

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie 20131013 04 林慧芬_復健與安寧緩和照護
Ähnlich wie 20131013 04 林慧芬_復健與安寧緩和照護 (20)
Mehr von Kit Leong
Mehr von Kit Leong (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
20131013 04 林慧芬_復健與安寧緩和照護
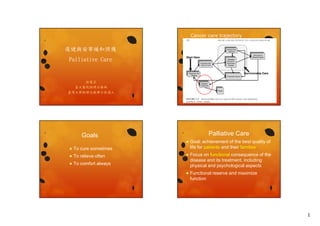
- 1. Cancer care trajectory 復健與安寧緩和照護 Palliative Care 林慧芬 臺大醫院物理治療師 臺灣大學物理治療博士候選人 Palliative Care Goals To relieve often Focus on functional consequence of the disease and its treatment, including physical and psychological aspects Functional reserve and maximize F ti l d i i function To cure sometimes Goal: achievement of the best quality of life for patients and their families To comfort always 1
- 2. How? Structure: multidisciplinary team Process: reiterative, active, educational, problem-solving process Assessment Goal setting intervention reassessment Outcome maximize the participation in patient’s social setting Minimize carers the pain and distress of patients and Where? What? Hospital Hospice/specialist palliative setting Disease related: brain tumor… Day care center Community Treatment related: chemotherapy induced, radiotherapy induced… Symptoms, etiology of the symptoms y p , gy y p 2
- 3. Symptoms Palliative care Functional limitation Pain Breathless/Dyspnea Cancer related fatigue (CRF) M t l Health: communication i ti Mental H lth 有效的溝通 依照疾病的病程與病人狀態提供以病人 為中心的決策過程 處理癌症或非癌症的併發症 症狀控制 心理社會及靈性的照護 瀕死照護(生命末期照護) 照護的協調性與持續性 Assessment 3
- 4. Deconditioning Fatigue Complications of treatment Under nutrition Neurological and musculoskeletal problems Pain Disability y Functional loss Dependent ADL Bowel and bladder dysfunction Thromboembolic disease Depression Coexisting comorbidities Poor quality of life Caregiver need Healthcare resource utilization Need for institutionalization Physical disability Cancer patients in the hospital setting 35% experienced functional loss due to physical weakness 32% required assistance with performance on ADLs 23% experienced difficulty with ambulation 7% had deficits in transfers (Lehmann et al., 1978) Significant functional impairments in patients with advanced and terminal cancer (Yoshioka Progressive debility and being a burden to others as reasons for desiring death among cancer patients (Breitbart et al., 1998; Morita et al., 2004) , ) et al., 1994) Maintain highest level of functional ability of Hospice and palliative care patients Patients’ desire Reduce burden of care Improve overall quality of life Satisfaction of care function pain care, function, and anxiety 4
- 5. Patient & Family Centered Patient & family’s expectation family s Environmental Patient What brings you the most pleasure? What are the most important things prevented? Physical ability Expected activity Questions What do you most like to do tomorrow if you can? Caregiver Red Flags or Yellow Flags Anemia Neutropenic What are you allowing the patient to do independently? Physical Functioning Complete blood count What’s the most concerned in caring for the physical What s needs of the patient? Strength, ROM, muscular and cardiopulmonary endurance, pain Thrombocytopenic Eastern Cooperative Oncology Group (ECOG) scale Neural impairments Skeletal impairments Karnofsky Performance Status scale (KPS scale) y ( ) Cardiovascular or pulmonary system 5
- 6. ECOG performance status KPS scale 0 Fully active, able to carry on all pre-disease performance without restriction 1 Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g., light house work, office work 2 Ambulatory and capable of all selfcare but unable to carry out any work activities. Up and about more than 50% of waking hours 3 Capable of only limited self care, confined to bed or chair more than 50% of waking hours 4 Completely disabled. Cannot carry on any selfcare. Totally confined to bed or chair 5 100 Normal no complaints; no evidence of disease. 90 Able to carry on normal activity; minor signs or symptoms of disease. 80 Normal activity with effort; some signs or symptoms of disease. Unable to work; able to live at home and care for most personal needs; varying amount of assistance needed. 70 Cares for self; unable to carry on normal activity or to do active work. 60 Requires occasional assistance, but is able to care for most of his personal needs. 50 Requires considerable assistance and frequent medical care. Unable to care for self; requires equivalent of institutional or hospital care; disease may be progressing rapidly. 40 Disabled; requires special care and assistance. assistance 30 Severely disabled; hospital admission is indicated although death not imminent. 20 Very sick; hospital admission necessary; active supportive treatment necessary. 10 Grade ECOG Able to carry on normal activity and to work; no special care needed. Moribund; fatal processes progressing rapidly. 0 Dead Dead Oken, et al. Am J Clin Oncol 1982;5:649-655 Patient assessment Category Physical function Karnofsky Performance Scale (KPS) Eastern Cooperative Oncology Group (ECOG) Functional Index Katz Activities of Daily Living (ADLs) Lawton Instrumental Activities of Daily Living (IADLs) Barthel Index (BI) Functional Independence Measure (FIM) Goal setting Assessment tools Balance/Fall Risk Patient and family need Achievable within one week Compensatory approach is concerned Berg Balance Scale Tinetti Assessment of Balance and Gait Timed Up and Go (TUG) Endurance 6 Minute Walk Test (6MWT) 6
- 7. 確認現有的資源及優勢-2 確認現有的資源及優勢-1 病患本身及家屬 1. 是否認清疾病進展對功能的影響? 是否認清疾病進展對功能的影響 2. 期望,是否好高騖遠? 3. 達成病患的目標需要花多少時間或 介入的次數? 4. 病患的家庭支持系統好嗎?家屬願 病患的家庭支持系統好嗎 家屬願 意配合嗎?照顧者是固定的嗎? 病患本身及家屬(續): 5 5. 病患現有的身體功能,有哪些可以安全的參與 於活動當中? 6. 病患現有的輔具有哪些?合適嗎?可以維修 或修改嗎?有輔具資源可運用嗎? 7. 病患使否有身障手冊?可爭取到哪些社會福利 資源? 8. 後續的安置問題 尊重病人自主權 確認現有的資源及優勢-3 確認現有的資源及優勢-4 照顧團隊的考量: 和病患、家屬及團隊共同擬訂計畫後一 和病患 家屬及團隊共同擬訂計畫後一 起解決問題。 1. 對於病患的期望或需要,緩和病房 團隊成員覺得可行嗎? 2. 可以給予怎樣的配合及幫助?(護理 師、社工、志工、宗教師) ★ 病患的參與可以減少其對疾病的絕望 ★ 增進和病患、家屬和醫療者間的關係 3. 3 如何以最有效率、節省人力、物力 如何以最有效率 節省人力 物力 成本的方式提供服務呢? ★ 提升病患的生活品質和減輕照顧者的 負擔 7
- 8. Palliation symptoms mobility Slowing functional decline Maintaining QOL 6-week structured PA: significant decrease in fatigue & increase in physical performance & emotional functioning (Oldervoll et al, 2005, 2006 ) 50 patients, home-based PA, walking Intervention—function Managing Improving (Lowe, et al. Support Care Cancer 2010;18:1469-75) Role of PT Strength training, ROM exercise, muscular and St th t i i i l d cardiopulmonary endurance training, pain management Activity modification Assistive devices Environmental adaptation Physical modalities for pain control Functional tasks Massage Physical modalities heat/cold Provision of adaptive and assistive equipment USD Environment modification TENS Education on energy conservation MLD Exercise Soft tissue mobilization 8
- 9. Adaptive equipment and assistive devices Caregiver education and support Adaptive equipment is used to improve performance in ADLs. ADLs Assistive devices are prescribed to help Mobility Balance Pain F ti Fatigue Joint instability Excessive skeletal loading Utilizations of strategies to prevent falls and maintain balance Weakness Use of good body mechanics Ambulation Instructions on the use of equipment Elimination of weight bearing on an affected extremity Exercise Maintenance of muscle strength, joint flexibility, range of motion, and balance Improvements in functional capacity, body composition, mood, self-esteem, quality of life Fatigue Pain Muscle spasm Edema 癌症末期療護最常見症狀 36 疼痛 70% 口乾 68% 缺乏食慾 61% 無力 47% 便秘 45% 呼吸困難 42% 噁心 嘔吐 噁心、嘔吐 36% 失眠 34% 盜汗 25% 吞嚥問題 23% 泌尿問題 21% 神經精神症狀 20% 皮膚問題 16% 消化不良 11% 腹瀉 70% 9
- 10. Case 1 Case 1 BC, bone meta with spine compression fracture BC, bone meta with spine compression fracture Intervention—pain S Somatic ti pain i Neuropathic Visceral Total Sit, dinner with family Pain, weakness, contracture of knee, poor endurance Intervention—pain (I) Medication: mouth, clock, the ladder pain pain suffering 10
- 11. Intervention—pain (2) PT Pain and Function measures Exercise and movement Graded and purposeful activity Postural re-education Massage assage Manual techniques Pain control modalities: TENS, heat & cold (Rehabilitation in cancer care, 2008) Pathophysiology of pain 11
- 12. Dyspnea Dyspnea (Rehabilitation in cancer care, 2008) Intervention—dyspnea Medical intervention Alter the physiological mechanisms Alter the central perception of dyspnea (Rehabilitation in cancer care, 2008) 12
- 13. Helpful Positions High side lying Sitting Sitti upright in a chair with f t b k and i ht i h i ith feet, back d arms supported Forward lean sitting with arms resting on pillows on a table Standing relaxed, leaning forward with arms resting on a support such as a windowsill Central Perception Fear, anxiety Fear anxiety, distress Safe, relaxation (including physical intervention) Overbreathing Communication and Understanding (empathy) Standing relaxed, leaning backwards against a wall with the legs slightly apart, chest forward and relaxed, arms hanging Fatigue: Screening & Assessment Cancer related fatigue NCCN guideline Screen and assessment patient/family education and counseling Primary evaluation Intervention non-pharmacologic pharmacologic Age 5-6 y/o: not tired, tired g y , Age 7-12 y/o: 1-5 scale 3: moderate 1-2: mild 4-5: severe Age >12 y/o: 0 10 scale 0-10 0-3: none to mild 4-6: moderate 7-10: severe 13
- 14. Patient/family education and counseling Non to Mild Not tired in age 5-6, scores 1-2 in age 7-12, 7 12 or scores 0 3 in age>12 0-3 Education Post treatment Active treatment End of life Active Post Post treatment treatment Active treatment treatment E d f lif End-of-life General strategies to manage fatigue Information about known pattern of p fatigue during and following treatment End of life General strategies for management of fatigue during active and post treatment post-treatment Energy conservation active treatment and post treatment Self-monitoring of fatigue level Energy conservation Use distraction Set priorities Pace Delegate Schedule activities at times of peak energy labor-saving devices Postpone nonessential activities P t ti l ti iti Limit naps to < 1 hour to not interfere with night-time sleep quality Structured daily routine Attend to one activity at a time 14
- 15. Non to Mild: Active Treatment Non to Mild: Post Treatment Non to Mild: End of Life Energy conservation End-of-Life Set priorities Pace Delegate Schedule activities at times of peak energy labor-saving and assistive devices Eliminate nonessential activities Structured daily routine Attend to one activity at a time Conserve energy for valued activities 15
- 16. Moderate to Severe Tired in age 5-6, scores 3-5 in age 7-12, or scores 4-10 in age>12 g Primary Evaluation Education Fatigue is not an indicator of disease progression Self-monitoring of the fatigue level Expected the end-of life symptom and the fatigue intensity may vary Primary evaluation Interventions Interventions: Active Treatment Interventions: Post Treatment 16
- 17. Interventions: End of Life Activity Enhancement (I) Fatigue: ** during cancer treatment g following cancer treatment Aerobic capacity: 11/22: significant difference between intervention and control group 3/22: significant pre-post difference 8/22: non significant difference Quality of life: - Anxiety: - Depression: - Cramp et al, 2008 Activity Enhancement (II) ↑functional capacity so↓effort in activities 15~45min/session (no more than I hour) 5 5 /sess o ( o o e t a ou ) 1-5 sessions/week 3~32 weeks, average: 12 weeks 25~80% age-predicted HRmax (220-age) walk, bicycle, ergometer, treadmill, yoga, tai-chi, walk bicycle ergometer treadmill yoga tai chi multidimensional (aerobic+stretching+resistance exercise) group/individualized, supervised/home-based , mixture of supervised and home-based Psychosocial Interventions Education: energy gy conservation and activity management to y g balance rest and activity planning, delegating, prioritizing, pacing, resting Support group Individual counseling Comprehensive coping strategy Stress management training Behavioral intervention 17
- 18. Sleep Therapy Stimulus control avoidance of long or late day naps Limiting total time in bed 注意力越來越差、皮膚顏色變化(濕冷、斑駁)、四肢 發冷末端發紺、脈搏減弱、血壓逐漸降低。 caffeine and exercise avoidance near bedtime comfortable sleep surroundings (dark, relaxing…) soothing activities at bedtime (music, …) 臨終脫水 – 不再進食及喝水。是一預備死亡的自然過程,大部分 Sleep hygiene 進行性惡化徵候 – 肌力下降 體重下降 神智混亂昏睡 時空感消失 肌力下降、體重下降、神智混亂昏睡、時空感消失、 Sleep restriction go to bed when sleepy, get out of bed after 20 min of wakefulness Have a routine bedtime and rising time 癌末頻死症狀 患者不會感到不適 患者不會感到不適。 死亡咯咯聲(death rattle) – 喉頭及支氣管內分泌物無法排出,隨呼氣及吐氣上下 移動發出聲音。 癌末頻死症狀 臨床的躁動不安 Care of palliative patient with cancer related lymphedema – 症狀包含:躁動、翻身/打滾、呻吟、意識不清、肌肉 痙攣 – 亦與下列症狀重疊:瞻妄、臨終痛苦(常因未完成遺願 而造成) 臨終大量出血 – 腫瘤在大血管周圍進而浸潤到血管壁,血管壁破裂後, 造成大量血液流出,好發於頭頸部腫瘤、骨盆腔內的 腫瘤合併陰道直腸廔管患者。 18
- 19. Possible causes of edema in palliative patients Malignant involvement or infiltration of lymphatic structure, structure lymphatic insufficiency Venous obstruction (thrombosis, compression by tumour) Decreased albumin (anorexia/cachexia of advanced cancer, ascites with repeated paracentesis) Renal or hepatic failure Cardiac failure Dependent limb, immobility, neurological deficit Effect of drug or cytotoxic chemotherapy intervention Infection 19
- 20. Key points for care of palliative patients with cancer related lymphedema Lymphedema care in advanced Thank you for you a e o a o your attention! CDT elements may need to be cancer can contribute to increasing the quality of life of the patient. Edema in this context is often multifactorial, and etiology needs to be ascertained in order to determine the appropriate treatment. The lymphedema therapist needs to work closely with the palliative team. modified, modified using lower compression and avoiding MLD directly over areas of subcutaneous tumour. Fitted compression garments are often not suitable or welltolerated in the palliative context because limb size may vary from day to day. Any Sharing? Key concepts of palliative care-1 Understanding and respect for the uniqueness of the p patient Inclusion of the family in providing care Involvement of the community in providing resources and care Interdisciplinary (team) work with nurse, physician, wound care or pain specialist, etc p p , Attention to detail and to what is important to the patient Good communication with the patient family and other palliative care providers 20
- 21. Key concepts of palliative care-2 Ingenuity and creativity in dealing with therapeutic problems Good control of pain and other symptoms Maintenance of independent and function Focus on meaning of symptoms, patient fears and expectations Non-abandonment of the patient Attention to the therapist’s own emotions in the caring for patient with limited progress 病人的疼痛應先試物理治療,一個月 沒效再開始用強效止痛劑 (X) 病人無法經由訓練提升功能時,則應 停止物理治療 (X) 病人可以選擇不接受治療 (O) Goals of care must be flexible and realistic and adapted to the patient’s ever-changing physical condition 21