Autonomic nervous system-I
•Als PPTX, PDF herunterladen•
0 gefällt mir•127 views

The autonomic nervous system (ANS) carries nerve impulses from the central nervous system to effector organs via two types of neurons - preganglionic and postganglionic. Preganglionic neurons originate in the CNS and synapse in peripheral ganglia, while postganglionic neurons innervate effector organs. Acetylcholine is the main neurotransmitter of the parasympathetic division and some parts of the sympathetic division. It is synthesized locally and broken down by acetylcholinesterase. Cholinergic drugs like pilocarpine and edrophonium act by either directly activating cholinergic receptors or indirectly by inhibiting acetylcholinesterase. Atropine is a competitive mus

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Autonomic nervous system-I
Ähnlich wie Autonomic nervous system-I (20)
Mehr von Karun Kumar
Mehr von Karun Kumar (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Autonomic nervous system-I
- 1. Autonomic Nervous System Dr. Karun Kumar Assistant Professor Dept. of Pharmacology
- 6. Working of ANS • Efferent neurons The ANS carries nerve impulses from the CNS to the effector organs by way of two types of efferent neurons: the preganglionic neurons and the postganglionic neurons • The cell body of the first nerve cell, the preganglionic neuron, is located within the CNS
- 8. • The preganglionic neurons emerge from the brainstem or spinal cord and make a synaptic connection in ganglia (an aggregation of nerve cell bodies located in the peripheral nervous system) • The ganglia function as relay stations between the preganglionic neuron and the second nerve cell, the postganglionic neuron • The cell body of the postganglionic neuron terminates on effector organs, such as smooth muscles of the viscera, cardiac muscle, and the exocrine glands
- 10. Cholinergic transmission • Acetylcholine Neurotransmitter at 1. Neuromuscular junction (NMJ) 2. All preganglionic neurons 3. All postganglionic parasympathetic neurons 4. Postganglionic sympathetic neurons in sweat glands
- 12. Synthesis, storage and destruction of ACh • Synthesized locally in the cholinergic nerve endings
- 13. Cholinesterase • 2 types:- 1. Acetylcholinesterase—AChE or true cholinesterase 2. Butyrylcholinesterase—BuChE or pseudochE
- 14. Location of cholinergic receptors 1. M1 Autonomic ganglia, gastric glands, CNS 2. M2 Heart (SA node, AV node, atrium) 3. M3 Visceral smooth muscle, ciliary muscle, Exocrine glands, vascular endothelium 4. NM Neuromuscular junction 5. NN Autonomic ganglia, adrenal medulla
- 15. Pehle khao (M1)phir dil lagao (M2) baaki kaam baad mein (M3)
- 23. Cholinergic agonists 1. Direct acting agonists Bind & activate Ach rec. a) Choline esters Ach, Bethanechol, Carbachol b) Plant alkaloids Muscarine, Nicotine, Pilocarpine, Arecoline 2. Indirectly acting agonists (anti-chE) a) Reversible Carbamates, Non-carbamates b) Irreversible Carbamates, Organophosphates
- 25. Pilocarpine • Obtained from the leaves of Pilocarpus microphyllus and other species • Prominent muscarinic action (M3) & mild nicotinic action at ganglia (NN) • Applied to the eye, it penetrates cornea and promptly causes miosis, ciliary muscle contraction and fall in intraocular tension lasting 4–8 hours. • Uses Open angle glaucoma, xerostomia • S/E Initial stinging sensation in the eye and painful spasm of accommodation, marked sweating, salivation and ↑ in other secretions
- 26. Edrophonium • Resembles Neostigmine in action • Has a brief duration of action (10–30 min) • Diagnostic agent for myasthenia gravis • Dose: 2–10 mg i.v.
- 27. Myasthenic vs Cholinergic crisis • Myasthenic crisis Ach ↓↓ • Cholinergic crisis Ach ↑↑ • Edroph. (Rev. inhib. of AchE) ↑ Ach at NMJ ↓ ↓ Dramatic improvement Worsened condition (Myasthenic crisis) (Cholinergic crisis) • Short duration of action (desirable for pts. presenting with cholinergic crisis as the worsening in their condition would be for short lasting)
- 28. Uses of anti-cholinesterases 1. Glaucoma 2. To reverse the effect of mydriatic After refraction error testing 3. To prevent and break adhesions between iris and lens/cornea Miotic is altered with mydriatic 4. Myasthenia gravis Neostigmine is used 5. Postoperative decurarization To reverse effect of muscle relaxants 6. Postoperative paralytic ileus/urinary retention
- 29. Why neostigmine is used in myasthenia gravis ?
- 31. 7. Cobra bite To antagonize the curare-like action of cobra neurotoxin 8. Belladonna poisoning Physostigmine is drug of choice for atropine poisoning 9. Alzheimer’s disease Rivastigmine, Donepezil and Galantamine afford some symptomatic improvement
- 32. Signs and symptoms of OP poisoning (Muscarinic) M Miosis U Urination S Secretions↑ (Salivation, lacrimation & sweating) C Cardiac contraction & conduction slows A Abdominal cramps R Reduction in i.o.t. (esp. in glaucoma) I Increased GI motility N NO (Nitric oxide) dependent vasodilatation I Inc. sec. from GIT & tracheobronchial tract C Constriction of tracheobronchial tract
- 33. Toxic manifestations • Nicotinic Fasciculations of skeletal muscles leading to paralysis 1. Monday = Mydriasis 2. Tuesday = Tachycardia 3. Wednesday = Weakness 4. Thursday = Hypertension 5. Friday = Fasciculations
- 34. Toxic manifestations • CNS 1. Restlessness 2. Tremors 3. Convulsions 4. Ataxia 5. Respiratory arrest
- 35. Treatment 1. Termination of further exposure to the poison— fresh air, wash the skin and mucous membranes with soap and water, gastric lavage according to need 2. Maintain patent airway, positive pressure respiration if it is failing 3. Supportive measures—maintain BP, hydration, control of convulsions with judicious use of diazepam
- 36. Specific antidotes 1. Atropine All cases of anti-ChE (carbamate or organophosphate) poisoning must be promptly given atropine 2 mg i.v. repeated every 10 min till dryness of mouth or other signs of atropinization appear (upto 200 mg has been administered in a day). Continued treatment with maintenance doses may be required for 1–2 weeks 2. Cholinesterase reactivators Pralidoxime is injected i.v. slowly in a dose of 1–2 g (children 20–40 mg/kg) [Only in OP poisoning]
- 38. Atropine Uses (ATROPA) 1. As mydriatic-cycloplegic in refraction error testing, fundoscopy, iridocyclitis 2. Traveller’s diarrhea 3. Rapid onset mushroom poisoning 4. Organophosphorus poisoning 5. Preanaesthetic medication 6. Arrhythmias (brady-arrhythmias)
- 39. Adverse effects of Atropine (DHATURA) 1. Dry mouth, difficulty in swallowing & speaking 2. Hot dry skin & hypotension 3. Accommodation paralysis (blurring of near vision) 4. Tachycardia 5. Urinary Retention & fecal retention (constipation) 6. Ataxia & acute congestive glaucoma may precipitate • “Dry as a bone, blind as a bat, red as a beet, and mad as a hatter”
- 41. Dental implication of atropine • Xerostomia caused by atropinic drugs can promote dental caries and oral candidiasis
- 43. Treatment of atropine poisoning 1. If poison has been ingested, gastric lavage should be done with tannic acid 2. Patient should be kept in a dark quiet room 3. Cold sponging or ice bags are applied to reduce body temperature 4. Physostigmine 1–3 mg s.c. or i.v. antagonises both central and peripheral effects 5. Other general measures (maintenance of blood volume, assisted respiration, diazepam to control convulsions) should be taken as appropriate
- 45. Contraindications of atropine 1. Individuals with a narrow iridocorneal angle— may precipitate acute congestive glaucoma 2. Caution is advocated in elderly males with prostatic hypertrophy—urinary retention can occur
- 46. Interactions 1. Absorption of most drugs is slowed because atropine delays gastric emptying. Extent of digoxin and tetracycline absorption may be increased 2. Antihistaminics, tricyclic antidepressants, phenothiazines, disopyramide, pethidine have anticholinergic property—additive side effects occur with atropinic drugs
- 47. Uses of other anti-cholinergics 1. To relieve urinary frequency and urgency, enuresis in children (Vasicoselective) 2. Bronchial asthma and COPD Ipratropium bromide and Tiotropium bromide 3. Parkinsonism Central anticholinergics reduce tremor and rigidity 4. Motion sickness Hyoscine (severe case), Dicyclomine (mild cases)
Hinweis der Redaktion
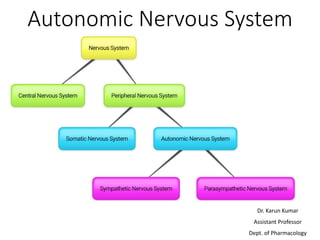
- involuntary ; A ganglion is a group of neuron cell bodies in the peripheral nervous system. In the somatic nervous system this includes dorsal root ganglia and trigeminal ganglia among a few others. In the autonomic nervous system there are both sympathetic and parasympathetic ganglia which contain the cell bodies of postganglionic sympathetic and parasympathetic neurons respectively.
- The efferent neurons carry signals away from the brain and spinal cord to the peripheral tissues, and the afferent neurons bring information from the periphery to the CNS. A ganglion is a collection of neuronal bodies found in the voluntary and autonomic branches of the peripheral nervous system (PNS). Ganglia can be thought of as synaptic relay stations between neurons. The information enters the ganglia, excites the neuron in the ganglia and then exits.
- "ganglion" should be reserved for collections of nerve cell bodies outside the central nervous system and nuclei should be used for collections of neurons inside.
- While AChE is strategically located at all cholinergic sites and serves to inactivate ACh instantaneously, BuChE present in plasma and elsewhere probably serves to metabolize ingested esters.
- Edrophonium is a short and rapid-acting anticholinesterase drug. Its effect is manifest within 30 to 60 seconds after injection and lasts an average of 10 minutes.
- Deficiency of Ach in M. crisis
- Paralytic ileus is the condition where the motor activity of the bowel is impaired, usually without the presence of a physical obstruction.
- Why neostigmine & not physostigmine in myasthenia gravis ? m. Gravis A.b. against Nm rec.; 1. Neost. Has acn. On periph. Tissues without causing a/e in CNS;2. direct agonistic action on Nm rec. in addn. to inh. Of chE 3. Physost. Produces undesirable central effects. It lacks the direct agonistic action on nicotinic cholinergic receptors
- Ptosis /ˈtoʊsɪs/ is a drooping or falling of the upper eyelid.
- Cobra venom consists of a neurotoxin which is responsible for respiratory paralysis simulating that associated with a non-depolarizing muscle relaxant
- a brief spontaneous contraction affecting a small number of muscle fibres, often causing a flicker of movement under the skin
- A fasciculation, or muscle twitch, is a spontaneous, involuntary muscle contraction and relaxation, involving fine muscle fibers
- The high affiity of pralidoxime for phosphorus enables it to break the phosphorus bond with cholinesterase and thereby regenerate the enzyme
- Pralidoxime is ineffective as an antidote to carbamate anti-ChEs (physostigmine, neostigmine, carbaryl, propoxur) in which case the anionic site of the enzyme is not free to provide attachment to it.
- Cycloplegia is paralysis of the ciliary muscle of the eye, resulting in a loss of accommodation
- Inhaled mercury vapours while making hats
- Delirium an acutely disturbed state of mind characterized by restlessness, illusions, and incoherence, occurring in intoxication, fever, and other disorders.
- Why Physostigmine is preferred over Neostigmine in Atropine Poisoning ? P is tert. Amine (lipid soluble) & crosses BBB. Neost. Cannot cross BBB due to its polar nature & therefore, not able to reverse the central sympt. Of atr. poisoning