Diuretics
•Als PPTX, PDF herunterladen•
0 gefällt mir•546 views

Hello friends. In this PPT I am talking about diuretics. If you like it, please do let me know in the comments section. A single word of appreciation from you will encourage me to make more of such videos. Thanks. Enjoy and welcome to the beautiful world of pharmacology where pharmacology comes to life. This video is intended for MBBS, BDS, paramedical and any person who wishes to have a basic understanding of the subject in the simplest way.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Diuretics
Ähnlich wie Diuretics (20)
Mehr von Karun Kumar
Mehr von Karun Kumar (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Diuretics
- 1. Diuretics Dr. Karun Kumar Senior Lecturer Dept. of Pharmacology
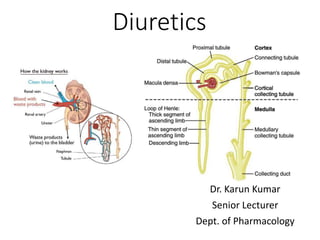
- 3. Diuretics • Diuretics (natriuretics) are drugs which cause a net loss of Na+ and water in urine • COLT Pee (Site of action) 1. Carbonic anhydrase inhibitors (PCT) 2. Osmotic diuretics (LOH) 3. Loop diuretics (TAL of LOH) 4. Thiazides (DT) 5. Potassium Sparing diuretics (CT)
- 5. Loop diuretic (Furosemide) • Its maximal natriuretic effect is much greater than that of other classes • It is active even in patients with relatively severe renal failure • The major site of action is the thick AscLH (therefore called loop diuretics) where it inhibits Na+- K+-2Cl¯ cotransport • Furosemide ↑ Ca2+ excretion (contrast thiazides which reduce it) as well as Mg2+ excretion
- 8. • Diuresis is delayed whereas release of PGs is immediate action I.v. Furosemide causes prompt ↑ in systemic venous capacitance (venodilation) due to ↑ PGs ↓ ↓ LV filling pressure (↓ preload) ↓ Shifting of fluid from pulmonary to sytemic circulation ↓ Immediate relief in dyspnoea (Quick relief in LVF and pulmonary edema)
- 9. Bumetanide • 40 times more potent than Furosemide • Induces very rapid diuresis • Highly effective in pulmonary edema. • Site of action and duration of action are similar to furosemide • Hyperuricaemia, K+ loss, glucose intolerance and ototoxicity are claimed to be less marked, but it may rarely cause myopathy
- 10. Uses 1. Edema Diuretics are used irrespective of etiology of edema—cardiac, hepatic or renal. The high ceiling diuretics are preferred in CHF for rapid mobilization of edema fluid. They are the diuretics of choice for nephrotic and other forms of resistant edema 2. Acute pulmonary edema (acute LVF, following MI) I.v. Furosemide or its congeners produces prompt relief. This is due to vasodilator action that precedes the saluretic action.
- 11. 3. Cerebral edema Though osmotic diuretics are preferred, Furosemide may be given i.m. 4. Hypertension High ceiling diuretics are indicated only in the presence of renal insufficiency, CHF, or in resistant cases and in hypertensive emergencies; otherwise thiazides are preferred
- 12. Thiazides • Medium efficacy diuretics • Site of action Cortical diluting segment or the early DT • Inhibit Na+Cl¯ symport at the luminal membrane • Moderately efficacious diuretics, because nearly 90% of the glomerular filtrate has already been reabsorbed before it reaches their site of action • Thiazides have a flat dose response curve
- 14. • The extrarenal actions of thiazides consist of a slowly developing fall in BP in hypertensives and elevation of blood sugar in some patients due to decreased insulin release which probably is a consequence of hypokalaemia
- 15. Indications 1. Edema Thiazides may be used for mild-to moderate cases • For mobilization of edema fluid more efficacious diuretics are preferred, but thiazides may be considered for maintenance therapy • They act best in cardiac edema; are less effective in hepatic or renal edema • They are powerless in the presence of renal failure • Cirrhotics often develop refractoriness to thiazides due to development of secondary hyperaldosteronism
- 16. 2. Hypertension Thiazides and related diuretics, especially Chlorthalidone are one of the 1st line drugs 3. Diabetes insipidus Thiazides decrease positive free water clearance and are the only drugs effective in nephrogenic diabetes insipidus • However, they reduce urine volume in pituitary origin cases as well
- 18. Adverse Effects 1. Hypokalaemia This is the most significant problem. • It is rare at low doses, but may be of grave consequence when brisk diuresis is induced or on prolonged therapy. • The usual manifestations are weakness, fatigue, muscle cramps.
- 19. • Cardiac arrhythmias are the serious complications. • It can be prevented and treated by: (a) High dietary K+ intake or (b) Supplements of KCl (24–72 mEq/day) or (c) Concurrent use of K+ sparing diuretics. 2. Acute saline depletion Overenthusiastic use of diuretics, particularly high ceiling ones, may cause dehydration and marked fall in BP
- 20. 3. Dilutional hyponatraemia • Occurs in CHF patients when vigorous diuresis is induced with high ceiling agents, rarely with thiazides. • Kidney tends to retain water, though it is unable to retain salt due to the diuretic; e.c.f. gets diluted, hyponatraemia occurs and edema persists despite natriuresis.
- 21. • Patients feel very thirsty. • Treatment of this distortion of fluid-electrolyte balance is difficult: 1. Withhold diuretics 2. Restrict water intake 3. Give glucocorticoid which enhances excretion of water load. 4. If hypokalaemia is present, its correction helps
- 22. 4. GIT and CNS disturbances Nausea, vomiting and diarrhoea may occur with any diuretic. • Headache, giddiness, weakness, paresthesias, impotence are occasional complaints 5. Hearing loss Occurs rarely, only with high ceiling diuretics 6. Allergic manifestations Rashes, photosensitivity occur, especially in patients hypersensitive to sulfonamides.
- 23. 7. Brisk diuresis induced in cirrhotics may precipitate mental disturbances and hepatic coma 8. Hyperuricaemia Long-term use of higher dose thiazides in hypertension has caused rise in blood urate level but is rare now due to use of lower doses
- 24. 9. Hyperglycaemia and hyperlipidemia Have occurred in the use of diuretics as antihypertensive. These metabolic changes are minimal with low dose thiazides now recommended. 10. Magnesium depletion It may develop after prolonged use of thiazides as well as loop diuretics
- 25. Interactions 1. Thiazides and high ceiling diuretics potentiate all other antihypertensives 2. Hypokalaemia induced by these diuretics enhances digitalis toxicity 3. Loop diuretics can enhance ototoxicity and nephrotoxicity of aminoglycoside 4. Indomethacin and other NSAIDs diminish the action of diuretics by inhibiting PG synthesis in the kidney
- 26. 5. Probenecid competitively inhibits tubular secretion of furosemide and thiazides: decreases their action 6. Serum lithium level rises due to enhanced reabsorption of Li+ in PT
- 27. Carbonic Anhydrase Inhibitors • In the proximal tubule, carbonic anhydrase catalyzes the reversible conversion of hydrogen ion and bicarbonate to carbon dioxide and water, thereby enabling the reabsorption of sodium bicarbonate • This process is inhibited by carbonic anhydrase inhibitors such as acetazolamide
- 29. Uses (GAME) 1. Glaucoma Adjuvant to other ocular hypotensives 2. To alkalinise urine for urinary tract infection or to promote excretion of certain acidic drugs 3. Acute Mountain sickness Symptomatic relief as well as prophylaxis. Benefit occurs probably due to reduced CSF formation and lowering of brain pH 4. Epilepsy (catamenial)
- 30. Adverse Effects • Acidosis, hypokalaemia, drowsiness, paresthesias, fatigue, abdominal discomfort • Hypersensitivity reactions—fever, rashes • Bone marrow depression is rare but serious • Contraindicated in liver disease may precipitate hepatic coma by interfering with urinary elimination of NH3 (due to alkaline urine)
- 31. Potassium sparing diuretics • Aldosterone antagonists and renal epithelial Na+ channel inhibitors indirectly conserve K+ while inducing mild natriuresis potassium sparing diuretics • In the collecting duct, sodium enters the principal cells through sodium channels • Sodium is then transferred into the interstitial fluid by the sodium pump, while potassium is pumped in the opposite direction and then moves through potassium channels into the tubular fluid
- 32. • Aldosterone stimulates these processes by increasing the synthesis of messenger RNA that encodes for sodium channel and sodium pump proteins • The potassium-sparing diuretics exert their effects via two mechanisms: 1. Amiloride and Triamterene inhibit the entrance of sodium into the principal cells 2. Spironolactone blocks the mineralocorticoid receptor and thereby inhibits sodium reabsorption and potassium secretion
- 34. Uses of Spironolactone 1. To counteract K+ loss due to thiazide and loop diuretics 2. Edema Useful in cirrhotic and nephrotic edema in which aldosterone levels are generally high • Spironolactone is frequently added to a thiazide/loop diuretic in the treatment of ascites due to cirrhosis of liver
- 35. 3. Hypertension: Used as adjuvant to thiazide to prevent hypokalemia, it may slightly add to their antihypertensive action • More importantly, it may have the potential to attenuate hypertension related renal fibrosis and ventricular/vascular hypertrophy 4. CHF As additional drug to conventional therapy in moderate to severe CHF; can retard disease progression and lower mortality
- 36. Interactions 1. Given together with K+ supplements— dangerous hyperkalaemia can occur 2. Aspirin blocks Spironolactone action by inhibiting tubular secretion of its active metabolite canrenone 3. More pronounced hyperkalaemia can occur in patients receiving ACE inhibitors/ARBs 4. Spironolactone increases plasma digoxin concentration
- 37. Adverse effects • Side effects Drowsiness, mental confusion, epigastric distress and loose motions • Spironolactone interacts with progestin and androgen receptors as well • In addition, it may enhance testosterone clearance or its peripheral conversion to estradiol, producing dose and duration of treatment related hormonal side effects like gynaecomastia, erectile dysfunction or loss of libido in men, and breast tenderness or menstrual irregularities in women • Most serious is hyperkalaemia that may occur, especially if renal function is inadequate
- 38. Eplerenone • It is a newer and more selective aldosterone antagonist which has much lower affinity for other steroidal receptors • Less likely to produce hormonal disturbances like gynaecomastia, impotence, menstrual irregularities, etc. • This feature makes it particularly suitable for longterm use in the therapy of hypertension and chronic CHF • Risk of hyperkalaemia and g.i. side effects are like spironolactone
- 39. Osmotic diuretics (Mannitol) • Acts on Loop of Henle • Mannitol appears to limit tubular water and electrolyte reabsorption by 1. Retains water isoosmotically in PT—dilutes luminal fluid which opposes NaCl reabsorption 2. Inhibits transport processes in the thick AscLH by an unknown mechanism Largest contributor to the diuresis
- 40. 3. Expands extracellular fluid volume (because it does not enter cells, Mannitol draws water from the intracellular compartment)—increases g.f.r. and inhibits renin release.
- 41. Uses 1. Increased intracranial or intraocular tension (acute congestive glaucoma, head injury, stroke, etc.): by osmotic action it encourages movement of water from brain parenchyma, CSF and aqueous humour. It is also used before and after ocular/brain surgery to prevent acute rise in intraocular/intracranial pressure 2. To maintain GFR and urine flow in impending acute renal failure e.g. in shock, severe trauma, cardiac surgery, haemolytic reactions
Hinweis der Redaktion
- Osmolarity is affected by changes in water content, as well as temperature and pressure. In contrast, osmolality is independent of temperature and pressure. 2[Na+] + [Glucose]/18 + [ BUN ]/2.8[7] where [Glucose] and [BUN] are measured in mg/dL. 285-295 milli-osmoles per kilogram. 1 mole nacl = 23 + 35 = 58gm The clearance of a drug is the theoretical volume of plasma from which the drug is completely removed in unit time. CL = Rate of elimination/C
- Thiazide diuretics have a paradoxical effect in diabetes insipidus (↓ free water clearance). Inh. PDE enz. & ↑ 3,5-cAMP ↑ memb. Perm. Of CD & DT ↓ ECF vol. & hyponatremia Stim. Na & H2O reabs. From PT ↓ delivery to DT ↓ urine o. ADH inc. memb. Permeab. Of CT by inc. 3,5-cAMP
- Dilutional hyponatremia, also known as water intoxication, it is a potentially life-threatening condition which occurs when a person consumes too much water without an adequate intake of electrolytes.
- Paresthesia (or paraesthesia) is an abnormal dermal sensation (e.g., a tingling, pricking, chilling, burning, or numb sensation on the skin) with no apparent physical cause. The manifestation of a paresthesia may be transient or chronic, and may have any of dozens of possible underlying causes.
- Catamenial epilepsy is a gender-specific type of epilepsy in which seizure frequency intensifies during certain phases of the menstrual cycle.