
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Trigeminal nerve
Ähnlich wie Trigeminal nerve (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Trigeminal nerve
- 2. Nervous system is the most complex system in the body, it is responsible for • Behavior • Thought • Action • Emotion reflects its activity
- 3. Classification of Nerve System 1. Anatomical • Central nervous system • Peripheral nervous system 2. Functional • Afferent • Efferent • Somatic • Autonomous
- 4. CELLULAR ORGANIZATION OF N.S Nervous system consists of two principal categories of cells. • Nerve cells or neurons • Supporting cells or neuroglia
- 5. CRANIAL NERVES • There are 12 pairs of cranial nerves, out of these 2 pairs arise from forebrain and 10 pairs from brain stem. • All the 12 pairs of cranial nerves are attached on the ventral aspect of brain except the 4th pair which is attached on dorsal aspect.
- 6. Morphological classification Those supplying muscles derived from cranial myotomes (Motor) • Oculomotor • Trochlear • Abducent • Hypoglossal • Accessory Muscles derived from brachial arches (Mixed) • Trigeminal • Glassopharyngeal • Vagus • Facial Those associated with special sense organs (Sensory) • Olfactory • Optic • Vestibulocochleor
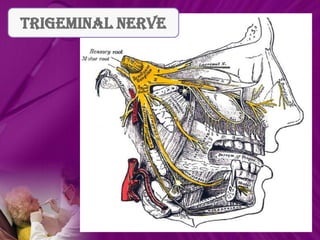
- 8. • The fifth vertebrate peripheral nerve that emerges from within the skull. • It is sensory from the head, but motor to the jaw muscles. • The largest cranial nerve. • It was described by Fallopius and again by Meckel in 1748. • The term trigeminal was given by Winslow on account of its three divisions.
- 9. • The part of parasympathetic craniosacral outflow • It is mixed nerve ( sensory and motor ) • Contains 1,70,000 sensory fibres 7,700 motor fibres • The 3 divisions have approx Ophthalmic 26,000 Maxillary 50,000 Mandibular 78,000
- 10. EMBROYOLOGY
- 13. NUCLEI
- 15. There are four trigeminal nuclei: one motor and three sensory The motor nucleus of CNV is in the superior part of the pons, deep to the floor of the 4th ventricle. The mesencephalic nucleus of CNV is lateral to the cerebral aqueduct. The principal sensory nucleus is in the dorsolateral area of the pontine tegmentum at the level of entry of the sensory fibres. The spinal nucleus of CNV is in the inferior part of the pons and throughout the medulla
- 16. SENSORY NUCLEI • The sensory function of the trigeminal nerve is to provide the tactile, proprioceptive, and nociceptive afference of the face and mouth. Mesencephalic nucleus First order sensory nucleus Cell body of pseudounipolar neurons exception to a general rule that first order neuron of CN lie outside CNS. Relay proprioception from muscle of mastication, EOM, facial muscles. Forms monosynaptic reflex arc . Situated in midbrain just lat to aqueduct.
- 17. Principal sensory nucleus- lies in pons lat to motor nucleus relays discriminitive touch Spinal nucleus- extends from caudal end of principal sen. Nuc. In pons to 2nd or 3rd spinal seg where its conti with sub.Gelatinosa. Divided in : PARSR ROSTRALIS PARS INTERPOLARIS PARS CAUDALIS
- 19. MOTOR NUCLEUS • The motor function activates the muscles of the mastication, the tensor tympani, tensor veli palatini, mylohyoid, and anterior belly of the digastric. • Innervates muscles of mastication tensor tympani and tensor palatini • Derived from first branchial arch. • Located in pons med. To princi sen. Nuc.
- 20. FUNCTIONAL COMPONENTS SENSORY ROOT GENERAL SOMATIC AFFERENTS FACE, SCALP, TEETH, GINGIVA, ORAL MUCOSA, NASAL CAVITIES, PNS ,CONJUNCTIVA AND CORNEA. Pain,temp,light touch, pressure proprioception trigeminal gang. Bypasses trigem gang. sensory root. descending fibres ascending fibres
- 21. descending fibres ascending fibres Spinal nuc. Principal sen nuc. Mesencephalic trigeminothalamic tract Thalamus post central gyrus cerebral cortex
- 22. MOTOR NUCLEUS MOTOR ROOT MANDIBULAR NERVE muscles of mastication tensor tympani massetor tensor palatini lat med pterygoids temporalis
- 23. SEMILUNAR OR GASSERIAN GANGLION • Cresentric in shape with convexity anterolat. • Contains cell bodies of pseudounipolar neurons. • LOCATION: lies in a bony fossa at apex of the petrous temporal bone on floor of middle cranial fossa , just lat to post. Part of lat wall of the cavernous sinus.
- 25. • COVERINGS: covered by dural pouch = MECKLES CAVE OR CAVUM TRIGEMINALE. Roof- 2 layers of dura floor- 1 dural and 1endosteal dural layer. cave lined by pia and arachnoid thus the ganglion is bathed in CSF. • ARTERIAL SUPPLY: ganglionic branches of ICA, middle meningeal artery and accessory meningeal artery.
- 29. OPTHALMIC NERVE
- 32. SO STN SON LPS SR LG MR LR LN FN NCN TN
- 34. PEN AEN ITN MR LCN SCN LG LN LR CG AN INT DIV ON NCN Sup Div of ON
- 38. MAXILLARY NERVE
- 50. MANDIBULAR NERVE
- 64. Applied Anatomy
- 65. TRIGEMINAL NEURALGIA DEFINITION: It is defined as sudden usually unilateral, severe, brief, stabbing, lancinating, recurring pain in the distribution of one or more branches of the Vth cranial nerve.
- 66. HISTORICAL REVIEW OF TRIGEMINAL NEURALGIA: JOHN LOCKE in 1677 gave the first full description with its treatment. NICHOLAS ANDRE in 1756 coined the term ‘Tic Doloureux’. JOHN FOTHERGILL in 1773 published detailed description of trigeminal neuralgia.
- 67. TIC DOULOUREUX: Tic douloureux painful jerking It is a truly agonizing condition, in which the patient may clunch the hand over the face & experience severe, lancinating pain associated with spasmodic contractions of the facial muscles during attacks – a feature that led to use of this term
- 68. AETIOLOGY: Usually idiopathic Demylination of the nerve Multiple sclerosis Petrous ridge compression Post – traumatic neuralgia Intracranial tumours Intracranial vascular abnormalities Viral etiology
- 69. PATHOGENESIS:
- 70. GENERAL CHARACTERISTICS: Incidence: 8 : 1,00,000 Age: 5th – 6th decade of life Sex: Female > male ; 1.6 > 1.0 Affliction for side: Right > left Division of trigeminal nerve involvement: V3 > V2 > V1
- 71. CLINICAL CHARACTERISTICS: Manifests as a sudden, unilateral, intermittent paroxysmal, sharp, shooting, lancinating, shock like pain, elicited by slight touching superficial ‘trigger points’ which radiates from that point, across the distribution of one or more branches of the trigeminal nerve. Pain is usually confined to one part of one division of trigeminal nerve. Pain rarely crosses the midline. Attacks do not occur during sleep.
- 72. Pain is of short duration, but may recur with variable frequency. In extreme cases, the patient will have a motionless face – the ‘frozen or mask like face’. Common trigger zones include: Cutaneous Intraoral Corner of the lips Teeth Cheek Gingivae Ala of the nose Tongue Lateral brow
- 73. DIAGNOSIS: From well taken history CT – scan MRI Diagnostic nerve block
- 74. TREATMENT MODALITIES: MEDICAL SURGICAL
- 75. MEDICAL MANAGEMENT: CARBAMAZEPINE: Trade name: Tegretol Carbitrol PHENYTOIN: Trade name: Dilantin GABAPENTIN: Trade name: Neurontin BACLOFEN: Trade name: Lioresal TRICYCLINE ANTIDEPRESSANTS
- 76. SURGICAL MANAGEMENT: PERIPHERAL INJECTION: It has been known that injection of destructive substance into peripheral branches of the trigeminal nerve, produces anaesthesia in the trigger zones or in areas of distribution of spontaneous pain. (A) LONG ACTING ANAESTHETIC AGENTS: Without adrenaline such as bupivacaine with or without corticosteroids may be injected at the most proximal possible nerve site.
- 77. (B) ALCOHOL INJECTION: 0.5 – 2 ml of 95 % absolute alcohol can be used to block the peripheral branches of the trigeminal nerve. Aim is to destroy the nerve fibres. It produces total numbness in the region of distribution of the nerve that was anaesthetized. Complication: Necrosis of the adjacent tissue Fibrosis Alcohol induced neuritis
- 78. PERIPHERAL NEURECTOMY (NERVE AVULSION): CRYOTHERAPHY:
- 79. GASSERIAN GANGLION PROCEDURES: PERCUTANEOUS RHIZOTOMY:
- 81. OPEN PROCEDURES ( INTRACRANIAL PROCEDURES): (A) Microvascular decompression of the trigeminal nerve sensory root: (B) Trigeminal root section:
- 82. Trigeminal neuropathy Sensory loss of face or weakness of the jaw muscles Causes- SLE, sjogren syndrome herpes zoster leprosy meningioma schwanomma
- 83. Wallenberg Syndrome (Lateral Medullary Syndrome) • In the medulla, the ascending spinothalamic tract (which carries pain/temperature information from the opposite side of the body) is adjacent to the descending spinal tract of the fifth nerve (which carries pain/temperature information from the same side of the face). • A stroke that cuts off the blood supply to this area (e.g., a clot in the posterior inferior cerebellar artery) destroys both tracts simultaneously. • The result is loss of pain/temperature sensation (but not touch/position sensation) in a unique “checkerboard” pattern (ipsilateral face, contralateral body) that is entirely diagnostic.
- 84. Herpes zoster ophthalmicus • Recurrent neurocutaneous inf. In opth. Div. of trigeminal dermatome, most freq. affecting nasociliary branch • HHV3 / vericella zoster • Gasserian ganglion ophthalmic nerve Supraorbital N. Infraorbital N. Supratrochlear N. Infratrochlear N. Nasal N.
- 85. • Pain precedes skin lesion • C/P is hemifacial unioccular • Cutaneous lesions evolve over few days Cutaneous lesion MP rash Vesicle Pustules Crust Permanent scar
- 86. Neurotrophic keratitis • Occurs dt partial or complete corneal anaesthesia dt loss of sensory innervation by the trigeminal N. • There is impaired response to corneal microtrauma as a result of impaired regeneration and healing of corneal epi. • Causes: infections viz HSV, VZV, leprosy traumatic V N injury ablation of gasserian ganglion chemical burns topical anaesthatic abuse, betablockrs,NSAIDS refractive Sx contact lens wear systemic: DM,MS, stroke, brainstem haemorrhage, aneurysm congenital
- 87. Cavernous sinus syndrome • Multiple cranial neuropathies Exophthalmos, ocular motor defects Horner’s syndrome • Sensory loss in V1 and / or V2. • Pupils may be spared or involved. • Causes: bacterial thrombophlebitis actinomycosis rhinocerebellar mucormycosis aspergillosis tolosa hunt syndrome neoplasms vascular lesions
- 88. Gradenigos syndrome • Petrous bone osteitis due to otitis media • Characterized by I/L trigeminal N palsy (Va, Vb) retro orbital pain I/L sixth N palsy.
- 89. Clinical Implication in Periodontics Posterior Superior • Mandibular anesthesia Alveolar block • Trismus LA • Paresthesia • Burning sensation • Position of lingual nerve Flap Retraction • Mental nerve Nicking of artery & • Hematoma vein • Apical end should be 2mm away from the nerve Implant • Drilling of implant • Incision should be 1-2 mm away from palatine Palatal Flap nerve • Blade should be kept vertical to palate.
- 90. REFRENCES • Human Anatomy ,vol.3 Head , Neck & Brain B.D Churasia • Cunningham’s Manual of Practical Anatomy vol.3 • Gray’s Anatomy Standring 39th Edition • Medical Embroyology Langham 8th Edition • IB Singh Textbook of Anatomy 2nd Edition • Textbook of oral surgery Neelima Malik • Textbook of Local anesthesia Monheim • Local Anesthesia Malamed • Clinical Periodontology & implant Dentistry Lindhe 4th Edition
- 91. THANK YOU