pelvis
- 2. Anatomy of the pelvis The pelvic ring is made up of the twoinnominate bones and the sacrum, articulating in front at the symphysis pubis (the anterior or pubic bridge) and posteriorly at the sacroiliac joints (the posterior or sacroiliac bridge).
- 3. Anatomy of the pelvis
- 5. Ligaments of the Pelvic Girdle
- 7. Introduction Fractures of the pelvis account for less than 5 per cent of all skeletal injuries, but they are particularly important because of the high incidence of associated soft tissue injuries and the risks of severe blood loss, shock, sepsis and adult respiratory distress syndrome (ARDS). Like other serious injuries, they demand a combined approach by experts in various fields. About two-thirds of all pelvic fractures occur in road accidents involving pedestrians; over 10 per cent of these patients will have associated visceral injuries, and in this group the mortality rate is probably in excess of 10 per cent.
- 8. Mechanism of injury Low-Energy Fractures Pelvic fractures resulting from low-energy mechanisms are usually fractures of individual bones of the pelvic ring that do not damage the true integrity of the ring structure. Example:postmenposaul,steroid induced,postirradation,congenitialand metabolic bone disease, fall from ground level. High-energy trauma also results in more severe injury to the pelvic ring, associated soft tissues, and viscera. Although high-energy mechanisms can produce isolated fractures, they most often result in two or more fractures of the pelvic ring. Example:motor vehical accidient,industrial incident,sporting event;fall from the hight greaterthan6ft ,crashing injery, gun shotinjery.
- 9. High-energy trauma ASSOCIATED HEMORRHAGEAND IMPLICATIONS FOR THERAPEUTIC INTERVENTION At the time of a traumatically induced pelvic fracture, some degree of hemorrhage is inevitable.The principal sites of bleeding are outlined inTable 1.The anticipated sites of major hemorrhage correlate with the region of the pelvis fracture, the vector of the provocative blow, and the magnitude of pelvic displacement.
- 10. High-energy trauma Principal Sites of Hemorrhage after a Pelvic Fracture Interossoeuos vasseles Periosteal sub capsulare , adjecent intra mascular vasseles Intrapelvic Gulteal vasseles Obturatorvassles Pudendal hypogastric External and internal illiac Common illiac and aorta Intra abdominal bleeding Visceral bleeding Majer abdominal bleeding
- 12. NEUROLOGIC INJURIES WITH PELVIC TRAUMA Lumbosacral plexus Presacral plexus Sciatic nerve Femral nerve Other motor nerve around the pelvis(eg:gulteal,pudendal,obturator) Lateral femoral cutaneuse nerve of the thigh Genitofemoral,illioinguinal nerve Lumbosacral nerve root
- 13. NEUROLOGIC INJURIES WITH PELVIC TRAUMA
- 14. VISCERAL INJURIES WITH PELVIC TRAUMA Intraabdominal Intrapelvic: Small and larg bowel. Urinary:urethera and bladder25% Genital:vaginal,occasionally other
- 15. Pelvic stability The crucial stabilizing ligaments extend from the sacrum, across the sacroiliac (SI) joints and posterior; they transmit weight- bearing forces either across the hip joints, into the lower extremities for ambulation, or into the ischial tuberosities for sitting.The crucial posterior SI ligaments stabilize the SI joints, along with the iliolumbar, sacrospinous, and sacrotuberous ligaments.With its ring-like configuration, the pelvis is intrinsically highly stable and resistant to deforming forces.
- 16. Pelvic stability
- 17. Pelvic instability If the pelvis can withstand weightbearing loads without displacement, it is stable; this situation exists only if the bony and key ligamentous structures are intact.
- 18. Pelvic instability Pelvic instability If the pelvis can withstand weightbearing loads without displacement, it is stable; this situation exists only if the bony and key ligamentous structures are intact. Determinants of Pelvic Instability The characteristic patterns of pelvic disruption correlate with the vector and magnitude of the provocative blow and the strength of the pelvic ring . Subtle changes in the force vector markedly alter the pattern of the disruption.A direct lateral blow on the posterior ilium usually causes a stable lateral compression injury with impaction of the sacral ala, and accompanying unilateral or bilateral ramus fractures. A blow to the anterior portion of the lateral ilium results in an internal rotational moment that creates an unstable injury in which the ilium sustains a vertical or crescent fracture with the sacral ala acting as a fulcrum (69).With the rotational deformity of the ipsilateral hemipelvis, the sharp edges of the ramus fractures can impale the bladder or occasionally the bowel.
- 19. defination pelvic Stable:lesion sparing the pasterior arch;pelvic floor intactand able to withstand normal physiological stresses without displacement. Partially Stable:pasterior osteoligamentous integrity partially maintained and pelvic floor intact Unstable :complete loss of osteoligamentous integrity and pelvic floor disrupted Pelvic ring:has tow arch(a)pasterior arch is behind acetabular surface includes sacrum’sacroilliac joint and ther ligament and pasterior illium (b)Anterior arch infrot of acetabular surface and includes pubic rami bone and symphseal joint
- 20. Classification PENNALANDTILE CLASSIFICATION Pennal and associates (50) classify the principal pelvic ring disruptions based on the direction of the injuring force and the degree of pelvic disruption TYPE A Stable A1—Fractures of the pelvis not involving the ring A2—Stable, minimally displaced fractures of the ring TYPE B Rotationally unstable, vertically stable B1—Open book B2—Lateral compression: ipsilateral B3—Lateral compression: contralateral (bucket- handle) TYPE C Rotationally and vertically unstable C1—Rotationally and vertically unstable C2—Bilateral C3—Associated with an acetabular fracture
- 21. TYPE A Stable A1—Fractures of the pelvis not involving the ring (1)Avulsion fractures A piece of bone is pulled off by violent muscle contraction; this is usually seen in sportsmen and athletes. The sartorius may pull off the anterior superior iliac spine, the rectus femoris the anterior inferior iliac spine, the adductor longus a piece of the pubis, and the hamstrings part of the ischium
- 23. managment All are essentially muscle injuries, needing only rest for a few days and reassurance. Pain may take months to disappear and, because there is often no history of impact injury, biopsy of the callus may lead to an erroneous diagnosis of a tumour. Rarely, avulsion of the ischial apophysis by the hamstrings may lead to persistent symptoms, in which case open reduction and internal fixation is indicated
- 24. Direct fractures Fracture of the ilium Fracture of the ischium Fracture of the pubic ramus
- 25. ANTEROPOSTERIOR COMPRESSION (APC) INJURIES ‘open book’ (1)APC-I injuries: there may be only slight (less than 2 cm) diastasis of the symphysis; however, although invisible on x-ray, there will almost certainly be some strain of the anterior sacroiliac ligaments. The pelvic ring is stable.
- 27. (2)APC-II injuries diastasis is more marked and the anterior sacroiliac ligaments (often also the sacrotuberous and sacrospinous ligaments) are torn. CT may show slight separation of the sacroiliac joint on one side. Nevertheless, the pelvic ring is still stable.
- 28. APC-III injuries the anterior and posterior sacroiliac ligaments are torn. CT shows a shift or separation of the sacroiliac joint; the one hemi-pelvis is effectively disconnected from the other anteriorly and from the sacrum posteriorly.The ring is unstable.
- 29. (b2)LATERAL COMPRESSION (LC) INJURIES Type B2-1: Lateral compression (internal rotation) force implodes hemipelvis. Rami may fracture anteriorly, and posterior impaction of sacrum may occur, with some disruption of posterior structures, but partial stability is maintained by intact pelvic floor and compression of sacrum.
- 30. LC-I injury. The ring is stable.
- 31. LC-II injury is more severe; in addition to the anterior fracture, there may be a fracture of the iliac wing on the side of impact. However, the ring remains stable.
- 33. LC-III injury is worse still. Due to lateral compression force on one iliac wing results in an opening anteroposterior force on the opposite ilium, causing injury patterns typical for that Mechanism.
- 35. vertical shear injury With a vertical shear injury, the iliolumbar ligaments, along with the posterior SI ligaments, are disrupted .With vertical displacement of the pelvis, the ipsilateral lower lumbar transverse processes are fractured.
- 37. Diagnosis History Suspected in high energy injury The main symptom Numbness or tingling in the groin or legs abdominal pain Groin pain (get warse when walking or moving) Difficulty urinating Difficulty walking Unable to stand Blood at the external meatus
- 38. Diagnosis look: My reveal ecchymosis or abrasions of the pelvis, back and buttocks Grey Turner's sings: A discoloration of the flanks is indicative of retroperitoneal hematoma. Destot's sign: A hematoma over the inguinal ligament, proximal thigh, perianal or scrotal areas. When inspecting the perineum may note the presence of blood at the anus or urethral meatus
- 40. feel: The bone pelvis my demonstrate tenderness or instability. A palpable fracture line or pelvis hematoma Pelvic springing: is performed by applying alternative compression and distraction forces to the iliac wings in order to detect crepitance or instability. The presence of blood on rectal and vagina examination is important, as displaced fracture me cause mucosal disruption. Perineal butterfly hematoma: Presence of haematoma highly specific for urethral disruption.
- 41. mesure Leg length: Examination of the leg is an important part of the physical examination in pelvis fracture. Adduction/abduction of the hip internal/external hip rotation that demonstrates instability. Pain or crepitus indicates involvement at or near acetabulum. FABER test: for the pubic ramus fracture patients experience groin pain when they place the ipsilateral foot on the contralateral knee and the ipsilateral hip is Flexed, Abducted and Externally Rotated. .examination of visceral injury
- 42. Radiographs: Every poly trauma patient should have Lateral c-spine Chest AP Pelvis AP pelvis is done to detect major (and potentially life- threatening) pelvic injury.
- 43. Plain Pelvic X-rays AP views 90% of all traumatic injuries to the bony pelvis were diagnosed on Anteroposterior veiw alone
- 44. Inlet view Caudal view in the 40-degree inlet. The inlet view demonstrates rotational deformity or anteroposterior displacement of one hemipclvis
- 45. Outlet view: Cephalic view in 40-degree outlet views the outlet view demonstrates vertical displacement of a hemipelvis
- 46. CT scan Is an essential part of the evaluation in pelvis fracture. It allows evaluation of the posterior portion of the pelvic ring that may be poorly appreciated on standard roentgenograms. Before the widespread use of CT scanning. many pelvic fractures were assumed. to be purely anterior injuries, although isolated anterior lesions actually are rare. CT scanning demonstrates rotational and anteroposterior displacement much better than plain roentgenograms, although vertical dispiacement is still better appreciated on roentgenograms than on axial CT images. Magnetic Resonance Imaging (MRI) Indicate that magnetic resonance imaging may provide clinically useful information with regard to genitourinary tract injuries.
- 47. Management of major pelvic fracture: You have to call orthopaedic surgeon, a urologist, a vascular surgeon, a colo-rectal surgeon and (sometimes) a gynaecologist!
- 48. Management I 1. Prehospital- transport with bed sheet, MAST, pelvic clumps. ) 3..
- 49. Initial management in the ER: Safe life Made during primary survey. Airway with c-spine control. Breathing (oxygen). Circulation IV access Crystalloid Control external loss Evaluation of intra-abdominal bleeding Look for major pelvic injury
- 50. Safe the limp The objectives of treatment for pelvic ring injuries include: Restoring bony anatomy. Preventing deformity. Minimizing discomfort. Facilitating return of' mobility and function.
- 51. minor fracture [ stable ] bed rest, Painkiller Physical therapy Healing take 8-21 wk
- 52. Severe injuries These injuries often require extensive surgery as well as lengthy physical therapy and rehabilitation .
- 53. External fixation 1. Advantages It helps tamponade bleeding from bone edges . Stabilizing the clots and the bone. Could be done in 20 min. 2. Disadvantages Can’t stop arterial bleeding. Delay the embolization for ongoing arterial hemorrhage. Degrade the quality of CT and angiograghy.
- 54. Fracture reduction and stabilization with external fixation
- 55. Timing of surgery Reduction may be easiest in first 24-48 hoursMay aid in percutaneus reduction
- 56. Reduction tools Traction Pelvic manipulator (e.g. femoral distractor) Specialized clamps
- 57. Reduction and Fixation: SI Joint Dislocation SI screw
- 60. Complications of high-energy pelvic fractures Complication of pelvis fracture result from associated injury the most complications: Pulmonary distress syndrome. Sciatic nerve injury Fat embolism Pneumonia Urinary tract infection Wound infection sepsis Coagulopathy and pulmonary embolism Paralytic ileus
- 61. Genitourinary GU complications occur in up to 37% of patients with pelvic ring injuries.65The most common GU complications occurring with pelvic ring injuries are bladder disruptions and ureteral disruptions, particularly in male patients. Less commonly, the ureters and kidneys may be injured.Dyspareunia and erectile dysfunction occur in approximately 29% of patients with pelvic ring injuries. Dyspareunia usually is caused by a displaced ramus fracture, causing pressure on the vaginal vault . Erectile dysfunction can have many causes, including vascular injury, neurologic injury, and psychological stress. A patient with erectile dysfunction should be referred to a urologist for evaluation and treatment.
- 62. Post operative complication Bed sores DVT prophylaxis is important postoperatively and should be managed aggressively. Mechanical methods, such as support stockings, work to decrease venous stasis, thereby decreasing the risk of DVT formation.
- 63. Thank you for listening