2. Sharma et al Valve Disease 665
elimination of smallpox and poliomyelitis in the world by Coronary Arteriography. Sones and colleagues22 obtained
vaccines. a selective coronary arteriogram by inadvertently engaging
the right coronary artery during an aortogram. Subse-
quently, coronary arteriography became routine in clinical
THE SECOND HALF OF THE TWENTIETH CENTURY practice but required arterial cutdown. The development of
Patient Assessment a percutaneous arterial access
Pressure Measurement. Efforts technique by Seldinger16 and of
to quantify the severity of valvular preformed catheters by Judkins23
CLINICAL SIGNIFICANCE
heart disease began in 1945 with made coronary arteriography fea-
attempts to measure intracardiac ● The diagnosis and assessment of the se- sible for widespread use. The data
pressures. In landmark studies, verity of valve stenosis and regurgitation obtained by catheterization, ven-
13
Hellems et al and Lagerlöf and are at an advanced level of accuracy. tricular and aortic angiography,
14
Werkö documented that pres- and selective coronary arteriogra-
● Interventional therapy in patients with phy are the foundation for evalu-
sures recorded with a cardiac cathe-
ter wedged into the distal pulmonary valvular heart disease results in an im- ation of valvular heart disease.
artery reflected left atrial pressure. provement of symptoms, functional class,
Ross15 developed the transseptal left ventricular function, and pulmonary Doppler Echocardiography and
approach to the left ventricle. Per- hypertension. Survival is improved in Ultrasonography. Edler and
cutaneous transthoracic puncture many patients. Hertz,24 using ultrasonography,
of the left ventricle was used to first recorded the movement of
● All patients should be considered poten- cardiac structures in 1953. Early
measure left ventricular pressure in
aortic stenosis. Subsequently, the tial candidates for interventional therapy M-mode echocardiography was
Seldinger16 technique for percuta- and should undergo appropriate clinical effective in the diagnosis of mitral
neous entry into a systemic artery evaluation and diagnostic testing. stenosis; 2-dimensional echocar-
revolutionized retrograde access diography allowed for real-time
to the ascending aorta and left visual morphologic evaluation of
ventricle. cardiac structure and function. Su-
perimposition of Doppler by Hatle and colleagues25 allowed
Valve Area Calculations. By comparing hydraulic systems for indirect hemodynamic measurement. Transesophageal
and cardiac physiology, Gorlin and Gorlin17 derived the echocardiography increased the clarity and accuracy of a
following formula for calculating mitral and aortic valve number of valvular heart diseases.
areas: Echocardiography/Doppler permitted the rapid initial as-
sessment of patients with mild, moderate, or severe valvular
CO/HR DFP
mitral valve area heart disease. It also was of great value not only in diag-
37'.9' gradient nosing unsuspected lesions but also in excluding disease.
Along with the chest x-ray and the electrocardiogram, echo-
CO/HR SEP' cardiography/Doppler has become an essential component
aortic valve area
44'.3' gradient' of the clinical evaluation of patients with valvular heart
disease. Computed tomography, electron beam computed
where CO cardiac output, HR heart rate, DFP tomography, and cardiac magnetic resonance imaging have
diastolic filling period, and SEP systolic ejection period. not been proven superior to echocardiography/Doppler for
this purpose.
Angiography. The first angiocardiogram in humans was
18
performed by Castellanos and colleagues. Aortography
and left ventricular angiography were essential to assessing INDIVIDUAL LESIONS
aortic and mitral regurgitation. Dodge and colleagues19 ac-
curately calculated the left ventricular volumes and ejection Mitral Stenosis
fraction from left ventricular angiograms using Arvidsson’s In 1954, the outstanding clinical cardiologist and scholar
technique. Paul Wood26 described the clinical features, pathophysiol-
ogy, complications, and outcomes of mitral stenosis. He
Normal Values. Values for right-sided heart pressures, pul- documented that, on average, the symptoms of mitral ste-
monary artery wedge pressure, and cardiac output were nosis began 19 years after rheumatic carditis.
documented in healthy volunteers.20 Another study in As early as the 1920s, but mainly in the early 1950s,
healthy subjects documented right and left-sided heart pres- mitral commissurotomy was performed by manual dilata-
sures and left ventricular volumes and ejection fraction.21 tion (“finger fracture”).27 Later in the 1950s, the results
The normal cardiac index was found to be 3.6 0.9 were improved by using the Tubbs’ dilator, which is intro-
L/min/m2. duced from the left ventricular apex. Both of these proce-
3. 666 The American Journal of Medicine, Vol 121, No 8, August 2008
dures were “blind” (closed). When performed by a skilled, Table 2 Procedural Advances in Valvular Heart Disease
experienced surgeon on an appropriate patient, closed mitral
commissurotomy had an excellent outcome; the survival Discoveries by 6 Nobel Laureates who have had an impact on
was better than that of medical therapy (Figure 2),28 and the valvular heart disease
24-year survival was 84%.27 The next development was Identification of the infecting organism of rheumatic fever
“open” mitral commissurotomy, which incorporated extra- Establishment of databases
Performance of randomized clinical trials
corporeal circulation. However, in skilled surgical hands,
Measurement of intracardiac pressures and calculation of valve
the results of closed and open mitral commissurotomies areas
were similar.29 In the early 1960s, mitral valve replacement Left ventricular angiography, aortography, coronary
provided excellent results for those patients who were poor arteriography
candidates for surgical commissurotomy.30 Echocardiography/Doppler
The 1980s ushered in the era of catheter balloon com- Total cardiopulmonary bypass for intracardiac surgery
missurotomy; the double balloon technique was followed by Cardiac Surgery:
the Inoue balloon (Toray Medical Co, Ltd), which is still in Commissurotomy
current use. In randomized trials, catheter balloon commis- Prosthetic heart valves
surotomy yielded outcomes at least as good as those ob- Valve repair
tained from closed or open surgical commissurotomy.31 Robotic surgery
Coronary artery bypass graft surgery
All 3 procedures yield the best results for mobile and
Percutaneous catheter intervention for coronary artery
disease
Catheter balloon commissurotomy
Table 1 Nobel Prize and Lasker Award-winning
Achievements Relevant to Valvular Heart Disease
Wilhelm Conrad Röntgen The Nobel Prize in Physics 1901
“In recognition of the extraordinary
services he has rendered by the
discovery of the remarkable rays Table 3 Accomplishments in Valvular Heart Disease
subsequently named after him”
Alexis Carrel The Nobel Prize in Physiology or Virtual elimination of rheumatic valve disease in developed
Medicine 1912 countries
“In recognition of his work on Reduction of rheumatic fever, rheumatic fever recurrences, and
vascular suture and the rheumatic valve disease in developing countries
transplantation of blood vessels Recognition of drug-induced valve disease
and organs” More accurate diagnosis of valve disease and assessment of
Willem Einthoven The Nobel Prize in Physiology or their severity
Medicine 1924 Significantly better assessment of severity of valve diseases
“For his discovery of the mechanism Definition of valvular abnormality/pathology
of the electrocardiogram” Correction of valve abnormality/pathology
Gerhard Domagk The Nobel Prize in Physiology or Relief of mitral stenosis by percutaneous catheter technique
Medicine 1939 Appropriate selection of valve replacement device and procedure
“for the discovery of the antibacterial resulting in improvement of symptoms, functional status,
effects of prontosil”* left ventricular function, pulmonary hypertension, and
Sir Alexander Fleming, The Nobel Prize in Physiology or survival
Ernst Boris Chain, Sir Medicine 1945
Howard Walter Florey “for the discovery of penicillin and its
curative effect in various infectious
diseases”
André Frédéric The Nobel Prize in Physiology or
Cournand, Werner Medicine 1956 Table 4 Recurrence of Rheumatic Fever*
Forssmann, Dickinson W. “for their discoveries concerning
Richards heart catheterization and Per Compliance
pathological changes in the Year, % Rate, %
circulatory system” Benzathine penicillin, 1.2 million 0.4 94
Albert Starr, Alain Albert Lasker Clinical Research Award (intramuscular) every 4 wk
Carpentier 2007 Oral penicillin G, 200,000 U once daily 5.5 50
“Surgeon-scientists who Sulfadiazine, 1 g/d 2.8 50
revolutionized the treatment of
*Data from Alban B, Epstein JA, Feinstein AR. Rheumatic fever in
heart disease”
children and adolescents: a long-term epidemiologic study of subsequent
*Protonsil was the first synthetic drug used for treatment of general prophylaxis, streptococcal infection and clinical sequelae. Ann Intern
bacterial infections in humans. Med. 1964;60(Suppl 5):1-129.
4. Sharma et al Valve Disease 667
matic fever and carditis: On average, symptoms of aortic re-
Reported Rheumatic Fever, Denmark, 1862-1962 gurgitation began 20 years after the occurrence of carditis.
300 The incidence of death, angina, or heart failure was 87% at
200
6 years in the high-risk group and 8% at 15 years in the
low-risk group.32 In the current era, aortic regurgitation is
MORBIDITY PER 100,000
Penicillin usually the result of aortic root dilation with echocardiog-
100
raphy/Doppler used to study the natural history.31 Of
asymptomatic patients with normal left ventricular ejection
50
fraction, approximately 3% to 6% per year become symptom-
atic or progress to left ventricular dysfunction; more than one
quarter of patients with left ventricular dysfunction become
20
symptomatic per year; and the mortality for symptomatic
patients is more than 10% per year. In addition, echocar-
10
1860 ‘70 ‘80 ‘90 1900 ‘10 ‘20 ‘30 ‘40 ‘50 ‘60 ‘70 diographic data for left ventricular dimensions show that an
YEAR
end-diastolic dimension of 70 mm ( 35 mm/m2) or an
end-systolic dimension of 50 mm ( 25 mm/m2) increases
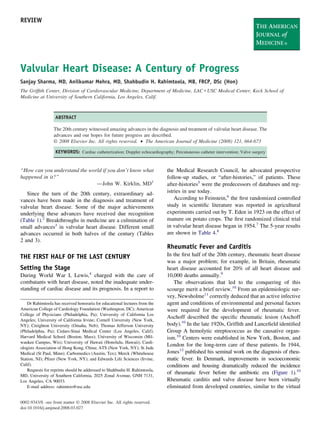
Figure 1 Incidence of rheumatic fever in Denmark from 1862
to 1962. From the Public Health Board of Denmark, Copenha- the chance that a patient will become symptomatic or de-
gen, Denmark. This is a log scale; from 1860 to 1945 morbidity velop left ventricular dysfunction.31 Left ventricular dys-
decreased by approximately 75%. The time when penicillin was function precedes the development of symptoms in more
available for clinical use (arrow). Adapted from Stollerman GH. than half of asymptomatic patients.31,33
Rheumatic Fever and Streptococcal Infections. New York: Arteriolar dilators were shown to have beneficial effects
Grune & Stratton, Inc. 1975;21-146. on hemodynamics and left ventricular size during 1 year of
follow-up. These data set the stage for a randomized trial
documenting that long-acting nifedipine reduced or de-
nonthickened or mildly thickened valves. Catheter bal- layed the need for aortic valve replacement in asymp-
loon commissurotomy is now the first-line treatment for tomatic patients with normal left ventricular ejection
mitral stenosis.30 fraction (Figure 3).33 In all symptomatic patients, aortic
valve replacement was shown to have beneficial effects on
Aortic Regurgitation symptoms, as well as left ventricular size and function, even
Most patients described in the after-histories of Lewis4 had when baseline left ventricular systolic function was abnor-
chronic aortic regurgitation. There were 3 eras.32 The era of mal;34 minimally symptomatic and asymptomatic patients
syphilis: The data are largely from the preantibiotic era; with mild left ventricular dysfunction have the best out-
syphilitic cardiovascular disease is now rare. The era of rheu- comes from the procedure.35
MITRAL STENOSIS MITRAL STENOSIS
(Functional Class II) (Functional Class III & IV)
Figure 2 Closed mitral commissurotomy is associated with better survival than medical
therapy in patients with severe mitral stenosis who were mildly symptomatic (left) and
severely symptomatic (right). Adapted from Roy SB, Gopinath N. Mitral stenosis. Circu-
lation. 1968;38(suppl V):68-76.
5. 668 The American Journal of Medicine, Vol 121, No 8, August 2008
occur in older patients. Atherosclerosis and inflammation
are important factors in the complex cause of calcific aortic
stenosis.36,37 The life expectancy of patients has markedly
increased; calcific aortic stenosis is now the most common
reason for valve replacement.
In 1968, an analysis of autopsy data showed a 3-year
average life expectancy for symptomatic patients with se-
vere aortic stenosis.38 Twenty years later, a follow-up study
after cardiac catheterization confirmed the short life expect-
ancy.39 In both studies, life expectancy after the onset of
heart failure was only 1 to 2 years.
In the 1970s, the importance of correcting aortic valve
areas for body size was recognized.40 Severe aortic stenosis
was diagnosed as aortic valve areas of 1.0 cm2 or less ( 0.6
cm2/m2);41 more recently, severe aortic stenosis was defined
as an aortic valve area of 0.7 cm2 or less ( 0.4 cm2/m2). A
Figure 3 Long-acting nifedipine administered twice daily re- mean aortic valve gradient of 50 mm Hg or more is usually
sults in a lower incidence of the need for aortic valve replace-
a reliable indicator of severe aortic stenosis.42
ment in asymptomatic patients with chronic severe aortic regur-
gitation and normal left ventricular ejection fraction. From In symptomatic patients with severe aortic stenosis, aor-
Scognamiglio R, Rahimtoola SH, Fasoli G, et al. Nifedipine in tic valve replacement has a beneficial effect on symptoms,
asymptomatic patients with severe aortic regurgitation and nor- left ventricular function, left ventricular hypertrophy, and
mal left ventricular function. N Engl J Med. 1994;331:689-695. survival (Figure 4).39,43 It also markedly improves symp-
PTS patients; AR aortic regurgitation; LV left ventricular. toms in patients with severe aortic stenosis and clinical heart
failure; if patients have no history of myocardial infarction
and the procedure is performed early, the left ventricular
Aortic Stenosis ejection fraction normalizes in one half to two thirds of
Most cases of severe aortic stenosis currently seen in de- patients (Figure 5).44 These positive outcomes also occur in
veloped countries are calcific (so-called degenerative) and patients with aortic stenosis, low aortic valve gradients, and
operated operated
non-operated
non-operated
non-
A B
Figure 4 Survival is better after aortic valve replacement (operated) than with medical
therapy (non-operated) in patients with severe aortic stenosis. A: Adapted from Schwarz F,
Banmann P, Manthey J, et al. The effect of aortic valve replacement on survival. Circu-
lation. 1982;66:1105-1110. B: Adapted from Horstkotte D, Loogen F. The natural history
of aortic valve stenosis. Eur Heart J. 1988;9(suppl E):57-64.
6. Sharma et al Valve Disease 669
a complication of the dilated orifice and diseased valve. The
subsequent results depend on the degree of the exhaustion
AVR FOR AS IN HEART FAILURE of the muscle of the heart. The backward pressure resulting
1.0 from the regurgitation embarrasses the left auricle, pulmo-
nary circulation, and right heart.” These observations, made
in 1908, are valid even now.
0.9 mean ± SE The incidence of mitral regurgitation in patients with
rheumatic valve disease was documented to be 34%.9 In
0.8 the late 1950s, ruptured chordae tendineae were recog-
nized as the cause of acute mitral regurgitation. At the
EJECTION FRACTION
0.7 1958 Goulstonian Lecture, Leatham47 gave his classic
presentation on auscultation of the heart. However, he
thought that late systolic sounds were pericardial/pleural
0.6
in origin and that the accompanying murmur was
“innocent” (Figure 16 in his article).47 Also in 1958,
0.5
McKusick48 wrote a treatise on cardiovascular sounds,
describing in considerable detail a “musical pleural peri-
0.4 cardial murmur” often preceded by a click. He noted that
this sound had been described earlier, first in 1843 in
0.3 patients with valves later determined at autopsy to be
“normal,” and then in 1880 by Osler.48
In 1963, on the basis of autopsy findings, Barlow and
0.2
colleagues49 described mitral valve prolapse as a cause of
these sounds. Subsequently, mitral valve prolapse was
0.1 P<0.001 diagnosed clinically by left ventricular angiography.
Echocardiography/Doppler represented a major advance
0 that not only provided evidence of the causes of mitral
Pre-Op Post-Op regurgitation, including mitral valve prolapse, and the
Peri-Op MI and late CHB
pathophysiologic changes associated with mitral regurgi-
Post-Op: Perivalvular Aortic Regurgitation tation, but also showed that mitral valve prolapse is
common and the most common cause of ruptured chordae
Figure 5 Left ventricular ejection fraction improves and even tendineae, which became known as “flail leaflets.” Mitral
normalizes after aortic valve replacement in approximately two regurgitation also can be caused by coronary artery dis-
thirds of patients with severe aortic stenosis and clinical heart ease because of its effect on the left ventricle. Recently,
failure. Adapted from Smith N, McAnulty JH, Rahimtoola SH. some drugs also have been shown to cause valvular
Severe aortic stenosis with impaired left ventricular function regurgitation.50
and clinical heart failure. Results of valve replacement. Circu- Symptomatic patients with severe mitral regurgitation
lation. 1978;58:255-264. AVR aortic valve replacement; SE
benefited from mitral valve replacement or repair. In asymp-
standard error; MI myocardial infarction; CHB com-
plete heart block. tomatic patients, mitral valve replacement or repair can be
deferred until the onset of symptoms or evidence of left
ventricular dysfunction, pulmonary hypertension, or atrial
fibrillation.51
severe left ventricular dysfunction if they have severe aortic
stenosis.45 Tricuspid Valve Disease
In 1908 Mackenzie46 observed, “Although actual disease
Mitral Regurgitation of the valves is rare, incompetence of the tricuspid orifice
In the early 1900s, mitral regurgitation was the most is extremely common . . . It should never be concluded
commonly diagnosed valve lesion. At that time, physi- that no tricuspid regurgitation occurs because of the ab-
cians were strongly discouraged from overdiagnosing sence of a murmur . . . A weak muscular wall and wide
organic mitral regurgitation, thus saving healthy subjects orifice may give rise to no murmur.” These observations
from invalidism.9 remain relevant even today, and good methods for repair-
Mackenzie46 was well aware of the spectrum of the ing or replacing tricuspid valves are still lacking. There is
clinical aspects of mitral regurgitation, writing, “The really a great need for improvements in surgical techniques,
serious trouble in connexion with mitral regurgitation arises replacement valves, and assessment of patients for
when the muscle is impaired and the regurgitation is due to surgery.
7. 670 The American Journal of Medicine, Vol 121, No 8, August 2008
Starr-Edwards
Starr- St. Jude
100 100
90 90
80 80
vent-free urvival (%)
70 70
Survival (%)
60 60
50 50
40 40
S
n=122 n=113 n=104 n=93 n=75 n=59 n=38 n=21 n=112 n=101 n=85 n=75 n=55 n=42 n=25 n=12
30 30
20 20
E
n=118 n=110 n=102 n=90 n=78 n=60 n=44 n=24 n=106 n=92 n=83 n=72 n=59 n=45 n=32 n=17
10 10
0 0
0 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 8
Time after operation (years) Time after operation (years)
Figure 6 Survival (left) and event-free survival (right) after aortic valve replacement with Starr-Edwards valve (Carpentier-Edwards,
Irvine, Calif) and St Jude valve (St Jude Medical Inc, St Paul, Minn). Data with mitral valve replacement were similar. Adapted with
permission from Murday AJ, Hochstizky A, Mansfield J, et al. A prospective controlled trial of St. Jude versus Starr Edwards aortic and
mitral valve prostheses. Ann Thorac Surg. 203;76:66-74.
SURGERY resumed an active life; 1 patient is known to have survived
another 31 years. This epochal event was followed in 1963
Open Heart Surgery and 1964 by an astounding surgical accomplishment dem-
In 1954, John Gibbon Jr52 described the use of total cardio- onstrating that valve replacement could be “safe.” McGoon
pulmonary bypass for intracardiac surgery. This had an et al55 replaced native aortic valves with Starr-Edwards
enormous impact on valve surgery and completely changed valves (Edwards Life Sciences, Irvine, Calif) in 100 con-
its performance. Valve surgery has been the most important secutive patients, most of whom were in severe heart fail-
advance in the treatment of symptomatic patients with se- ure, and all of the patients survived. Since 1960, Starr and
vere valve disease. Valve surgery markedly improves func- colleagues have used the Starr-Edwards valve in 3653 pa-
tional class, hemodynamics, and left ventricular function. It tients, 1 of whom survived 41 years.56 After improvements
also has improved survival in patients with severe aortic or to the original model in 1965, the Starr-Edwards valve has
mitral valve stenosis (Figures 2 and 4), and probably has remained virtually unchanged, and no structural valve de-
improved survival in symptomatic patients with severe aor- terioration has yet been observed. A randomized trial has
tic or mitral regurgitation. shown that Starr-Edwards and newer St Jude (St Jude Med-
ical Inc, St Paul, Minn) valves yield equally favorable
outcomes up to 8 years of follow-up (Figure 6).57
Valve Replacement Xenografts (heterografts) were first used in 1965 by
Prosthetic heart valves are mechanical or biological. Bio- Carpentier et al,58 who coined the term “bioprosthesis.”59
logical valves can be derived from patient tissues (au- Ross60 used autografts in 1967.
tografts) or donor tissues (allografts, called homografts), or Procedures involving stentless bioprostheses, homografts,
can be valves taken from another species (xenografts, called or the “Ross principle” require aortic root replacement with
“bioprosthesis”). reimplantation of coronary arteries, which poses a problem
Mechanical prosthetic heart valves were used in 1960 by if reoperation is needed. Furthermore, data from more
Harken and Starr. It was the initial results obtained by Starr than 400,000 patients from the Society of Thoracic Sur-
and Edwards53,54 that changed the scene. Of Starr and gery database have shown that the operative mortality for
Edwards’ first 8 patients, all of whom were in advanced these procedures is approximately twice that for stented
heart failure, 6 survived to leave the hospital and several bioprosthesis.61
8. Sharma et al Valve Disease 671
The 2 largest randomized trials, the Edinburgh Heart
Valve trial62 and the Veterans Administration trial,63 com-
pared a mechanical valve (original Delron-ring Bjork-
Shiley valve [Shiley Labs, Irvine, Calif]) with a porcine
bioprosthesis (Figures 7 and 8). The findings were similar:
There was no significant difference in survival over 20
years with 1 exception (discussed below); there were no
significant differences in thromboembolism, infective en-
docarditis, or all-cause complications; the mechanical
valves did not deteriorate, but they had a higher rate of
bleeding; and the bioprosthetic valves deteriorated at an
increasing rate. Only the Veterans Administration trial, in
which a larger number of patients underwent aortic valve
replacement, showed a higher mortality for the porcine
valve because of structural deterioration; however, no Figure 8 Department of Veterans Affairs trial of valvular
deterioration was observed in patients who were at least heart disease. Fifteen-year survival after aortic valve replace-
65 years old at the time of valve replacement. ment is better with a mechanical valve than with a bioprosthetic
The current choice is usually a mechanical valve or porcine valve because of structural valve deterioration of the
stented bioprosthesis.64 The choice between the 2 types of porcine bioprosthetic valve. With permission from Hammer-
meister KE, Sethi GK, Henderson WG, et al. Outcomes 15 years
prosthetic heart valves is a choice between which compli-
after valve replacement with a mechanical versus a bioprosthetic
cation is a greater problem for an individual patient and to valve: final report of the VA randomized trial. J Am Coll Car-
be avoided: anticoagulants and its complications with a diol. 2000;36:1152-1158. DVA developmental venous anom-
mechanical valve or the structural valve deterioration and its aly; VHD valvular heart disease; AVR aortic valve
complications with the use of a bioprosthesis. Patients un- replacement.
dergoing aortic valve replacement who are at least 60 to 65
years of age should receive a bioprosthesis. Current data
indicate that the Carpentier-Edwards pericardial valve has a
vival after valve replacement depends largely on patient-
lower rate of structural deterioration than a porcine pros-
related factors.63,65
thetic heart valve.64 In the Veterans Administration trial,
All prosthetic heart valves are smaller in area than the
only 40% to 50% of the deaths after valve replacement
native human valve and thus have the problem of valve
were related to the prosthetic valve, confirming that sur-
prosthesis–patient mismatch.40 After aortic valve replace-
ment, severe mismatch (valve area 0.6 cm2/m2) is asso-
100 ciated with significant morbidity and increased mortality.64
Valve Repair
original prosthesis intact (%)
80
AVR Aortic Valve. Aortic valve repair is performed most often
Patients surviving with
for congenital aortic stenosis with mobile, noncalcified aor-
60
tic valves. Many of these valves are suitable for catheter
balloon commissurotomy. Repair also is performed in se-
MVR lected patients with severe aortic regurgitation.
40
Mitral Valve. After Lillehei performed mitral valve repair
to treat mitral regurgitation in 1957,65 many more surgeons,
20 Mechanical including McGoon and Kay, advocated and practiced the
Bioporosthesis
procedure. It became even more popular in the 1970s, with
the elegant repair methods of Carpentier and Duran,65 and
0
0 2 4 6 8 10 12 14 16 18 20 again after 1983, when Carpentier66 described his sophisti-
Years after randomization cated “French correction.” A major advantage to mitral
valve repair, as opposed to replacement, is that it circum-
Figure 7 Survival with original valve after aortic valve re- vents both the complications of prosthetic valves and the
placement and mitral valve replacement in the Edinburgh Heart need for anticoagulation therapy associated with mechanical
Valve trial. Adapted from Oxenham H, Bloomfield P, Wheatley prosthetics.
DJ, et al. Twenty year comparison of a Bjork-Shiley mechanical
heart valve with porcine bioprostheses. Heart. 2003;89:715-721.
AVR aortic valve replacement; MVR mitral valve
Valve Surgery and Coronary Artery Disease. A combi-
replacement. nation of valve surgery and coronary artery bypass graft
surgery is the routine procedure in these patients.
9. 672 The American Journal of Medicine, Vol 121, No 8, August 2008
14. Lagerlöf H, Werkö L. Studies on the circulation of blood in man VI.
Table 5 Some Desirable Progress in the Future of Valvular The pulmonary capillary venous pressure pulse in man. Scand J Clin
Heart Disease Lab Invest. 1949;1:147-161.
15. Ross J, Jr. Transseptal left heart catheterization: a new method of left
Elimination, or at least marked reduction, of rheumatic heart
arterial puncture. Ann Surg. 1959;149:395-401.
disease in developing countries 16. Seldinger SI. Catheter replacement of the needle in percutaneous
Better knowledge of the development and growth of native arteriography; a new technique. Acta Radiol. 1953;39:368-376.
valves, including the role of genetics and other factors 17. Gorlin R, Gorlin SG. Hydraulic formula for the calculation of the
More accurate and complete knowledge of the causes of valve stenotic mitral valve, other cardiac valves, and central circulatory
disease shunts. Am Heart J. 1951;41:1-29.
Better assessment of severity of valve stenosis 18. Castellanos A, Pereiras R, Garcia AA. L’angio-cardiogra radio-opaca
More accurate measured quantitative assessment of valve chez l’enfant. Arch Estud Clin Habana. 1937;31:523-527.
regurgitation 19. Dodge HT, Sandler H, Ballew DW, et al. The use of biplane angio-
More precise and accurate documentation of the natural history cardiography for the measurement of left ventricular volume in man.
Am Heart J. 1960;60:762-776.
of all asymptomatic patients with severe, moderate, and mild
20. Barrat-Boyes B, Wood EH. Cardiac output and related measurement
valve disease and pressure values in the right heart and associated vessels, response
Better therapeutic options: to the inhalation of high oxygen mixtures in healthy subjects. J Lab
Pharmacologic agents for primary and secondary prevention Clin Med. 1958;51:72-90.
Optimal timing of invasive procedures 21. Ehsani, Rahimtoola SH, Sinno MZ, et al. Left ventricular performance
Better PHV, including tissue-engineered (including stem cell) during convalescent phase of myocardial infection. Arch Int Med.
PHV 1975;135:1539-1575.
Percutaneous therapeutic procedures 22. Sones FM, Jr, Shirey EK, Prondfit WL, et al. Cinecoronary arteriog-
Better therapeutic options for tricuspid valve disease raphy. Circulation. 1959;20:773.
Hybrid procedures (valve replacement CABG/PCI), performed 23. Judkins MP. Selective coronary arteriography: a percutaneous trans-
femoral technique. Radiology. 1967;89:815-824.
in a combined catheterization laboratory operating room
24. Edler I, Hertz CH. Use of ultrasonic reflectoscope for the continuous
Early diagnosis and treatment of emergencies in valvular heart
recording of the movements of heart walls. Kunglia Fysiografska
disease Sallskapets I Lund Frohandlingar. 1954;24:1-19.
PHV prosthetic heart valve; CABG coronary bypass graft surgery; 25. Hatle L, Angelsen BA, Tromsdal A. Non-invasive assessment of aortic
PCI percutaneous catheter intervention. stenosis by Doppler ultrasound. Br Heart J. 1980;43:284-292.
26. Wood P. An appreciation of mitral stenosis. Br Med J. 1954;1:1051-
1063, 1113-1124.
27. John S, Bashi VV, Jairaj PS, et al. Closed mitral valvotomy: early
FUTURE DIRECTIONS results and long term follow-up of 3724 consecutive patients. Circu-
Our hopes for further advancements in valvular heart dis- lation. 1983;68:891-896.
ease are summarized in Table 5. 28. Roy SB, Gopinath N. Mitral stenosis. Circulation. 1968;38(suppl
V):68-76.
29. Hickey MSJ, Blacksone E, Kirklin JW, et al. Outcome probabilities
References after surgical commissurotomy: implication for balloon commissurot-
1. Luderitz B. Book review. N Engl J Med. 2002;347:2175. omy. J Am Coll Cardiol. 1991;17:29-42.
2. LeRoy F. A Century of Nobel Prize Recipients, Chemistry Physics and 30. Rahimtoola SH, Durairaj A, Mehra N, Nuno I. Current evaluation and
Medicine. New York, NY: Marcel Dekker, Inc; 2003;229-360. management of patients with mitral stenosis. Circulation. 2002;106:
3. Comroe JH, Jr. Exploring the Heart. New York: WW Norton & Co; 1183-1188.
1983;3-21. 31. Bonow RO, Carabello B, de Leon AC. Task Force on practice guide-
4. Lewis T (Sir). Special Report Series to the National Health Insurance lines (Committee on management of patients with a report of the
Joint Committee, Medical Research Committee. 1917:8. American College of Cardiology/American Heart Association ACC/
5. Grant RT. After-histories for 10 years of a thousand men suffering AHA guidelines for the management of patients with valvular heart
from heart disease. Heart. 1933;16:275-334. disease. J Am Coll Cardiol. 1998;32;1486-1582.
32. Rahimtoola SH. Indications for surgery in aortic valve disease. In:
6. Feinstein AR. Current problems and future challenges in randomized
Yusuf S, Cairns J, Camm J, Gallen E, Gersh B, eds. Evidence Based
clinical trials. Circulation. 1984;70:767-774.
Cardiology. London: BMJ Publishing Books; 1998:811-832.
7. Fisher RA, Mackenzie WA. Studies in crop variation. II The manorial
33. Scognamiglio R, Rahimtoola SH, Fasoli G, et al. Nifedipine in asymp-
response to different potato varieties. J Agric Sci. 1923;13:315.
tomatic patients with severe aortic regurgitation and normal left ven-
8. Alban B, Epstein JA, Feinstein AR. Rheumatic fever in children and
tricular function. N Engl J Med. 1994;331:689-695.
adolescents: a long-term epidemiologic study of subsequent prophy-
34. Clark DG, McAnulty JH, Rahimtoola SH. Valve replacement in aortic
laxis, streptococcal infection and clinical sequelae. Ann Intern Med. insufficiency with left ventricular dysfunction. Circulation. 1980;61:
1964;60(Suppl 5):1-129. 411-421.
9. Wood P. Disease of the Heart and Circulation. Eyre & Spottiswoode 35. Tornos P, Sambola A, Permanyar-Miralda C, et al. Long-term outcome
2nd Edition. 1956:471-604. of surgically treated aortic regurgitation. J Am Coll Cardiol. 2006;46:
10. Stollerman GH. Rheumatic Fever and Streptococcal Infections. New 1012-1017.
York: Grune & Stratton, Inc. 1975;21-146. 36. Freeman RV, Otto CM. Spectrum of calcific aortic valve disease:
11. Newsholme A. The Milroy lectures on the natural history and affinities pathogenesis, disease progression, and treatment strategies. Circula-
of rheumatic fever: a study in epidemiology. Lancet. 1895;1:589-595, tion. 2005;111:3316-3326.
657-665. 37. Rajamannan N, Bonow RO, Rahimtoola SH. Calcific aortic stenosis:
12. Jones TD. Diagnosis of rheumatic fever. JAMA. 1944;126:481-484. an update. Nat Clin Pract Cardiovasc Med. 2007;4:254-262.
13. Hellems HK, Haynes FW, Dexter L. Pulmonary ‘capillary’ pressure in 38. Ross J, Jr, Braunwald E. Aortic stenosis. Circulation. 1968;36(suppl
man. J Appl Physiol. 1949;2:24-29. IV):61-67.
10. Sharma et al Valve Disease 673
39. Horstkotte D, Loogen F. The natural history of aortic valve stenosis. 54. Rahimtoola SH. The twenty-fifth anniversary of valve replacement: a
Eur Heart J. 1988;9(suppl E):57-64. time for reflection. Circulation. 1985;71:1-3.
40. Rahimtoola SH. The problem of valve prosthesis-patient mismatch. 55. McGoon DC, Pestana C, Moffitt EA. Decreased risk of aortic valve
Circulation. 1978;58:20-24. surgery. Arch Surg. 1965;91:779-786.
41. Rahimtoola SH. Perspective on valvular heart-disease: an update. J Am 56. Gao G, Wu YX, Grunkemeier GL, Starr A. Forty year survival with
Coll Cardiol. 1989;14:1-23. the Starr-Edwards heart valve prosthesis. J Heart Valv Dis. 2004;13:
42. Griffith MJ, Carey C, Coltart DJ, et al. Inaccuracies of using aortic 91-96.
valve gradients alone to grade severity of aortic stenosis. Br Heart J. 57. Murday AJ, Hochstizky A, Mansfield J, et al. A prospective controlled
1989;62:372-378. trial of St. Jude versus Starr Edwards aortic and mitral valve prosthe-
43. Schwarz F, Banmann P, Manthey J, et al. The effect of aortic valve ses. Ann Thorac Surg. 203;76:66-74.
replacement on survival. Circulation. 1982;66:1105-1110. 58. Carpentier A, Lemaigre G, Robert L. Biological factors affecting
44. Smith N, McAnulty JH, Rahimtoola SH. Severe aortic stenosis with long-term results of valvular homografts. J Thorac Cardiovasc Surg.
impaired left ventricular function and clinical heart failure. Results of 1969;58:467-483.
valve replacement. Circulation. 1978;58:255-264. 59. Carpentier A, Dubost C. From xenograft to bioprosthesis. In: Ionescu
45. Connolly HM, Oh JK, Schaff HV, et al. Severe aortic stenosis with low
MI, Ross DN, Wooler GH, eds. Biological Tissue in Heart Valve
transvalvular gradient and severe left ventricular dysfunction: results of
Replacement. London: Butterworth; 1971:515-541.
aortic valve replacement in 52 patients. Circulation. 2000;101:1940-1946.
60. Ross DN. Replacement of aortic and mitral valves with a pulmonary
46. Mackenzie J. Diseases of the Heart. Oxford University Press; 1908;
autograft. Lancet. 1967;2:956-958.
220-234.
61. Rankin JS, Hammill BG, Ferguson TB, Jr, et al. Determinants of
47. Leatham A. Auscultation of the heart. Lancet. 1958;2:703-708, 757-
operative mortality in valvular heart surgery. J Thorac Cardiovasc
765.
48. McKusick VA. Cardiovascular Sound in Health and Disease. Balti- Surg. 2006;131:547-557.
more, MD: Williams & Wilkins Co; 1958;202-212. 62. Oxenham H, Bloomfield P, Wheatley DJ, et al. Twenty year compar-
49. Barlow JB, Pocock WA, Marchand P, et al. The significance of late ison of a Bjork-Shiley mechanical heart valve with porcine biopros-
systolic murmurs. Am Heart J. 1963;66:443-452. theses. Heart. 2003;89:715-721.
50. Connolly HM, Crary JL, McGoon MD, et al. Valvular heart disease 63. Hammermeister KE, Sethi GK, Henderson WG, et al. Outcomes 15
associated with fenfluramine-phentermine. N Engl J Med. 1997;337: years after valve replacement with a mechanical versus a bioprosthetic
581-588. valve: final report of the VA randomized trial. J Am Coll Cardiol.
51. Rosenhek R, Rader F, Klaar H, et al. Outcome of watchful waiting in 2000;36:1152-1158.
asymptomatic severe mitral regurgitation. Circulation. 2006;113: 64. Rahimtoola SH. Choice of prosthetic heart valve for adult patients.
2238-2244. J Am Coll Cardiol. 2003;41:893-894.
52. Gibbon JH, Jr. Application of a mechanical heart and lung apparatus 65. Rahimtoola SH. Lessons learned about the determinants of the results
to cardiac surgery. Minn Med. 1954;37;171-180. of valve surgery. Circulation. 1988;78:1503-1507.
53. Starr A, Edwards ML. Mitral replacement: clinical experience with a 66. Carpentier A. Cardiac valve surgery—“the French correction.” J Tho-
ball-valve prosthesis. Ann Surg. 1961;154:726-740. rac Cardiovasc Surg. 1983;86:323-337.