Rhinocerebral mucormycosis
•Als PPTX, PDF herunterladen•
14 gefällt mir•553 views

Mucormycosis in Covid-19 Pandemic

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Rhinocerebral mucormycosis
Ähnlich wie Rhinocerebral mucormycosis (20)
Mehr von Mahavir Mohire
Mehr von Mahavir Mohire (9)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Rhinocerebral mucormycosis
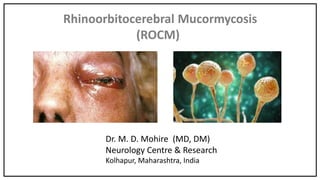
- 1. Rhinoorbitocerebral Mucormycosis (ROCM) Dr. M. D. Mohire (MD, DM) Neurology Centre & Research Kolhapur, Maharashtra, India
- 2. Overview Introduction, History & Epidemology Sources of infection Predisposing factors Clinical features Diagnosis Treatment Prognosis & mortality
- 3. Introduction Highly serious fungal infection in low immunity host Caused by fungus of Mucorales, species Rhizopus Incidence is 0.6 to 3 /1 million in Western countries. India 14 cases / 100,000 Persons, (Precovid) Males & Females are equally affected Incubation period for mucor is 3 to 15 days
- 4. Predisposing conditions Diabetes (T1DM & T2DM), with high sugar with/without ketoacidosis Cancer patients on chemotherapy Transplant cases on immunosupressants Autoimmune disorders on DMTs Leukemias & Lymphomas Covid-19 patients on steroids (CAM) IV Drug abusers
- 5. Mucormycosis [History] 1885 - CNS infection first described in man 1943 - Triad of T2DM, Ketoacidosis, nasoorbital necrosis, ketoacidosis, 1955 - First survival in 14 years girl with Diabetes treated with iodides. 1958 - Efficacy of Amphotericin established 1962 - Survival has improved with Amphotericin-B. 1980 - Liposomal Amphotericin B available
- 6. Classification of Mucormycosis Rhinoorbitocerebral mucormycosis (ROCM) : 50% Pumonary mucormycosis : 20% Gastrointestinal mucormycosis : 5% Cutaneous mucormycosis & other : 10% Disseminated mucormycosis 15% Covid-19 steroid induced mucormycosis (CAM)
- 7. Source of Infection Bread mold Dung Damp soil Rotten Fruits & Vegetables
- 8. Susceptibility for Mucormycosis Diabetes with/without ketoacidosis, Bad oral hygiene Transplant patients on immunosupressants, Cancer patients on chemotherapy ROCM frequent in Covid-19 Diabetics on steroids ROCM is slow in Nondiabetics
- 9. Covid Associated Mucormycosis (CAM) in india End of May 2021, over 10,000 cases are reported From Dec to Feb 2021 the infection rate is scorging rapidly Recorded from almost every state of India Diabetes in over 95 % of cases It is now declared to be National Emergency & Notifiable disease.
- 10. Covid Associated Mucormycosis (CAM) in India Dexamethasone reduce lung inflammation in Covid-19 pneumonia Steroids leads to shooting of blood sugar in diabetics Steroids impairs immunity Covid Diabetics requiring long admission Covid Diabetics requiring O2 for many days to weeks & ventilators Suboptimal hygiene of Industrial O2, Oxygen tank regulators & humidifier for O2 use are possible reasons for surge of mucormycosis
- 11. Covid Associated Mucor (CAM) Majority in India CAM is typically observed 10 to 20 days after discharge In India about 80 million people are diabetic Diabetes seen in 95 % of cases More than 70 % of all World cases cases in India
- 12. Symptoms of ROCM Mucormycosis Fulminating symptoms Aggressive spread is characteristic of CAM Nasal stuffiness, epistaxis, fever, diplopia, Blindness one or both sides, swollen face, Proptosis, red eyes Black/Bloody discharge from nostrils, Drowsiness, stroke on one side, seizures
- 13. Warning signs in Mucormycosis Redness around eyes, red eyes, epistaxis, severe headache, Uni or bilateral proptosis, toxic patient with fever
- 14. Mucormycosis (CAM) Typical Case. ESCHAR Swollen face, bilateral ptosis & Eschar
- 15. 62 Yrs.M, T2DM 30 years, Covid RT-PCR positive, HRCT Score 20, D-dimer, CRP high, treated with dexamethasone, Blood sugar 300 to 510 mgs during adm, oxygen for 10 days, . Discharged on day 15. Day 10 of discharge : Watering nose with cough Day 13 of discharge : Mild fever, severe headache without vomiting Day 14 of discharge : Sudden R eye visual loss Day 17 of discharge : R eye ptosis, R ext phthalmoplegia, R pupil dilated, R eye blind, & swollen face with proptosis Day 20 of discharge : L eye blindness, L ophthalmoplegia, R Proptosis Day 21 of discharge : Diagnosis ROCM on scrapings from nose, MRI showed Pansinusitis, Day 21 Liposomal Amphotericin B started, Died on 27 the day ROCM ‘Typical Case’
- 16. MRI scan showing sinusitis ROCM ‘Typical Case’ MRI head Sphenoid sinusitis Ethmoid & Maxillary sinusitis
- 17. Signs in ROCM Swollen face, ptosis one or both sides, black eschar at nostrils Sometimes black eschar on palate & pharyngeal walls Conjunctival oedema with chemosis & Proptosis Panophthalmitis One or both sides 2nd, 3rd, 4th, 5th 6th, 7th cranial nerves, (Cavernous sinus thrombosis uni or bilateral)
- 18. Typical Lesion of ROCM Eschar ( black necrotic tissue) Necrotic tissue is Black
- 19. Cavernous Sinus Thrombosis in ROCM Proptosis with loss of Vision is typical Cavernous Sinus Thrombosis one or both sides is frequently asscociated with Proptosis
- 20. ROCM lesions on Palate
- 21. Nasal Endoscopic Pictures of ROCM
- 22. Mucormycosis (ROCM) (Diagnosis) High suspicion in a diabetic or immune-compromised Neuro + ENT, Eye signs, MRI Head, Orbits , Angio & Veno Neuro + ENT + Eye signs + MRI = Certain Confirmed Tissue Diagnosis after Nasal Endoscopy
- 23. Mucormycosis (CNS Signs) Commonly involved is Optic Nerve Other Nerves involved : Cr Ns 3, 4, 5, 6, 7 & rarely 9, 10, & 11. Hemiparesis, Hemiplegia, seizures Altered sensorium Cavernous sinus thrombosis leads to 2, 3, 4, 6 Cr Ns dysfunction Cr Ns are invaded by angioinvasiveness & perineural spread
- 24. Clinical Staging of Rhinocerebral Mucormycosis First Stage : Blocked Nose, Congestion of Eyes, Swelling & numbness of Face Second Stage : Spread to Orbits, Headache & Orbital pain, Blindness, in one or both eyes Third Stage : Involvement of Jaw & Mouth, Fever, UC, Black Nose In 3rd Stage Brain is involved, Brain is involved in 20%.
- 25. Investigations Routine, RFT, LFT, Electrolytes, HbA1C, Urine & blood ketones Baseline MRI Head & Orbits with Angio & Veno Nasal scraping for KOH, & special Fungal stains Fungal culture on blood agar & special fungal media Diagnostic Nasal endoscopy (FESS) for Tissue diagnosis
- 26. Lab diagnosis Often difficult Scraping from nasal cavity mostly negative on microscopy Tissue biopsy on endoscopic aspiration is Positive Frozen tissue sections with special fungal stains are diagnostic Fungal cultures are diagnostic
- 27. ROCM Orbital Imaging T2-weighted MRI shows hyperintense sinuses & orbital hyperintense signal lesion displacing eyeball T2-MRI shows hyperintense ethmoid cells. Soft tissue swelling seen anterior to eyeball. orbital hyperintense signal along orbital apex into left cavernous sinus & internal carotid artery T1-weighted MRI shows hypointense mucosal thickening of left ethmoid cells.Soft tissue swelling seen anterior to eyeball,.orbital isointense along orbital apex into cavernous sinus. Lone et al, Ind J Otology,2015,21, 215-218.
- 28. Imaging Characters of Sinuses, Orbit, Face, Skull and Brain Showing Swollen Ext Ocular Muscles, Mass in sinuses & Bone Erosion Structures Involved Ethmoid sinus : 85 % Maxillary sinus : 80% Orbit : 76 % Face : 60% Brain : 15 % Skull base : 15 % Sphenoid sinus : Least common Frontal Sinus : Least common Multiple regions are involved in most cases
- 29. Brain involvement in ROCM Dissiminated mucormycosis (hematogenous) Diect extension in Frontal lobe Leptomeningeal Stroke Mass lesion Mass lesion Brain Abscess
- 30. Brain arterial & Venous involvement Int Carotid A Thrombosis R-Cavernous Sinus Thrombosis ROCM
- 31. Mechanism of Spread in between two cavernous sinuses Spread of Mucormycosis is very fast. Spread is ascending Angioinvasiveness. Spread is also ascending perineural through 3rd, 4th, 5th, 6th, & 7th Cranial nerves Dissiminated Hematogenous spread is also important.
- 32. Orbital Pathology in ROCM Congestion, Proptosis, Chemosis, Hemorrhage, abscess formation, Extensive necrosis Central tissue necrosis, with acute inflammatory exudate Invasion of Subcutaneous fat, orbital fat and fascial layers Thrombosing Arteritis, Veins less involved Superior Orbital Syndrome
- 33. Tissue Biopsies from nasal endoscopy & Orbit Nonseptate hyphae in Eosin and Hematoxylin
- 34. Ribes, J. A. et al. 2000. Clin. Microbiol. Rev. 13(2):236-301 Morphologic structures seen in the sporangium-producing Mucorales
- 35. Branching at right angles Lactophenol cotton blue On microscopy on KOH Preparation & Sabaroud medium KOH Preparation Nonseptate hypae Growth on Sabauroud medium Courtesy to Dr Shishir Vanjare, GSMC & KEMH, Mumbai
- 36. Mucor growth culture on Agar Plate
- 37. Immunology of Mucormycosis In healthy state resting spores are resistant to phagocytic killing. So spores are susceptible to degradation by macrophages. The case of immune suppression, and ability of macrophage against Mucorales is compromised. On penetration of the endothelial lining, mucorales attack platelets. Platelets adhere to mucormycete spores, and favour germination & destruction. Dendritic cells are activated in response to Mucorales, inducing adaptive immunity.
- 38. Mucormycosis [Pathogenesis] Mucorales involve arteries causing thrombosis & infarction. Mold spread quickly along lamina properia of small and medium sized arteries and extend beyond Cr Ns into brain. Infection involve all structures in the path, orbit, eye, bone and brain. ICA thrombosed in 1/3 of autopsies. Carvenous sinus thrombosis frequent. Perineural ascending spread thr Cr Ns to Brain (Thrombosis of arteries and veins due to angioinvasiveness)
- 39. Management of Mucormycosis “Time is LIFE” Guidelines Early diagnosis of Rhinocerebral Mucormycosis Baseline MRI Head, MR Head-Orbit, Angio-Veno URGENT Diagnostic Nasal Endoscopic for biopsy Diagnosis confirmed on Biopsy, Correct Metabolic Parameters Start Inj Amphotericin B, Oral Posaconazole, Early Surgical Debridment by nasal Endoscopy & Orbital & Facial debridment. Stop Anticoagulation 12 hrs before 1st debridment, (Cont. next Page)
- 40. Most of CAM Diabetics are on Rivoroxaban OR Dabigatran on discharge If Second Debridment needed, Consider 2nd Debridment based on Clinical & Repeat Imaging Stop Rivaroxaban for 12 hours before second Debridment Restart Rivaroxaban 12 hours after Second Debridment After 15 days of Antifungal Treatment, review for continuing therapy for 1 to 2 Weeks Always monitor Carefully Neurological signs Management of Mucormycosis “Time is LIFE” Cont. from last slide
- 41. Medical Management Blood sugar control, daily monitoring of RFT, LFT, Hemogram, Electrolytes Liposomal Amphotericin B, 1.5 to 5 mg/kg/day, for 2 weels for all, watch Toxicity Dual therapy of Amphotericin B & Posaconazole, 300 mg BD, on day 1, From day 2, 300 mg once a day for all patients. Oral Posaconazole 300 mg BD, for next 2 to 4 weeks or more monitoring clinical & radiological recovery. (Tissue diagnosis is must before starting treatment)
- 42. Inj. Amphotericin B Preparations Conventional Preparations Liposomal Amphotericin B Colloid Dispersion Lipid Complex Inj Amphotericin B is to be administered by slow IV infusion Premedication : 1) 1 liter of Nacl to avoid renal toxicity Antihistaminics and Glucocorticoids to prevent Anaphylaxis Amphotericin B need dilution in Dexrous for administration & slow infusion Costly, Less Renal toxicity
- 43. Liposomal Amphopericin B Injection Broad spectrum Antifungicidal Adverse effects : Fever, Headache, Renal toxicity, Hypokalemia, hypomagnesimia Anorexia, Nausea, Vomitng, Hepatic toxicity, cardiac arrythmias, Liposomal Preparationhas Drug Interactions : Flucytosine, Cisplastin, Foscarnet, Aminoglycosides Start with low dose, gradually increase to Therapeutic levels
- 44. Liposomal Pharmacodynamics of Amphotericin B Bioavailability : 100% for intravenous infusion. Protein Binding : 90 % to plasma proteins Metabolism : Exclusively renal Half life : 15 days LD 50 : > 5 mg / kg, can result in Cardiorespiratory arrest
- 45. Tab Amphotericin B : IIT- Hyderabad Oral Amphotericin –B : 60 mg Tab Nanotechology Less Kidney toxicity Cost Rs 200 / day Great Promise
- 46. Oral Posaconazole Antifungal drug superior to Flucanozole Hepatic Toxicity : Mild to severe Absorption decreased by proton pump inhibitors Can be used as salvage treatment in those intolerant to Amphotericin B IV & Liquid formulation also available Can also used as stepdown treatment after administration of Amphotericin B Caution needed with other drugs with potent CYP450 inhibitors
- 47. Surgical Management of CAM Early surgical debridment of sinuses for all (Escharotomy) Transcutaneous retrobulbar Amphotericin B, 3.5 mg in 1 ml, in selected cases Orbital exentrationfor those with extensive orbital involment Facial surgical debridment Follow up of patient ofter discharge to check recurrence Aggressive Medical treatment & Surgical intervention
- 48. Management of Cavernous Sinus & Arterial occlusion in Mucormycosis Aggressive Treatment with Amphotericin B & Prosaconazole is the KEY Use of Anticoagulation & Antiplatelets It is better to do Early Surgical debridment to prevent stroke Mannitol can be used only if needed to reduce ICT Craniotomy with Decompressive surgery is sometimes Life Saving
- 49. Complications & Prognosis Blindness, stroke, facial disfiguration, organ damade & death Mortality is over 50 % despite prompt diagnosis & treatmen Delay in Diagnosis is culprit for higher deaths
- 50. Why Epidemic of Mucormycosis in India There are few cases of Mucormycosis in rest of the World India had no cases of of Mucormycosis in 1st Covid 19 Wave In 2nd Wave we have 3 times more cases than 1st Wave Maharashtra produce 1500 metric tons of Medical O2 per Day O2 requirement of Maharashtra in 2nd Wave jumped to 300% Suboptimal hyegine of Industrial O2, and water used in O2 therapy humidifier Suboptimal hyegine in Hospitals, due to workload beyond human capacity
- 51. Prevention of Mucormycosis Personal hygiene of body with attention to nose and oral cavity Environmental cleanliness Early diagnosis of mucormycosis by mass awareness campaign Early institution of therapy Adequate contrpl of blood sugar levels in diabetics Personal awareness in Diabetics & immunocompromised
- 52. DD of Rhinocerebral Mucormycosis Orbital Tuberculosis B-Cell Lymphoma IgG-4 related disease Orbital Sarcoid Malignancy-Meastasis Wegener’s granulomatosis Tolosa Hunt Syn Vascular Malformation of Orbit
- 53. Summary & Conclusions Rhinoorbitocerebral Mucormycosis is highly fatal disease Early diagnosis is most crucial New Symptom in Diabetic (Post-Covid) should be investigated URGENTLY. Severe Headache out of proportion to common cold in Diabeti consider Mucormycosis Early MRI Imaging of Orbits & Brain should be done ENT & Eye Consultation for New symptoms need consideration Early Diagnosis of Mucormycosis is warrante Aggressive Medical & Surgical Treatment carries good outcome.