
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie H & p format(gi)
Ähnlich wie H & p format(gi) (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
H & p format(gi)
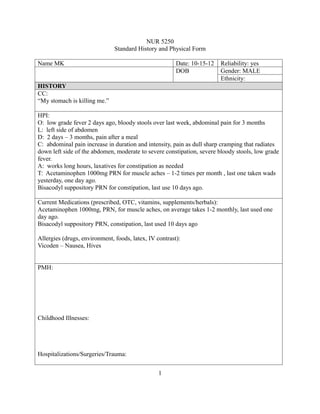
- 1. NUR 5250 Standard History and Physical Form Name MK Date: 10-15-12 Reliability: yes DOB Gender: MALE Ethnicity: HISTORY CC: “My stomach is killing me.” HPI: O: low grade fever 2 days ago, bloody stools over last week, abdominal pain for 3 months L: left side of abdomen D: 2 days – 3 months, pain after a meal C: abdominal pain increase in duration and intensity, pain as dull sharp cramping that radiates down left side of the abdomen, moderate to severe constipation, severe bloody stools, low grade fever. A: works long hours, laxatives for constipation as needed T: Acetaminophen 1000mg PRN for muscle aches – 1-2 times per month , last one taken wads yesterday, one day ago. Bisacodyl suppository PRN for constipation, last use 10 days ago. Current Medications (prescribed, OTC, vitamins, supplements/herbals): Acetaminophen 1000mg, PRN, for muscle aches, on average takes 1-2 monthly, last used one day ago. Bisacodyl suppository PRN, constipation, last used 10 days ago Allergies (drugs, environment, foods, latex, IV contrast): Vicoden – Nausea, Hives PMH: Childhood Illnesses: Hospitalizations/Surgeries/Trauma: 1
- 2. SOCIAL HISTORY Marital Status: Single Married Domestic Partner Divorced Widowed Cohabitants: ___________________________________________________________________ Children: _____________________________________________________________________ Education: ____________________________________________________________________ Occupation: ___________________________________________________________________ Interests/Activities: _____________________________________________________________ Exercise: Aerobic Weights ________________________________________________ Diet: Balanced Calcium __________________________________________________ Sleep/Rest: ______________ Caffeine: No Yes cups/day _________________________ Tobacco: No Yes PPD _______ # years _______ Quit Year _______________________ Smoking in home: Yes No __________________________________________________ ETOH: Yes No Daily Weekly Monthly # drinks ______________________ Recreational Drugs: ____________________________________________________________ Support Systems/Coping Skills: Adequate Inadequate FAMILY HISTORY Family History Unknown Father: _______________________________________________________________________ Mother: _______________________________________________________________________ Siblings: ______________________________________________________________________ MGF: ________________________________________________________________________ MGM: ________________________________________________________________________ PGF: _________________________________________________________________________ PGM: ________________________________________________________________________ Other: ________________________________________________________________________ Cultural/Religious Influences: _____________________________________________________ _____________________________________________________________________________ _ * Include genogram 2
- 3. HEALTH MAINTENANCE HISTORY Exam Last Date Results N/ Refused A Pap Test Mammogram SBE/TSE Stool guaiac Flex sig/Colonoscopy CXR ECG Dental Vision Hearing Lipid Profile FBS PSA PPD Immunizations (dates): Td MMR/titers Hep B Polio Varicella vaccine/chickenpox Influenza Pneumovax Safety: Seatbelt Use Cycling Helmet Sunscreen Occupational Smoke Detectors Housing Dom. Violence Firearms ROS: *note pertinent positive and negative findings General Cardiovascular Skin Respiratory Eyes Gastrointestinal Ears Genitourinary/Gynecological Nose/Mouth/Throat Musculoskeletal 3
- 4. Breast Neurological PHYSICAL EXAMINATION *address all significant pertinent and abnormal findings Weight Temp BP BMI Height Pulse Resp General Appearance Skin 4
- 5. HEENT Cardiovascular Respiratory Gastrointestinal Genitourinary Musculoskeletal Neurological Other ASSESSMENT AND PLAN Diagnosis: Differential Diagnoses: 5
- 6. Intervention: Follow-up: PERIODIC HEALTH SCREENING PLAN Exam Performed Scheduled N/A Refused Breast Exam Mammogram Pap Test Prostate exam Testicular exam Digital rectal with stool guaiac Flexible Sigmoidoscopy/Colonoscopy Bone Density PPD IMMUNIZATIONS Immunizations current: Yes No Vaccine Given Planned Refused Td Hepatitis B Influenza Pneumonia Other: HEALTH COUNSELING (check if discussed, describe any intervention) Smoking cessation ____________________________________________________________ Alcohol/Drug Use ____________________________________________________________ Diet/Weight _________________________________________________________________ Vitamins/Calcium ____________________________________________________________ Periodic Dental/Vision care _____________________________________________________ Exercise/Sleep _______________________________________________________________ Sun exposure ________________________________________________________________ Seatbelts/Helmets ____________________________________________________________ Stress/Family issues __________________________________________________________ Safety: Weapons/Domestic Violence _____________________________________________ BSE/TSE ___________________________________________________________________ Sexual issues/risks ____________________________________________________________ Contraception ________________________________________________________________ 6
- 7. Living Will/Power of atty/DNR __________________________________________________ LAB/STUDIES ORDERED CXR Lipids Creat/BUN HbA1C ECG CBC/diff LFTs TSH Electrolytes FBS UA/UC Other: Provider’s Signature Date Note dictated/written 7