1. chapter 64
Drugs Used in Oncologic Disorders
Objectives
AFTER STUDYING THIS CHAPTER, THE STUDENT WILL BE ABLE TO:
1. Contrast normal and malignant cells. 5. Describe pharmacologic and nonpharmacologic
2. Describe major types of antineoplastic drugs interventions to prevent or minimize adverse
in terms of mechanism of action, indications drug effects.
for use, administration, and nursing process 6. Promote reduction of risk factors for develop-
implications. ment of cancer and early recognition of cancer
3. Discuss the rationales for using chemotherapeu- signs and symptoms.
tic drugs in combination with each other, with 7. Manage or assist clients/caregivers in manag-
surgical treatment, and with radiation therapy. ing symptoms associated with chemotherapy
4. Discuss common and potentially serious regimens.
adverse drug effects.
Critical Thinking Scenario
Georgia Sommers, a 39 year-old mother of 4, is diagnosed with breast cancer that was detected by routine
mammography. She is recovering from a modified radical mastectomy when she comes to the clinic to dis-
cuss additional treatment with chemotherapy with the oncologist. He explains that she will receive combina-
tion therapy with three drugs on a cycle of every 4 weeks.
Reflect on:
Possible reactions of Ms. Sommers to a diagnosis of cancer. What is the role of the nurse during the
period of initial diagnosis?
How will you assess Ms. Sommers concerns regarding chemotherapy?
What are the benefits of combination (using more than one drug) therapy?
What impact do you think chemotherapy might have on Ms. Sommers’ ability to function normally and
meet normal demands of life?
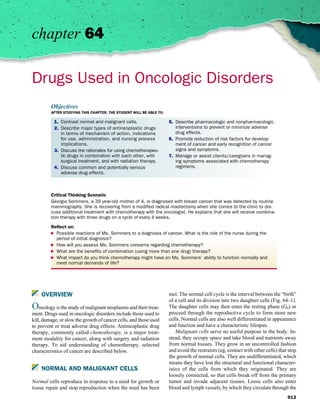
OVERVIEW met. The normal cell cycle is the interval between the “birth”
of a cell and its division into two daughter cells (Fig. 64–1).
Oncology is the study of malignant neoplasms and their treat- The daughter cells may then enter the resting phase (G0) or
ment. Drugs used in oncologic disorders include those used to proceed through the reproductive cycle to form more new
kill, damage, or slow the growth of cancer cells, and those used cells. Normal cells are also well differentiated in appearance
to prevent or treat adverse drug effects. Antineoplastic drug and function and have a characteristic lifespan.
therapy, commonly called chemotherapy, is a major treat- Malignant cells serve no useful purpose in the body. In-
ment modality for cancer, along with surgery and radiation stead, they occupy space and take blood and nutrients away
therapy. To aid understanding of chemotherapy, selected from normal tissues. They grow in an uncontrolled fashion
characteristics of cancer are described below. and avoid the restraints (eg, contact with other cells) that stop
the growth of normal cells. They are undifferentiated, which
means they have lost the structural and functional character-
NORMAL AND MALIGNANT CELLS istics of the cells from which they originated. They are
loosely connected, so that cells break off from the primary
Normal cells reproduce in response to a need for growth or tumor and invade adjacent tissues. Loose cells also enter
tissue repair and stop reproduction when the need has been blood and lymph vessels, by which they circulate through the
913
2. 914 SECTION 11 DRUGS USED IN SPECIAL CONDITIONS
mutations of normal growth-regulating genes called proto-
G0 oncogenes, which are present in all body cells. Normally,
G1
proto-oncogenes are active for a brief period in the cell re-
productive cycle. When exposed to carcinogens and genetically
altered to oncogenes, however, they may operate continuously
and cause abnormal, disordered, and unregulated cell growth.
Unregulated cell growth and proliferation increases the prob-
ability of neoplastic transformation of the cell. Tumors of the
breast, colon, lung, and bone have been linked to activation
of oncogenes.
M S Tumor suppressor genes (anti-oncogenes) normally func-
tion to regulate and inhibit inappropriate cellular growth and
proliferation. Abnormal tumor suppressor genes (ie, absent,
damaged, mutated, or inactivated) may be inherited or re-
sult from exposure to carcinogens. When these genes are in-
activated, a block to proliferation is removed and the cells
begin unregulated growth. One tumor suppressor gene, p53,
G2 is present in virtually all normal tissues. When cellular de-
oxyribonucleic acid (DNA) is damaged, the p53 gene allows
Figure 64–1 Normal cell cycle. The normal cell cycle (the interval be-
time for DNA repair and restricts proliferation of cells with
tween the birth of a cell and its division into two daughter cells) in-
volves several phases. During the resting phase (G0), cells perform all abnormal DNA. Mutations of the p53 gene, a common ge-
usual functions except replication; that is, they are not dividing but are netic change in cancer, are associated with more than 90% of
capable of doing so when stimulated. Different types of cells spend small-cell lung cancers and more than 50% of breast and
different lengths of time in this phase, after which they either reenter colon cancers. Mutant p53 proteins can also form complexes
the cell cycle and differentiate or die. During the first active phase (G1),
ribonucleic acid (RNA) and enzymes required for production of de-
with normal p53 proteins and inactivate the function of the
oxyribonucleic acid (DNA) are developed. During the next phase (S), normal suppressor gene.
DNA is synthesized for chromosomes. During G2, RNA is synthesized, Thus, activation of oncogenes and inactivation of anti-
and the mitotic spindle is formed. Mitosis occurs in the final phase oncogenes probably both play roles in cancer development.
(M). The resulting two daughter cells may then enter the resting phase
Multiple genetic abnormalities are usually characteristic of
(G0) or proceed through the reproductive cycle.
cancer cells and may occur concurrently or sequentially.
Overall, evidence indicates that neoplastic transformation
is a progressive process involving several generations of
body and produce additional neoplasms at sites distant from cells, with each new generation becoming more like malig-
the primary tumor (metastasis). nant cells. Thus, malignancy probably results from a combi-
A malignant cell develops from a transformed normal cell. nation of factors experienced over a person’s lifetime. One
The transformation may begin with a random mutation (ab- factor may be a random cell mutation. However, mutations
normal structural changes in the genetic material of a cell). A and malignancies are increased in people exposed to certain
mutated cell may be destroyed by body defenses (eg, an im- chemical, physical, or biologic factors, especially in large
mune response), or it may replicate. During succeeding cell amounts or for long periods of time. Some carcinogens and
divisions, additional changes and mutations may produce risk factors are listed in Box 64–1. Once a cancer develops,
cells with progressively fewer normal and more malignant factors influencing the growth rate include blood and nutri-
characteristics. It usually takes years for malignant cells to ent supply, immune response, and hormonal stimulation
produce a clinically detectable neoplasm. (eg, in tumors of the breast, uterus, ovary, and prostate).
CANCER Classification of Malignant Neoplasms
The term cancer is used to describe many disease processes Malignant neoplasms are classified according to the type of
with the common characteristics of uncontrolled cell growth, tissue involved, the rate of growth, and other characteristics.
invasiveness, and metastasis, as well as numerous etiologies, With the exception of the acute leukemias, they are considered
clinical manifestations, and treatments. One theory of carcino- chronic diseases.
genesis involves abnormal genes and cells, in which cancer Hematologic malignancies involve the bone marrow and
may be caused by mutation of genes (abnormal structural lymphoid tissues; they include leukemias, lymphomas, and
changes in cellular genetic material), abnormal activation of multiple myeloma. Leukemias are cancers of the bone marrow
genes that regulate cell growth and mitosis, or lack of tumor characterized by overproduction of abnormal white blood cells.
suppressor genes. The abnormal genes, called oncogenes, are The four main types are acute lymphocytic; acute myelo-
3. CHAPTER 64 DRUGS USED IN ONCOLOGIC DISORDERS 915
BOX 64-1
CARCINOGENS AND RISK FACTORS
Despite extensive study, the cause of cancer is not clear. Because women who took the drugs for menopausal symptoms. With breast
cancer is actually many diseases, many etiologic factors are proba- cancer, endogenous estrogens are clearly causative, but the role of
bly involved. The factors that initiate the transformation of a single exogenous estrogens is less clear. Oral contraceptives, most of
normal cell into a malignant cell and allow tumor growth are com- which contain an estrogen and a progestin, have been related to en-
plex and overlapping, including the environmental and host factors dometrial cancer and possibly to breast cancer. A progestin taken
described below. to prevent estrogen-induced endometrial cancer may increase risks
of breast cancer. The antiestrogen tamoxifen, which is widely used
Environmental Carcinogens
to prevent or treat breast cancer, is associated with endometrial can-
Biologic carcinogens include several infections, mainly viral.
cer. Androgens and anabolic steroids, especially with high doses
Viruses linked to cancer include Epstein-Barr (Burkitt lymphoma,
and prolonged use, have been associated with hepatic neoplasms.
Hodgkin’s disease); hepatitis B and C (liver cancer); herpes sim-
plex II (cancer of cervix and vulva); human papilloma (cancer of the Host Factors
cervix, penis, oral cavity, esophagus, larynx); human immunodefi- Age. Except for a few early childhood cancers, the risks of can-
ciency (Kaposi’s sarcoma); and human T-cell lymphotropic (T-cell cer increase with age.
leukemia or lymphoma). In addition, Helicobacter pylori, the bac- Alcohol use may make carcinogens more soluble or enhance
terium that causes most gastric and duodenal ulcers, is also associ- their tissue penetration. Cancers associated with alcohol use
ated with gastric cancer and gastric lymphoma. include those of the breast, head and neck, and liver.
Radiation (eg, from sunlight and tanning beds) can damage Diet. A high-fat diet is associated with breast, colon, and prostate
DNA and cause mutations by changing cell structure or causing cancer; a low-fiber diet may increase risks of colon cancer.
damage that interferes with transfer of genetic information during Sex. Men are more likely to have leukemia and cancer of the
cell reproduction. urinary bladder, stomach, and pancreas; women are at risk
Chemicals include numerous substances that can damage cel- of cancer of the breast, cervix, and endometrium. Lung and
lular structures and interfere with cell replication and regulation. colon cancer occur equally in both sexes.
Industrial carcinogens include benzene (bladder cancer), Geography and ethnicity are more environmental than heredi-
hydrocarbons (lung and skin cancer), polyvinyl chloride (liver tary or racial. Immigrants who adopt dietary and lifestyle
cancer), and other substances used in the production of various habits of natives have similar risks and people who live in
products. Workers who manufacture the products and people who cities have greater risks because of greater exposure to air
live in the plant vicinity are most likely to be affected. Tobacco pollutants and other carcinogens. In the United States,
products contain numerous carcinogens and are associated with African Americans have higher rates of multiple myeloma
cancers of the lungs, mouth, pharynx, larynx, esophagus, and blad- and cancers of the lung, prostate, esophagus, and pancreas
der. Chemicals in cigarette smoke cause most lung cancer, in than white people.
smokers and other people exposed to cigarette smoke. Children Heredity. In some families, there is a strong tendency toward
development of cancer. For example, close relatives of pre-
whose parents smoke have an increased risk of brain cancer, lym-
menopausal women with breast cancer are at high risk for
phomas, and acute lymphocytic leukemia. Smokeless tobacco
breast cancer.
products are also carcinogens.
Immunosuppression, whether caused by disease or drug ther-
Therapeutic drugs are associated with both hematologic and
apy, is associated with an increased risk of cancer. For ex-
solid neoplasms. The alkylating antineoplastic drugs are associated
ample, clients with acquired immunodeficiency syndrome
with leukemia, lymphoma, and other cancers. The drugs damage
are at risk for Kaposi’s sarcoma, and clients who undergo
DNA and interfere with growth or replication of tumor cells. At the
organ transplantation and receive immunosuppressant drugs
same time, they may damage the DNA of normal cells and trans- are at risk for lymphomas and skin cancers.
form some of them into malignant cells. Clients who are given Obesity has been associated with increased risks of developing
these drugs and survive their illness have an increased risk of de- cancer of the breast, colon, endometrium, esophagus, liver,
veloping leukemia for 15 to 20 years. Antineoplastic drugs that pancreas, and prostate gland.
cause bone marrow suppression or immunosuppression may also Previous cancer is associated with a higher risk of other cancers
lead to secondary cancer. Immunosuppressants (eg, azathioprine in those who are treated and survive (eg, children with
and corticosteroids in renal transplant recipients) are associated leukemia may develop other cancers; women with cancer in
with an increased risk of non-Hodgkin’s lymphoma, which may one breast have a higher risk of cancer in the other breast; fe-
appear within months of transplantation, and for later skin cancer male survivors of Hodgkin’s disease have a greater risk of de-
(eg, squamous cell carcinoma and malignant melanoma) and veloping breast cancer than the general population; patients
Kaposi’s sarcoma. Other clients on immunosuppressant drugs are who received radiation may develop bone and soft tissue sar-
at risk for lymphomas, squamous cell carcinoma of skin, and soft comas; those who received radiation to the neck area may de-
tissue sarcomas, but at lower rates than transplant recipients. For velop thyroid cancer; and patients who received radiation to
example, leukemia and solid tumors have been reported in clients the head may develop brain tumors). Secondary cancers are
who took azathioprine for rheumatoid arthritis. usually attributed to treatments that damage DNA and even-
Sex hormones are growth factors for certain cells. Estrogens are tually transform normal cells into malignant cells.
associated with cancer of the vagina in daughters of women who Tobacco use is a major lifestyle risk factor for cancers of the
took the drugs during pregnancy and with endometrial cancer in lung, esophagus, and head and neck.
4. 916 SECTION 11 DRUGS USED IN SPECIAL CONDITIONS
genous; chronic lymphocytic; and chronic myelogenous. ANTINEOPLASTIC DRUGS
Lymphomas are tumors of lymphoid tissue characterized by
abnormal proliferation of the white blood cells normally General Characteristics
found in lymphoid tissue. They usually develop within lymph
nodes and may occur anywhere, because virtually all body 1. Most drugs kill malignant cells by interfering with
tissues contain lymphoid structures. The two main types are cell replication, with the supply and use of nutrients
Hodgkin’s disease and non-Hodgkin’s lymphoma. Multiple (eg, amino acids, purines, pyrimidines), or with the
myeloma is a tumor of the bone marrow in which abnormal genetic materials in the cell nucleus (DNA or RNA).
plasma cells proliferate. Because normal plasma cells pro- 2. The drugs act during the cell’s reproductive cycle
duce antibodies and abnormal plasma cells cannot fulfill this (Fig. 64–2). Some, called cell cycle specific, act mainly
function, the body’s immune system is impaired. As the ma- during specific phases such as DNA synthesis or forma-
lignant cells expand, they crowd out normal cells, interfere tion of the mitotic spindle. Others act during any phase
with other bone marrow functions, infiltrate and destroy of the cell cycle and are called cell cycle nonspecific.
bone, and eventually metastasize to other tissues, such as the 3. Cytotoxic drugs are most active against rapidly divid-
spleen, liver, and lymph nodes. ing cells, both normal and malignant. Commonly dam-
Solid neoplasms are composed of a mass of malignant aged normal cells are those of the bone marrow, the
cells (parenchyma) and a supporting structure of connective lining of the gastrointestinal tract, and the hair follicles.
tissue, blood vessels, and lymphatics (stroma). The two 4. Each drug dose kills a specific percentage of cells. To
major classifications are carcinomas and sarcomas. Carci- achieve a cure, all malignant cells must be killed or
nomas are derived from epithelial tissues (skin, mucous reduced to a small number that can be killed by the
membrane, linings and coverings of viscera) and are the person’s immune system.
most common type of malignant tumors. They are further 5. Antineoplastic drugs may induce drug-resistant malig-
classified by cell type, such as adenocarcinoma or basal cell nant cells. Mechanisms may include inhibiting drug up-
carcinoma. Sarcomas are derived from connective tissue take or activation, increasing the rate of drug inactivation,
(muscle, bone, cartilage, fibrous tissue, fat, blood vessels). pumping the drug out of the cell before it can act, in-
They are subclassified by cell type (eg, osteogenic sarcoma, creasing cellular repair of DNA damaged by the drugs,
angiosarcoma). or altering metabolic pathways and target enzymes of
the drugs. Mutant cells also may emerge.
6. Most cytotoxic antineoplastic drugs are potential ter-
Grading and Staging of atogens.
7. Most antineoplastic drugs are given orally or intra-
Malignant Neoplasms
venously (IV); some are given topically, intrathecally,
or by instillation into a body cavity.
When a malignant neoplasm is identified, it is further “graded”
8. A few drugs are available in liposomal preparations.
according to the degree of malignancy and “staged” accord-
These preparations increase drug concentration in
ing to tissue involvement. Grades 1 and 2 are similar to the
malignant tissues and decrease concentration in nor-
normal tissue of origin and show cellular differentiation;
mal tissues, thereby increasing effectiveness while
grades 3 and 4 are unlike the normal tissue of origin, less dif-
decreasing toxicity. For example, liposomal doxoru-
ferentiated, and more malignant. Staging indicates whether the
bicin and daunorubicin reduce the drugs’ cardiotoxic
neoplasm is localized or metastasized and which organs are in-
effects.
volved. These characteristics assist in treatment (eg, localized
tumors are usually amenable to surgical or radiation therapy;
metastatic disease requires systemic therapy).
Cell Cycle Phases of Cell Cycle
Nonspecific Cell Cycle Specific
Effects of Cancer on the Host
Alkylating agents G0
Effects vary according to the location and extent of the dis- Antibiotics G1 Steroids
ease process. There are few effects initially. As the neoplasm
grows, effects occur when the tumor becomes large enough Nitrosoureas S Antimetabolites
to cause pressure, distortion, or deficient blood supply in sur-
rounding tissues; interfere with organ function; obstruct ducts G2 Podophyllotoxins
and organs; and impair nutrition of normal tissues. More
M Taxanes or taxoids
specific effects include anemia, malnutrition, pain, infection,
hemorrhagic tendencies, thromboembolism, hypercalcemia, Vinca alkaloids
cachexia, and various symptoms related to impaired function
of affected organs and tissues. Figure 64–2 Cell cycle effects of cytotoxic antineoplastic drugs.
5. CHAPTER 64 DRUGS USED IN ONCOLOGIC DISORDERS 917
Indications for Use approved in 2002 for treatment of colorectal cancer in patients
whose disease has recurred or worsened following standard
Cytotoxic antineoplastic drugs are used in the treatment of therapy. It is used with 5-fluorouracil and leucovorin and given
malignant neoplasms to cure the disease, relieve symptoms, every 2 weeks by injection. Adverse effects include peripheral
or induce or maintain remissions (symptom-free periods that neuropathy, vomiting, diarrhea, and anemia.
last for varying lengths of time). Chemotherapy is the treatment
of choice for Hodgkin’s disease, leukemia, Wilms’ tumor, and
Ewing’s sarcoma, but it is less effective in cancers of the Antimetabolites
lung, colon, and prostate gland. Antimetabolites are substances that are structurally similar to
In hematologic neoplasms, drug therapy is the treatment normal metabolites. They are allowed to enter cancer cells
of choice because the disease is systemic rather than local- because they are similar to nutrients needed by the cells for
ized. In solid tumors, drug therapy is often used before or reproduction. Once inside the cell, the drugs may compete
after surgery or radiation therapy. with, replace, or antagonize the normal metabolite. These ac-
Antineoplastic drugs are sometimes used in the treatment
tions deprive the cell of substances needed for formation of
of nonmalignant conditions. For example, small doses of
DNA or cause formation of abnormal DNA. The drugs are
methotrexate (MTX) are used for rheumatoid arthritis and
cell cycle specific because they exert their cytotoxic effects
psoriasis.
only during the S phase of the cell’s reproductive cycle, when
DNA is being synthesized.
This group includes a folic acid antagonist (eg, methotrex-
Classifications ate), purine antagonists (eg, mercaptopurine), and pyrimidine
antagonists (eg, fluorouracil). These drugs have been used to
Cytotoxic antineoplastic drugs are usually classified in terms treat many types of cancers, but they are most effective against
of their mechanisms of action (alkylating agents and anti- rapidly growing tumors, and individual drugs vary in their
metabolites) or their sources (plant alkaloids, antibiotics). effectiveness with different kinds of cancer. Toxic effects
Other drugs used in chemotherapy are immunostimulants (see include bone marrow depression, mucositis and ulceration of
Chap. 44), hormones, hormone inhibitors, and cytoprotectants. the GI tract, and hair loss (alopecia).
Alkylating Agents Antitumor Antibiotics
Alkylating agents include nitrogen mustard derivatives, ni- These drugs (eg, doxorubicin) are active in all phases of the
trosoureas, and platinum compounds. Nitrogen mustard de- cell cycle and their cytotoxic effects are similar to those of
rivatives (eg, cyclophosphamide) interfere with cell division the alkylating agents. They bind to DNA so that DNA and
and the structure of DNA during all phases of the malignant RNA transcription is blocked. Major toxicities are bone mar-
cell cycle. As a result, they have a broad spectrum of activ- row depression and GI upset. Doxorubicin and related drugs
ity. They are most effective in hematologic malignancies but also cause cardiotoxicity and tissue necrosis if extravasation
also are used to treat breast, lung, and ovarian tumors. All of occurs. Bleomycin may cause significant pulmonary toxicity.
these drugs cause significant myelosuppression (bone mar- All of these drugs except bleomycin must be given IV.
row depression).
Nitrosoureas also interfere with DNA replication and RNA
synthesis and may inhibit essential enzymatic reactions of can- Plant Alkaloids
cer cells. They are cell cycle nonspecific and have been used in
clients with gastrointestinal (GI), lung, and brain tumors. They Plant alkaloids include derivatives of camptothecin (eg, topote-
are highly lipid soluble and therefore enter the brain and cere- can), podophyllotoxin (eg, etoposide), taxanes (eg, pacli-
brospinal fluid more readily than other antineoplastic drugs. taxel), and plants of the Vinca genus (eg, vincristine). These
They cause delayed bone marrow depression, with maximum drugs vary in their characteristics and clinical uses.
leukopenia and thrombocytopenia occurring 5 to 6 weeks after
drug administration. As a result, the drugs are given less often
than other drugs, and complete blood counts (CBCs) are
needed weekly for at least 6 weeks after a dose. Nursing Notes: Apply Your Knowledge
Platinum compounds are cell cycle–nonspecific agents that
inhibit DNA, RNA, and protein synthesis. Cisplatin is widely
used to treat both hematologic and solid cancers. Adverse Your patient, Sally Moore is receiving an antineoplastic drug that
effects include severe nausea and vomiting, nephrotoxicity, is known to cause bone marrow depression, with a nadir (lowest
and ototoxicity. Carboplatin is most often used to treat en- point) 12 days after administration. Discuss the effects of bone
marrow depression and appropriate nursing assessments. What
dometrial and ovarian carcinomas and it produces bone marrow
teaching would be appropriate for this patient?
depression as a major adverse effect. Oxaliplatin (Eloxatin) was
6. 918 SECTION 11 DRUGS USED IN SPECIAL CONDITIONS
Camptothecins (also called DNA topoisomerase inhibitors) It may cause severe bone marrow depression. Ibritumomab is
inhibit an enzyme required for DNA replication and repair. a conjugated antibody used to treat non-Hodgkin’s lymphoma.
They have activity in several types of cancers, including col- It is used with rituximab and may cause severe bone marrow
orectal, lung, and ovarian cancers. Dose-limiting toxicity is depression and fatal infusion-related reactions. Rituximab is
myelosuppression. used to treat non-Hodgkin’s lymphoma. Common adverse
Podophyllotoxins act mainly in the G2 phase of the cell effects include infusion reactions (hypoxia, acute respiratory
cycle and prevent mitosis. Etoposide is used mainly to treat tes- distress syndrome, myocardial infarction, ventricular dys-
ticular and small cell lung cancer; teniposide is used mainly for rhythmias, cardiogenic shock) and lymphopenia.
childhood acute lymphocytic leukemia. Dose-limiting toxicity
is myelosuppression.
Miscellaneous Cytotoxic Agents
Taxanes inhibit cell division (antimitotic effects). They
are used mainly for advanced breast and ovarian cancers. Miscellaneous agents vary in their sources, mechanisms of
Dose-limiting toxicity is neutropenia. action, indications for use, and toxic effects. L-Asparaginase
Vinca alkaloids are cell cycle–specific agents that stop (Elspar) is an enzyme that inhibits cellular protein synthesis
mitosis. These drugs have similar structures but different anti- and reproduction by depriving cells of required amino acids.
neoplastic activities and adverse effects. Vincristine is used It is used to treat acute lymphocytic leukemia and can cause
to treat Hodgkin’s disease, acute lymphoblastic leukemia, allergic reactions, including anaphylaxis. Pegaspargase (On-
and non-Hodgkin’s lymphomas. Vinblastine is used to treat caspar) is a modified formulation for people who are hyper-
Hodgkin’s disease and choriocarcinoma; vinorelbine is used sensitive to Elspar. Hydroxyurea acts in the S phase of the cell
to treat non–small cell lung cancer. The drugs can cause se- cycle to impair DNA synthesis. It is used to treat leukemia,
vere tissue damage with extravasation (leaking of medication melanoma, and advanced ovarian cancer. A major adverse
into soft tissues around the venipuncture site). In addition, effect is myelosuppression. Procarbazine inhibits DNA, RNA,
vinblastine and vinorelbine are more likely to cause bone and protein synthesis. It is used to treat Hodgkin’s disease. It
marrow depression, and vincristine is more likely to cause is a monoamine oxidase inhibitor and may cause hypertension
peripheral nerve toxicity. if given with adrenergic drugs, tricyclic antidepressants, or
foods with high tyramine content (see Chap. 10). Common
adverse effects include leukopenia and thrombocytopenia.
Monoclonal Antibodies
Miscellaneous biotherapy agents include interferons (see
Monoclonal antibodies (see Chap. 45) are produced from one Chap. 44) and imatinib (Gleevec). Interferon alfa (Roferon-A,
cell line. For antitumor effects in cancer, they are designed to Intron A) is used to treat hairy cell leukemia, chronic my-
combine with growth factor receptors on malignant cell sur- elogenous leukemia, Kaposi’s sarcoma, and other cancers.
faces and inhibit tumor growth. Researchers also conjugate Imatinib is a tyrosine kinase inhibitor that inhibits cell pro-
monoclonal antibodies with radioisotopes, toxins, chemother- liferation and increases cell death in chronic myelogenous
apeutic agents, and drug-filled liposomes to increase their leukemia. It is also used to treat a rare type of cancer called
effectiveness and deliver antineoplastic drugs to specific areas gastrointestinal stromal tumor and is being investigated for
of the body. use in other cancers. It is given orally and its side effects
Cancer cells have more growth factor receptors than healthy include edema, cramps, nausea, and anemia.
cells. For example, 20% to 30% of women with breast cancer
have an excessive number of HER2 receptors. A monoclonal
Hormones and Hormone Inhibitors
antibody, trastuzumab (Herceptin), was developed specifi-
cally to bind with HER2 receptors and inhibit malignant cell Hormones interfere with protein synthesis and inhibit tumor
growth. This antibody is used with other antineoplastic drugs growth in hormone-dependent tissues. The goal of therapy is
to improve response in women with metastatic breast can- control of tumor growth and palliation of symptoms rather
cer. A major adverse effect is the development of congestive than cure. Hormones are not cytotoxic and adverse effects are
heart failure. The drug should not be used with doxorubicin usually mild.
or cyclophosphamide, because of increased risks of cardio- Sex hormones (estrogens, progestins, androgens) are use-
vascular toxicity. ful in cancers of the breast, prostate gland, and other repro-
Other monoclonal antibodies available for clinical use in- ductive organs. Adrenal corticosteroids suppress formation
clude alemtuzumab (Campath IH), ibritumomab tiuxetan and function of lymphocytes and therefore are most useful in
(Zevalin), gemtuzumab (Mylotarg), and rituximab (Rituxan). the treatment of leukemia and lymphoma. They are also used
Alemtuzumab binds to molecules on T and B cells in lympho- for complications of cancer (eg, brain metastases, hypercal-
cytic leukemia. Major adverse effects include allergic reac- cemia) and with radiation therapy to reduce radiation-related
tions, leukopenia, and pancytopenia. Because of the high risk edema in the mediastinum, brain, and spinal cord. Dexa-
of infection, patients are treated prophylactically with anti- methasone is commonly used in neurologic disorders.
biotic, antifungal, and antiviral drugs during and for 3 months Hormone inhibitors include aromatase inhibitors
after therapy. Gemtuzumab, an antibody conjugated with an (eg, anastrozole) that inhibit estrogen synthesis, antiestrogens
antitumor antibiotic, is used to treat acute myeloid leukemia. (eg, tamoxifen) that bind to estrogen receptors and block
7. CHAPTER 64 DRUGS USED IN ONCOLOGIC DISORDERS 919
estrogen action; aminoglutethimide, an adrenocorticosteroid- mia, malnutrition, weight loss, pain, and infection; specific
inhibiting agent that produces a “medical adrenalectomy”; manifestations depend on the organs affected.
and goserelin and leuprolide, which inhibit testosterone se- Assess for other diseases and organ dysfunctions (eg, car-
cretion in advanced prostatic cancer and inhibit production of diac, renal or hepatic) that influence response to chemo-
estrogen in advanced breast cancer. therapy.
Assess emotional status, coping mechanisms, family
relationships, and financial resources. Anxiety and depres-
INDIVIDUAL DRUGS sion are common features during cancer diagnosis and
treatment.
Cytotoxic antineoplastic drugs are listed in Drugs at a Glance: Assess laboratory test results before chemotherapy to es-
Cytotoxic Antineoplastic Drugs; hormones and hormone in- tablish baseline data and during chemotherapy to monitor
hibitors are listed in Drugs at a Glance: Antineoplastic Hor- drug effects:
mones and Hormone Inhibitors.
• Blood tests for tumor markers (tumor-specific antigens
on cell surfaces). Alpha-fetoprotein is a fetal antigen nor-
CYTOPROTECTANT DRUGS mally present during intrauterine and early postnatal life
but absent in adulthood. Increased amounts may indicate
Cytoprotectants reduce the adverse effects of cytotoxic drugs, hepatic or testicular cancer. Carcinoembryonic antigen
which may be severe, debilitating, and life threatening (CEA) is secreted by several types of malignant cells (eg,
(Box 64–2). Severe adverse effects may also limit drug CEA is present in approximately 75% of people with
dosage or frequency of administration, thereby limiting the colorectal cancer). A rising level may indicate tumor pro-
effectiveness of chemotherapy. Several cytoprotectants are gression and levels that are elevated before surgery and
available to protect certain body tissues from one or more ad- disappear after surgery indicate adequate tumor excision.
verse effects and allow a more optimal dose and schedule of If CEA levels rise later, it probably indicates tumor re-
cytotoxic agents. To be effective, administration and sched- currence. In chemotherapy, falling CEA levels indicate
uling must be precise in relation to administration of the effectiveness. Other tumor markers are immunoglobulins
cytotoxic agent. A cytoprotective agent does not prevent or (elevated levels may indicate multiple myeloma) and
treat all adverse effects of a particular cytotoxic agent and it prostate-specific antigen (elevated levels may indicate
may have adverse effects of its own. prostatic cancer).
Amifostine produces a metabolite that combines with • Complete blood cell count (CBC) to check for anemia,
cisplatin and ameliorates cisplatin-induced renal damage. leukopenia, and thrombocytopenia because most cyto-
Dexrazoxane decreases cardiac toxicity of doxorubicin. toxic antineoplastic drugs cause bone marrow depression.
Erythropoietin, filgrastim, oprelvekin, and sargramostim A CBC and white blood cell differential are done before
are colony-stimulating factors (see Chap. 44) that stimulate each cycle of chemotherapy to determine dosage and fre-
the bone marrow to produce blood cells. Erythropoietin stim- quency of drug administration, to monitor bone marrow
ulates production of red blood cells and is used for anemia; function so fatal bone marrow depression does not occur,
oprelvekin stimulates production of platelets and is used to and to assist the nurse in planning care. For example, the
prevent thrombocytopenia; filgrastim and sargramostim stim- client is very susceptible to infection when the leukocyte
ulate production of white blood cells and are used to reduce count is low, and bleeding is likely when the platelet
neutropenia and the risk of severe infection. Leucovorin is count is low.
used with high-dose MTX. Mesna is used with ifosfamide, • Other tests. These include tests of kidney and liver func-
which produces a metabolite that causes hemorrhagic cysti- tion, serum calcium, uric acid, and others, depending on
tis. Mesna combines with and inactivates the metabolite and the organs affected by the cancer or its treatment.
thereby decreases cystitis. Dosages and routes of adminis- Nursing Diagnoses
tration for these medications are listed in Drugs at a Glance:
• Pain, nausea and vomiting, weakness, and activity intol-
Cytoprotective Agents.
erance related to disease process or chemotherapy
• Imbalanced Nutrition: Less Than Body Requirements re-
lated to disease process or chemotherapy
• Anxiety related to the disease, its possible progression,
Nursing Process and its treatment
• Ineffective Family Coping related to illness and treatment
Assessment of a family member
Assess the client’s condition before chemotherapy is started • Deficient Fluid Volume related to chemotherapy-induced
and often during treatment. Useful information includes the nausea, vomiting, and diarrhea
type, grade, and stage of the tumor as well as the signs and • Risk for Injury: Infection related to drug-induced neu-
symptoms of cancer. General manifestations include ane- tropenia; bleeding related to drug-induced thrombo-
8. 920 SECTION 11 DRUGS USED IN SPECIAL CONDITIONS
cytopenia; stomatitis related to damage of GI mucosal • Physiologic care includes pain management, comfort
cells measures, and assistance with nutrition, hygiene, ambu-
• Deficient Knowledge about cancer chemotherapy and lation, and other activities of daily living as needed.
managing adverse drug effects • Psychological care includes allowing family members or
significant others to be with the client and participate in
Planning/Goals care when desired, and keeping clients and families in-
The client will: formed.
• Receive assistance in coping with the diagnosis of cancer
Evaluation
• Experience reduced anxiety and fear
• Receive chemotherapy accurately and safely • Monitor drug administration for accuracy.
• Experience reduction of tumor size, change of laboratory • Observe and interview for therapeutic effects of chemo-
values toward normal, or other therapeutic effects of therapy.
chemotherapy • Compare current laboratory reports with baseline values
• Experience minimal bleeding, infection, nausea and vom- for changes toward normal values.
iting, and other consequences of chemotherapy • Compare weight and nutritional status with baseline val-
• Maintain adequate food and fluid intake and body weight ues for maintenance or improvement.
• Receive assistance in activities of daily living when • Observe and interview for adverse drug effects and inter-
needed ventions to prevent or manage them.
• Be informed about community resources for cancer care • Observe and interview for adequate pain management
(eg, hospice, Reach to Recovery, other support groups) and other symptom control.
Interventions
Participate in and promote efforts to prevent cancer.
• Follow and promote the diet recommended by the PRINCIPLES OF THERAPY
American Cancer Society (ie, decrease fat; eat five or
more servings of fruits and vegetables daily; increase in- Overview of Cancer Treatment
take of dietary fiber; minimize intake of salt-cured or
smoked foods). Most cancer treatment involves surgery, radiation, and chemo-
• Promote weight control. Obesity may contribute to the therapy. Optimal regimens maximize effectiveness (eg, attempt
development of several cancers, including breast and en- to eradicate tumor cells at primary, regional, and systemic
dometrial cancer in women. sites) and minimize morbidity (eg, pain and treatment-
• Identify cancer-causing agents and strategies to reduce related toxicity).
exposure to them when possible. Surgery is used to excise small, localized tumors, which
• Strengthen host defenses by promoting a healthful may be curative; to remove tumors that have been reduced in
lifestyle (eg, good nutrition, adequate rest and exercise, size by radiation therapy, chemotherapy, or both; and to treat
stress management techniques, avoiding or minimizing complications of cancer, such as bowel obstruction. Surgical
alcohol and tobacco use). risks are greater in clients who have received preoperative
• Avoid smoking cigarettes and being around smokers. radiation therapy or chemotherapy.
Passive smoking increases risk of lung cancer in spouses Radiation therapy is used to treat most types of cancer.
of smokers and risks of brain cancer, lymphomas, and It may be used alone to cure some malignancies such as
acute lymphogenous leukemia in children of smokers. Hodgkin’s disease or cervical cancer. It may be used with
• Minimize exposure to sunlight, use sunscreens liber- surgery to reduce the need for radical surgery (eg, in breast
ally, and wear protective clothing to prevent skin cancer. cancer, excision of small tumors plus radiation therapy is as
Participate in and promote cancer screening tests in non- effective as mastectomy). With soft tissue sarcomas of the
symptomatic people, especially those at high risk, to detect limbs, wide excision plus radiation therapy can be used in-
cancer before signs and symptoms occur. These tests in- stead of amputation. Radiation is also used to eliminate local
clude regular examination of breasts, testicles, and skin and or regional malignant cells (eg, positive lymph nodes) that re-
tests for colon cancer such as hemoccult tests on stool and main after surgery; with chemotherapy to cure or control
sigmoidoscopy. Early recognition of risk factors, premalig- growth of tumors; and as a palliative treatment in metastatic
nant tissue changes (dysplasia), biochemical tumor mark- disease, such as relieving symptoms in clients with bone or
ers, and beginning malignancies may be lifesaving; early
brain involvement.
treatment can greatly reduce the suffering and problems as-
Cytotoxic chemotherapy is most effective when started be-
sociated with advanced cancer.
fore extensive tumor growth or when the tumor burden has
For clients receiving cytotoxic anticancer drugs, try to
been reduced by surgical excision or radiation therapy. Once
prevent or minimize the incidence and severity of adverse
metastasized, solid tumors become systemic diseases and are
reactions (Box 64-2).
not accessible to surgical excision or radiation therapy.
Provide supportive care to clients and families.
(text continues on page 925)
9. CHAPTER 64 DRUGS USED IN ONCOLOGIC DISORDERS 921
Drugs at a Glance: Cytotoxic Antineoplastic Drugs
Generic/Trade Name Routes and Dosage Ranges* Clinical Uses Adverse Effects
Alkylating Drugs
NITROGEN MUSTARD DERIVATIVES
Chlorambucil (Leukeran) PO 0.1–0.2 mg/kg/d for 3–6 wk. Main- Chronic lymphocytic leukemia, Bone marrow depression, hepato-
tenance therapy, 0.03–0.1 mg/kg/d Hodgkin’s and non-Hodgkin’s toxicity, secondary leukemia
lymphomas
Cyclophosphamide Induction therapy, PO 1–5 mg/kg/d; IV Hodgkin’s disease, non- Bone marrow depression, nausea,
(Cytoxan) 20–40 mg/kg in divided doses over Hodgkin’s lymphomas, vomiting, alopecia, hemorrhagic
2–5 days. Maintenance therapy, leukemias, cancer of breast, cystitis, hypersensitivity reac-
PO 1–5 mg/kg daily lung or ovary, multiple tions, secondary leukemia or
myeloma, neuroblastoma bladder cancer
Ifosfamide (Ifex) IV 1.2 g/m2/d for 5 consecutive d. Re- Germ cell testicular cancer Bone marrow depression, hemor-
peat every 3 wk or after white blood rhagic cystitis, nausea and vom-
cell and platelet counts return to nor- iting, alopecia, CNS depression,
mal after a dose. seizures
Melphalan (Alkeran) PO 6 mg/d for 2–3 wk, then 28 drug- Multiple myeloma, ovarian Bone marrow depression, nausea
free days, then 2 mg daily cancer and vomiting, hypersensitivity
IV 16 mg/m2 every 2 wk for 4 doses, reactions
then every 4 wk
NITROSOUREAS
Carmustine (BiCNU, IV 150–200 mg/m2 every 6 wk Hodgkin’s disease, non- Bone marrow depression, nausea,
Gliadel) Wafer, implanted in brain after tumor Hodgkin’s lymphomas, mul- vomiting
resection tiple myeloma, brain tumors
Lomustine (CCNU) PO 130 mg/m2 every 6 wk Hodgkin’s disease, brain Nausea and vomiting, bone mar-
tumors row depression
PLATINUM COMPOUNDS
Carboplatin (Paraplatin) IV infusion 360 mg/m2 on day 1 every Palliation of ovarian cancer Bone marrow depression, nausea
4 wk and vomiting, nephrotoxicity
Cisplatin (Platinol) IV 100 mg/m2 once every 4 wk Advanced carcinomas of Nausea, vomiting, anaphylaxis,
testes, bladder, ovary nephrotoxicity, bone marrow
depression, ototoxicity
Oxaliplatin (Eloxatin) IV infusion 85 mg/m2 every 2 wk Advanced colon cancer Anaphylaxis, anemia, increased
risk of bleeding or infection
Antimetabolites
Capecitabine (Xeloda) PO 1250 mg/m2 q12h for 2 wk, then a Metastatic breast cancer, col- Bone marrow depression, nausea,
rest period of 1 wk, then repeat cycle orectal cancer vomiting, diarrhea, mucositis
Cladribine (Leustatin) IV infusion 0.09 mg/kg/d for Hairy cell leukemia Bone marrow depression, nausea,
7 consecutive d vomiting
Cytarabine (Cytosar-U) IV infusion 100 mg/m2/d for 7 d Leukemias of adults and Bone marrow depression, nausea,
children vomiting, anaphylaxis, mucositis,
diarrhea
Fludarabine (Fludara) IV 25 mg/m2/d for 5 consecutive d; Chronic lymphocytic leukemia Bone marrow depression, nausea,
repeat every 28 d vomiting, diarrhea
Fluorouracil (5-FU) IV 12 mg/kg/d for 4 d, then 6 mg/kg Carcinomas of the breast, Bone marrow depression, nausea,
(Adrucil, Efudex, every other day for 4 doses colon, stomach, and vomiting, mucositis
Fluoroplex) Topical, apply to skin cancer lesion pancreas Pain, pruritus, burning at site of
twice daily for several weeks Solar keratoses, basal cell car- application
cinoma
Gemcitabine (Gemzar) IV 1000 mg/m2 once weekly up to 7 wk Lung and pancreatic cancer Bone marrow depression, nausea,
or toxicity, withhold for 1 wk, then vomiting, flu-like symptoms, skin
once weekly for 3 wk and withhold rash
for 1 wk
Mercaptopurine PO 2.5 mg/kg/d Acute and chronic leukemias Bone marrow depression, nausea,
(Purinethol) (100–200 mg for average adult) vomiting, mucositis
Methotrexate (MTX) Acute leukemia in children, induction, Leukemias, non-Hodgkin’s Bone marrow depression, nausea,
(Rheumatrex) PO, IV 3 mg/m2/d; maintenance, lymphomas, osteosarcoma, vomiting, mucositis, diarrhea,
PO 30 mg/m2 twice weekly choriocarcinoma of testes, fever, alopecia
Choriocarcinoma, PO, IM 15 mg/m2 cancers of breast, lung,
daily for 5 d head and neck
(continued )
10. 922 SECTION 11 DRUGS USED IN SPECIAL CONDITIONS
Drugs at a Glance: Cytotoxic Antineoplastic Drugs (continued )
Generic/Trade Name Routes and Dosage Ranges* Clinical Uses Adverse Effects
Antitumor Antibiotics
Bleomycin (Blenoxane) IV, IM, SC 0.25–0.5 units/kg once or Squamous cell carcinoma, Pulmonary toxicity, mucositis,
twice weekly Hodgkin’s and non- alopecia, nausea, vomiting,
Hodgkin’s lymphomas, tes- hypersensitivity reactions
ticular carcinoma
Dactinomycin IV 15 mcg/kg/d for 5 d and repeated Rhabdomyosarcoma, Wilms’ Bone marrow depression, nausea,
(Actinomycin D, every 2–4 wk tumor, choriocarcinoma, vomiting. Extravasation may
Cosmegen) testicular carcinoma, lead to tissue necrosis.
Ewing’s sarcoma
Daunorubicin IV 25–45 mg/m2 daily for 3 d every Acute leukemias, lymphomas Same as doxorubicin, below
conventional 3–4 wk
Daunorubicin liposomal IV infusion, 40 mg/m2 every 2 wk AIDS-related Kaposi’s Bone marrow depression, nausea,
(DaunoXome) sarcoma vomiting
Doxorubicin conventional Adults, IV 60–75 mg/m2 every 21 d Acute leukemias, lymphomas, Bone marrow depression, alope-
(Adriamycin) Children, IV 30 mg/m2 daily for 3 d, carcinomas of breast, lung, cia, mucositis, GI upset,
repeated every 4 wk and ovary cardiomyopathy. Extravasation
may lead to tissue necrosis.
Doxorubicin liposomal IV infusion, 20 mg/m2, once every 3 wk AIDS-related Kaposi’s sar- Bone marrow depression, nausea,
(Doxil) coma vomiting, fever, alopecia
Epirubicin (Ellence) IV infusion 120 mg/m2 every 3–4 wk Breast cancer Cardiotoxicity
Idarubicin (Idamycin) IV injection 12 mg/m2/d for 3 d, with Acute myeloid leukemia Same as doxorubicin, above
cytarabine
Mitomycin (Mutamycin) IV 20 mg/m2 every 6–8 wk Metastatic carcinomas of Bone marrow depression, nausea,
stomach and pancreas vomiting. Extravasation may
lead to tissue necrosis.
Mitoxantrone (Novantrone) IV infusion 12 mg/m2 on days 1–3, for Acute nonlymphocytic Bone marrow depression, conges-
induction of remission in leukemia leukemia, prostate cancer tive heart failure, nausea
Pentostatin (Nipent) IV 4 mg/m2 every other week Hairy cell leukemia unrespon- Bone marrow depression, hepato-
sive to alpha-interferon toxicity, nausea, vomiting
Valrubicin (Valstar) Intravesically, 800 mg once weekly for Bladder cancer Dysuria, urgency, frequency, blad-
6 wk der spasms, hematuria
Plant Alkaloids
CAMPTOTHECINS
Irinotecan (Camptosar) IV infusion, 125 mg/m2 once weekly Metastatic cancer of colon or Bone marrow depression, diarrhea
for 4 wk, then a 2-wk rest period; rectum
repeat regimen
Topetecan (Hycamtin) IV infusion 1.5 mg/m2 daily for 5 con- Advanced ovarian cancer, Bone marrow depression, nausea,
secutive days every 21 d small-cell lung cancer vomiting, diarrhea
PODOPHYLLOTOXINS
Etoposide (VePesid) IV 50–100 mg/m2/d on days 1–5, or Testicular cancer, small-cell Bone marrow depression, allergic
100 mg/m2/d on days 1, 3, and lung cancer reactions, nausea, vomiting,
5, every 3–4 wk alopecia
PO 2 times the IV dose
Teniposide (Vumon) IV infusion 165 mg/m2 twice weekly for Acute lymphocytic leukemia in Same as etoposide, above
8–9 doses children
TAXANES
Docetaxel (Taxotere) IV infusion 60–100 mg/m2, every 3 wk Advanced breast cancer, Bone marrow depression, nausea,
non–small cell lung cancer vomiting, hypersensitivity reac-
tions,
Paclitaxel (Taxol) IV infusion 135 mg/m2 every 3 wk Advanced ovarian cancer, Bone marrow depression, allergic
advanced breast cancer, reactions, hypotension, brady-
non–small cell lung cancer, cardia, nausea, vomiting
AIDS-related Kaposi’s
sarcoma
VINCA ALKALOIDS
Vinblastine (Velban) Adults, IV 3.7–11.1 mg/m2 (average Metastatic testicular carci- Bone marrow depression, nausea,
5.5–7.4 mg/m2) weekly noma, Hodgkin’s disease vomiting. Extravasation may
Children, IV 2.5–7.5 mg/m2 weekly lead to tissue necrosis.
Vincristine (Oncovin) Adults, IV 1.4 mg/m2 weekly Hodgkin’s and other lym- Peripheral neuropathy. Extravasa-
Children, IV 2 mg/m2 weekly phomas, acute leukemia, tion may lead to tissue necrosis.
neuroblastoma, Wilms’ tumor
(continued )
11. CHAPTER 64 DRUGS USED IN ONCOLOGIC DISORDERS 923
Drugs at a Glance: Cytotoxic Antineoplastic Drugs (continued )
Generic/Trade Name Routes and Dosage Ranges* Clinical Uses Adverse Effects
Vinorelbine (Navelbine) 2
IV injection 30 mg/m once weekly Non–small cell lung cancer Bone marrow depression, periph-
eral neuropathy. Extravasation
may lead to tissue necrosis.
Monoclonal Antibodies
Gemtuzumab ozogamicin IV infusion, 9 mg/m2, for 2 doses, 14 d Acute myeloid leukemia Chills, fever, nausea, vomiting,
(Mylotarg) apart diarrhea
Ibritumomab tiuxetan See literature Non-Hodgkin’s lymphoma, with Severe or fatal infusion reaction,
(Zevalin) rituximab severe bone marrow depression
Rituximab (Rituxan) IV infusion, 375 mg/m2 once weekly Non-Hodgkin’s lymphoma Hypersensitivity reactions, cardiac
for 4 doses dysrhythmias
Trastuzumab (Herceptin) IV infusion, 4 mg/kg, then 2 mg/kg Metastatic breast cancer Cardiotoxicity (dyspnea, edema,
once weekly heart failure)
Miscellaneous Agents
L-Asparaginase (Elspar) IV 1000 IU/kg/d for 10 d Acute lymphocytic leukemia Hypersensitivity reactions, includ-
ing anaphylaxis
Hydroxyurea (Hydrea) PO 80 mg/kg as a single dose every Chronic myelocytic leukemia, Bone marrow depression, nausea,
third day or 20–30 mg/kg as a single melanoma, ovarian cancer, vomiting, peripheral neuritis
dose daily head and neck cancer
Levamisole (Ergamisol) PO 50 mg q8h for 3 d every 2 wk Colon cancer, with fluorouracil Nausea, vomiting, diarrhea
Procarbazine (Matulane) PO 2–4 mg/kg/d for 1 wk, then Hodgkin’s disease Bone marrow depression, mucosi-
4–6 mg/kg/d tis, CNS depression
Temozolomide (Temodar) PO 150 mg/m2 once daily for 5 d, then Brain tumors Bone marrow depression
200 mg/m2 every 28 d
*Dosages may vary significantly or change often, according to use in different types of cancer and in different combinations.
AIDS, acquired immunodeficiency syndrome.
Drugs at a Glance: Antineoplastic Hormones and Hormone Inhibitors
Generic/Trade Names Routes and Dosage Ranges Clinical Uses Adverse Effects
Antiestrogens
Fulvestrant (Faslodex) IM 250 mg once monthly (one 5-mL Advanced breast cancer in GI upset, hot flashes, injection site
or two 2.5-mL injections) postmenopausal women reactions
Tamoxifen (Nolvadex) PO 20 mg once or twice daily Breast cancer: after surgery or Hot flashes, nausea, vomiting, vaginal
radiation; prophylaxis in discharge, risk of endometrial can-
high-risk women; and treat- cer in nonhysterectomized women
ment of metastatic disease
Toremifene (Fareston) PO 60 mg once daily Metastatic breast cancer in Hot flashes, nausea, hypercalcemia,
postmenopausal women tumor flare
Aromatase Inhibitors
Anastrazole (Arimidex) PO 1 mg once daily Advanced breast cancer in Nausea, hot flashes, edema
postmenopausal women
Exemestane (Aromasin) PO 25 mg once daily Advanced breast cancer in Hot flashes, nausea, depression, in-
postmenopausal women somnia, anxiety, dyspnea, pain
Letrozole (Femara) PO 2.5 mg once daily Advanced breast cancer Nausea, hot flashes
Goserelin (Zoladex) SC implant, 3.6 mg every 28 d or Advanced prostatic or breast Hot flashes, transient increase in
10.8 mg every 12 wk cancer, endometriosis bone pain
Leuprolide (Eligard, SC 7.5 mg/mo Advanced prostatic cancer Same as for goserelin, above
Lupron, Viadur) IM 7.5 mg/mo, 22.5 mg/3 mo, or
30 mg/4 mo
IM implant 65 mg/12 mo
Triptorelin (Trelstar LA, IM 3.75 mg/28 d or 11.25 mg/3 mo Advanced prostatic cancer Same as for goserelin and leuprolide,
Trelstar Depot) above
12. 924 SECTION 11 DRUGS USED IN SPECIAL CONDITIONS
BOX 64-2
MANAGEMENT OF CHEMOTHERAPY COMPLICATIONS
Complications may range from minor to life threatening. System- • Inspect the mouth daily for signs of inflammation and lesions.
atic efforts toward prevention or early detection and treatment are • Give medications for pain. Local anesthetic solutions, such as
needed. viscous lidocaine, can be taken a few minutes before meals.
• Nausea and vomiting commonly occur. They are usually treated Because the mouth and throat are anesthetized, swallowing and
with antiemetics (see Chap. 63), which are most effective when detecting the temperature of hot foods may be difficult, and
started before chemotherapy and continued on a regular sched- aspiration or burns may occur. Doses should not exceed 15 mL
ule for 24 to 48 hours afterward. An effective regimen is a sero- every 3 hours or 120 mL in 24 hours. If systemic analgesics
tonin receptor antagonist (eg, ondansetron) and a corticosteroid are used, they should be taken 30 to 60 minutes before eating.
(eg, dexamethasone), given orally or intravenously (IV). Other • In oral infections resulting from mucositis, local or systemic
measures include a benzodiazepine (eg, lorazepam) for anticipa- antimicrobial drugs are used. Fungal infections with Candida
tory nausea and vomiting and limiting oral intake for a few hours. albicans can be treated with antifungal tablets, suspensions, or
• Anorexia interferes with nutrition. Well-balanced meals, with lozenges. Severe infections may require systemic antibiotics,
foods the client is able and willing to eat, and nutritional supple- depending on the causative organism as identified by cultures
ments, to increase intake of protein and calories, are helpful. of mouth lesions.
• Fatigue, which may be profound, is often caused or aggravated • Infection is common because the disease and its treatment lower
by anemia and can be prevented or treated with administration of host resistance to infection.
erythropoietin. An adequate diet and light to moderate exercise, • Help the client maintain a well-balanced diet. Oral hygiene
as tolerated, may also be helpful. and analgesics before meals may increase food intake. High-
• Alopecia occurs with several drugs, including cyclophospha- protein, high-calorie foods and fluids can be given between
mide, doxorubicin, methotrexate, and vincristine. Complete hair meals. Nutritional supplements can be taken with or between
loss can be psychologically devastating, especially for women. meals. Provide fluids with high nutritional value (eg, milk-
Helpful measures include the following: shakes or nutritional supplements) if the client can tolerate
• Counsel clients that hair loss is likely but that it is temporary them and has an adequate intake of water and other fluids.
and that hair may grow back a different color and texture. • Instruct the client to avoid exposure to infection by avoiding
• Suggest the purchase of wigs, hats, and scarves before hair loss crowds, anyone with a known infection, and contact with fresh
is expected to occur. flowers, soil, animals, or animal excrement.
• Suggest using a mild shampoo and avoiding rollers, hair dry- • Frequent and thorough handwashing by the client and every-
ers, permanent waves, hair coloring, and other treatments that one involved in his or her care is necessary to reduce exposure
damage the hair and may increase hair loss. to pathogenic microorganisms.
• Mucositis (also called stomatitis) occurs often with the anti- • The client should take a bath daily and put on clean clothes. In
metabolites, antibiotics, and plant alkaloids and usually lasts 7 addition, the perineal area should be washed with soap and
to 10 days. It may interfere with nutrition; lead to oral ulcera- water after each urination or defecation.
tions, infections, and bleeding; and cause pain. Nurse or client • When venous access devices are used, take care to prevent
interventions to minimize or treat mucositis include: them from becoming sources of infection. For implanted
• Brush the teeth after meals and at bedtime with a soft tooth- catheters, inspect and cleanse around exit sites according
brush and floss once daily with unwaxed floss. Stop brushing to agency policies and procedures. Use strict sterile technique
and flossing if the platelet count drops below 20,000/mm3 be- when changing dressings or flushing the catheters. For peri-
cause gingival bleeding is likely. Teeth may then be cleaned pheral venous lines, the same principles of care apply,
with soft, sponge-tipped or cotton-tipped applicators. except that sites should be changed every 3 days or if signs of
• Rinse the mouth several times daily, especially before meals phlebitis occur.
(to decrease unpleasant taste and increase appetite) and after • Avoid indwelling urinary catheters when possible. When they
meals (to remove food particles that promote growth of micro- are necessary, cleanse the perineal area with soap and water
organisms). One suggested solution is 1 tsp of table salt and at least once daily and provide sufficient fluids to ensure an
1 tsp of baking soda in 1 quart of water. adequate urine output.
• Encourage the client to drink fluids. Systemic dehydration and • If fever occurs, especially in a neutropenic client, possible
local dryness of the oral mucosa contribute to the development sources of infection are usually cultured and antibiotics are
and progression of mucositis. Pain and soreness contribute to started immediately.
dehydration. Fluids usually tolerated include tea, carbonated • Severe neutropenia can be prevented or its extent and dura-
beverages, ices (eg, popsicles), and plain gelatin desserts. Fruit tion minimized by administering filgrastim or sargramostim
juices may be diluted with water, ginger ale, Sprite, or 7-Up to to stimulate the bone marrow to produce leukocytes. A pro-
decrease pain, burning, and further tissue irritation. Drinking tective environment may be needed to decrease exposure to
fluids through a straw may be more comfortable, because this pathogens.
decreases contact of fluids with painful ulcerations. • Bleeding may be caused by thrombocytopenia and may occur
• Encourage the client to eat soft, bland, cold, nonacidic foods. spontaneously or with minor trauma. Precautions should be insti-
Although individual tolerances vary, it is usually better to tuted if the platelet count drops to 50,000/mm3 or below. Mea-
avoid highly spiced or rough foods. sures to avoid bleeding include:
• Remove dentures entirely or for at least 8 hours daily because • Giving oprelvekin to stimulate platelet production and pre-
they may irritate oral mucosa. vent thrombocytopenia.
(continued)
13. CHAPTER 64 DRUGS USED IN ONCOLOGIC DISORDERS 925
BOX 64-2
MANAGEMENT OF CHEMOTHERAPY COMPLICATIONS (Continued)
• Avoiding trauma, including venipuncture and injections, when the client about pain or burning. After a drug has been injected,
possible. continue the rapid flow rate of the IV fluid for 2 to 5 minutes
• Using an electric razor for shaving. to flush the vein.
• Checking skin, urine, and stool for blood. If using a central IV line, do not give the drug unless pa-
• For platelet counts less than 20,000/mm3, stop brushing the tency is indicated by a blood return. Using a central line does
teeth. not eliminate the risk of extravasation.
• Extravasation. Several drugs (called vesicants) cause severe • When extravasation occurs, the drug should be stopped im-
inflammation, pain, ulceration, and tissue necrosis if they leak mediately. Techniques to decrease tissue damage include aspi-
into soft tissues around veins. Thus, efforts are needed to pre- rating the drug (about 5 mL of blood, if able) through the IV
vent extravasation or to minimize tissue damage if it occurs. catheter before it is removed, elevating the involved extrem-
• Identify clients at risk for extravasation, including those who ity, and applying warm (with dacarbazine, etoposide, vinblas-
are unable to communicate (eg, sedated clients, infants), have tine, and vincristine) or cold compresses (with daunorubicin
vascular impairment (eg, from multiple attempts at venipunc- and doxorubicin). Nurses involved in chemotherapy must
ture), or have obstructed venous drainage after axillary node know the procedure to be followed if extravasation occurs
surgery. so it can be instituted immediately.
• Be especially cautious with the anthracyclines (eg, doxoru- • Hyperuricemia results from rapid breakdown of malignant
bicin) and the vinca alkaloids (eg, vincristine). Choose pe- cells, whether it occurs spontaneously or as a result of anti-
ripheral IV sites carefully, avoiding veins that are small or neoplastic drugs. Uric acid crystals can cause kidney damage.
located in an edematous extremity or near a joint. Inject the Interventions to minimize nephropathy include a high fluid in-
drugs slowly (1 to 2 mL at a time) into the tubing of a rapidly take, with IV fluids if necessary, and a high urine output; alka-
flowing IV infusion, for rapid dilution and detection of ex- linizing the urine with sodium bicarbonate or other agents; and
travasation. Observe the venipuncture site for swelling and ask giving allopurinol to inhibit uric acid formation.
Chemotherapy regimens should be managed by oncologists used in advanced cancer to relieve symptoms and treat or
experienced in use of the drugs; the consequences of inap- prevent complications.
propriate or erroneous drug therapy may be fatal for clients
(from the disease or the treatment).
Adjuvant chemotherapy is used after surgery or radiation Drug Selection Factors
to destroy or reduce microscopic metastases. It is often used
in the treatment of clients with carcinomas of the breast, Factors that determine drug choice include which drugs have
colon, lung, ovaries, or testes. Palliative chemotherapy is been effective in similar types of cancer; primary tumor sites;
Drugs at a Glance: Cytoprotective Agents
Generic/Trade Name Clinical Uses Routes and Dosage Ranges
Amifostine (Ethyol) Reduction of cisplatin-induced renal toxicity IV infusion 910 mg/m2 once daily within 30 min of
starting chemotherapy
Dexrazoxane (Zinecard) Reduction of doxorubicin-induced cardiomyopathy IV 10 times the amount of doxorubicin (eg, dexrazox-
in women with metastatic breast cancer who ane 500 mg/m2 per doxorubicin 50 mg/m2), then
have received a cumulative dose of 300 mg/m2 give doxorubicin within 30 min of completing dexra-
and need additional doxorubicin zoxane dose
Erythropoietin (Epogen, Treatment of chemotherapy-induced anemia SC 150–300 units/kg 3 times weekly, adjusted to
Procrit) maintain desired hematocrit
Filgrastim (Neupogen) Treatment of chemotherapy-induced neutropenia SC, IV 5 mcg/kg/d, at least 24 h after cytotoxic
chemotherapy, up to 2 wk or an absolute neu-
trophil count of 10,000/mm3
Leucovorin (Wellcovorin) “Rescue” after high-dose methotrexate for os- “Rescue,” PO, IV, IM 15 mg q6h for 10 doses,
teosarcoma starting 24 h after methotrexate begun
Advanced colorectal cancer, with 5-fluorouracil Colorectal cancer, IV 20 mg/m2 or 200 mg/m2,
followed by 5-fluorouracil, daily for 5 d, repeated
every 28 d
Mesna (Mesnex) Prevention of ifosfamide-induced hemorrhagic IV, 20% of ifosfamide dose for 3 doses (at time of
cystitis ifosfamide dose, then 4 h and 8 h after ifosfamide
dose)
Oprelvekin (Neumega) Prevention of thrombocytopenia SC 50 mcg/kg once daily, usually for 10–21 d
Sargramostim (Leukine) Myeloid reconstitution after bone marrow trans- IV infusion 250 mcg/m2/d until absolute neutrophil
plant; to decrease chemotherapy-induced neu- count is >1500/mm3 for 3 d, up to 42 d
tropenia
14. 926 SECTION 11 DRUGS USED IN SPECIAL CONDITIONS
CLIENT TEACHING GUIDELINES
Managing Chemotherapy
Most chemotherapy is given intravenously, in outpatient clin- ✔ Inform any other physician, dentist, or health care provider
ics, by nurses who are specially trained to administer the med- that you are taking chemotherapy before any diagnostic
ications and monitor your condition. The medications are test or treatment is begun. Some procedures may be con-
usually given in cycles such as every few weeks. There are traindicated or require special precautions.
many different chemotherapy drugs, and the ones used for a ✔ If you are of childbearing age, effective contraceptive mea-
particular client depend on the type of malignancy, its location, sures should be carried out during and a few months after
and other factors. chemotherapy.
The goal of chemotherapy is to be as effective as possible ✔ A few chemotherapy medications and medications to pre-
with tolerable side effects. Particular side effects vary with the vent or treat side effects are taken at home. Instructions
medications used; some increase risks of infection, some for taking the drugs should be followed exactly for the
cause anemia, nausea, or hair loss. All of these can be man- most beneficial effects.
aged effectively, and several medications can help prevent or ✔ Although specific instructions vary with the drugs you are
minimize side effects. In addition, some helpful activities are taking, the following are a few precautions with some
listed below. commonly used drugs:
✔ Keep all appointments for chemotherapy, blood tests, ✔ With cyclophosphamide, take the tablets on an em-
and check-ups. This is extremely important. Chemother- pty stomach. If severe stomach upset occurs, take
apy effectiveness depends on its being given on time; with food. Also, drink 2 or 3 quarts of fluid daily, if
blood tests help to determine when the drugs should be possible, and urinate often, especially at bedtime. If
given and how the drugs affect your body tissues. blood is seen in the urine or signs of cystitis occur
✔ Do everything you can to avoid infection, such as avoid- (eg, burning with urination), report to a health care
ing other people who have infections and washing your provider. The drug is irritating to the bladder lining
hands frequently and thoroughly. If you have a fever, and may cause cystitis. High fluid intake and fre-
chills, sore throat, or cough, notify your oncologist. quent emptying of the bladder help to decrease blad-
✔ Try to maintain or improve your intake of nutritious food der damage.
and fluids; this will help you feel better. A dietitian can be ✔ With doxorubicin, the urine may turn red for 1 to 2 days
helpful in designing a diet to meet your needs. after drug administration. This discoloration is harm-
✔ If your chemotherapy may cause bleeding, you can de- less; it does not indicate bleeding. Also, report to a
crease the likelihood by shaving with an electric razor, health care provider if you have edema, shortness of
avoiding aspirin and other nonsteroidal anti-inflammatory breath, and excessive fatigue. Doxorubicin may need
drugs (including over-the-counter Advil, Aleve, and others), to be stopped if these symptoms occur.
and avoiding injections, cuts, and other injuries when pos- ✔ With fluorouracil, drink plenty of liquids while taking.
sible. If you notice excessive bruising, bleeding gums ✔ With methotrexate, avoid alcohol, aspirin, and pro-
when you brush your teeth, or blood in your urine or bowel longed exposure to sunlight.
movement, notify your oncologist immediately. ✔ With vincristine, eat high-fiber foods, such as raw
✔ If hair loss is expected with the medications you take, you fruits and vegetables and whole cereal grains, if you
can use wigs, scarves, and hats. These should be pur- are able, to prevent constipation. Also try to maintain
chased before starting chemotherapy, if possible. Hair a high fluid intake. A stool softener or bulk laxative
loss is temporary; your hair will grow back! may be prescribed for daily use.
presence and extent of metastases; and physical status of age the DNA, RNA, or proteins of the malignant cell,
the client, including other disease conditions that affect and another drug can be chosen to prevent their repair
chemotherapy, such as liver or kidney disease. Most regimens or synthesis.
use combinations of drugs because they are more effective, less • Drugs should act at different times in the reproductive
toxic, and less likely to cause drug resistance than single agents. cycle of the malignant cell. For example, more malig-
Numerous combinations have been developed for use in spe- nant cells are likely to be destroyed by combining cell
cific types of cancer. Selection and scheduling of individual cycle–specific and cell cycle–nonspecific drugs. The
drugs in a multidrug regimen are based on efforts to maximize first group kills only dividing cells; the second group
effectiveness and minimize adverse effects. Characteristics of kills cells during any part of the life cycle, including the
effective drug combinations include the following: resting phase.
• Each drug should have activity against the type of tumor • Consecutive doses kill a percentage of the tumor cells
being treated. remaining after earlier doses and further decrease the
• Each drug should act by a different mechanism. Drugs tumor burden.
can be combined to produce sequential or concurrent • Toxic reactions of the various drugs should not overlap
inhibition. For example, one drug can be chosen to dam- so that maximal tolerated doses may be given. It is