
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Penetrating neck trauma [autosaved]
Ähnlich wie Penetrating neck trauma [autosaved] (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Penetrating neck trauma [autosaved]
- 1. PENETRATING NECK TRAUMA PRESENTED BY DR. KARIM
- 2. Introduction i. Penetrating Trauma from clavicles to skull base (neck) . ii. PNT is a relatively uncommon inj with significant morbidity and possible mortality . iii. There is no international guidelines on PNT management. iv. Surgical management for PNT has evolved the last two decades , based on the advent of advanced radiographic studies and endoscopic techniques. v. Management of PNT is a big challenging issue for emergency physicians , due to two reasons location of vital structures and critical inj and vascular management . vi. Anatomy of the Neck region is very necessary .
- 3. Epidemiology 1.7 % all trauma patients have PNT Male 4 * Female GSW about 24-48 % Cause of inj Stab wound about 40 – 75 % cause of inj GSW is responsible for 50 % significant inj and often critical inj Stab inj responsible for 10-20% significant inj and less critical inj All PNT have 1,3 – 3 % mortality Major vascular inj have 50 % mortality Wounded age average 30 y Zone II inj = about 38- 67 % Zone III inj = about 16-19% Zone I inj 13-18%
- 4. Epidemiology Approximately 10 % of patients present with air way compromise. Isolated Cervical spin inj in PNT are uncommon. 7% of wounded have cervical spin inj . Unstable cervical spin inj are rare < 0,5 % Arterial inj about 25 % of all PNT Carotid artery is 80 % involve & Vertebral artery is 43% involve of 25% arterial inj Aero digestive structures inj occurs about 23-30% of all PNT Neurologic structures inj occurs about 20 %
- 5. Surgical anatomy of neck Skin Fascial Layer of the neck Platysma muscle ( Ext Jugular vein is located superficial …)
- 6. Fascial layer of the neck Fascia is the internal connective tissue forms sheets. Support internal structures of the neck . Compartmentalizes structures of the neck . Superficial cervical layer or fascia & deep cervical fascia
- 7. Deep Cervical Fascia Lies deep to the superficial fascia and platysma muscle . Acts like a shirt collar , supporting the structures and vessels of the neck . Organized into several layers . 1. Investing layer , lies superficial , can be thought like a tube. 2. pretracheal layer , situated in the ant neck , fuses with pericardium, trachea , esophagus , thyroid gland , infra hyoid muscle enclosed by it . 3. Prevertebral fascia , surrounds vertebral column , its associated muscles , surrounds the brachial plexus as it leaves the neck and subclavian artery as it pass through the lower neck region (forms axillary sheath. 4. Carotid sheath (enclosed Common carotid artery , Int jugular vein and vagus nerve .
- 10. Carotid sheath and triangle
- 11. Neck triangles Anterior trisngle Posterior triangle Carotid triangle
- 12. Anterior triangle Its contents : Common carotid artery & its bifurcation Internal jugular vein Cranial nerve = VII , IX , X , XI , XII
- 13. Posterior triangle It’s contents : subclavian vein + artery Transvers cervical vein +artery Supra scapular vein + artery Cranial nerve XI Accessory N Brachial plexus Cervical plexus (Phrenic N)
- 14. Carotid triangle It’s contents : common carotid artery Internal jugular vein Vagus N
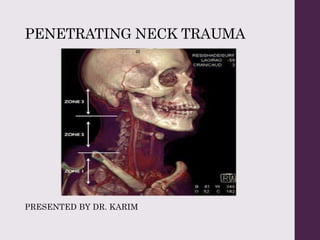
- 15. Neck Zones
- 16. Zone I o Most caudal anatomic zone o Structure within this zone include the : 1. Proximal common carotid artery . 2. Vertebral and subclavian arteries . 3. Subclavian , innominate , and jugular vein . 4. Recurrent laryngeal N & Vagus N 5. Esophagus 6. Thoracic duct Vascular inj Mangement is challenging in this zone . High mortality Due to the sternum , surgical access to zone I may require sternotomy or thoracotomy to control hemorrhage . Needle thoracostomy . check the upper limbs .
- 17. Zone II 1. Middle anatomic zone 2. Vertical & horizontally neck exploration incision provide surgical access to this zone . It’s contains : carotid artery jugular and vertebral vein , pharynx , & larynx Recurrent laryngeal & Vagus N spinal cord
- 18. Zone III 1. The cephald anatomic zone 2. Vascular access in this zone is difficult, some time require craniotomy , mandibulotomy or maneuvers to displace anteriorly the mandible . 3. Anatomic structures in this zone are : Extra cranial carotid & vertebral artery Jugular vein spinal cord cranial nerve IX , XII sympathetic trunk
- 19. Type of inj (pathophysiology) Etiology divided : 1- high velocity mechanism -- cause critical inj , make temporary cavity & permanently cavity inside the wound 2- low velocity mechanism ---just make permanently cavity inside the wounds , and injure the neck structures on the projectile victor . 3 – vascular structures injured by both , direct & indirect trauma (temporary cavity & shear force ) primary & secondary after the time of injury .
- 20. Primary and secondery vascular pathology Primary vascular inj : vessel es transection vessel es laceration vessel es puncture vessel es intimal flap pseudo aneurysm Secondary vascular inj : thrombosis , arterovenus fistula formation , pseudo aneurysm .
- 21. Clinical Feature میباشد ذیل های حالت دو از انتروال یکی به عنق نافذه تروما مجروحین. 1-اعراض بدون نسبی طور به و ثابت هیمودینامیک حالت به 2-شاک درحالت مریضان–هوایی طرق تشوش و خونریزی
- 22. Aero digestive & vascular Hard & soft sign Hard sign Soft sign Air way compromise Stable hematoma Massive subcutaneous emphysema Mild hypotension Air bubbling through the wound Un explained altered mental status Expanding or pulsatile hematoma Focal neurologic deficit Active bleeding Prehospital bleeding from inj shock نزدیکشریان موقیعت به جرحه بودن داخلی جگوالر ورید و کاروتید Neurologic deficit Subtle neurologic deficit
- 23. Hard sign Soft sign Stridor Audible bruit and palpable thrill inside the inj dyspnea Absent or diminished peripheral pulse Shock Deep neck pain Pain or difficulty when swallowing Hematemesis Change of Voice Odynophagia Laryngeal crepituse Dysphagia hemoptysis Cervical or mediastina air –x ray hoarseness
- 24. Decision for management in PNT patient
- 27. Prehospital Management Patient with PNT can decompensate rapidly & should be transported immediately to a trauma center . Impaled object should not be removed in the field . Systemic approach to the management of PNT is critical . The initial evaluation and assessment involves resuscitation in accordance with the ATLS principles .
- 28. Air way Management Airway obstruction Secretion or blood in respiratory tract Fracture or inj of larynx Massive sub cutaneous emphysema Trachea deviation Expanding hematoma Altered mental status Soft tissue distortion Changes of voice Stridor Hemoptysis
- 29. Air way management I. Orotrachail intubation II. intermittent suction III. Tracheotomy and tracheostomy IV. Cricothyroidotomy V. Supra glottis air way VI. Up right position VII. Trachial tube placement through the wound of trachea VIII. Avoid and do not use bag valve mask
- 30. شود گرفته نظر در هوایی طرق منجمنت جریان در باید که نقاط. 1-کی جروحاتو نافذه په عنق د چه دا -خوری برهم له اناتومی نارمل–وی موجود هیماتوم–جریان خونریزی فعاله لری–وی مختل شعور–وی موجوده حنجری د یا تراکیا د جرحه–وینه یا افرازات وی موجوده کی لیاره هوایی. چی ده مشکله زیاته لپاره داکتر تجربه با زیات د حتی کی حاالتو پورتنی په شی وکوالی منجمنت هوایی طرق–تجربه اندازه کافی باید اساس همدی په ولرو وسایل کافی ورسره او مهارت او. 2-طرق شی کیدای چه دا بل وی نه نارمله کی جروحاتو دی په اناتومی چه دا ولری جرحه خپله هوایی–د هم یا او انتوبیشن کاذب د انتوبیشن کورانه کور شی کیدای مخامخ سره خطر زیات ال د جرحه حنجری یا تراخیا–زیات نو دی کار په احتیاط. 3-د وینی د انتوبیشن کی شتون په هیماتوم د عنق د واوسو متوجه باید ته دی شی کیدای سبب خونریزی دوباره او کیدو خطا د علقی. 4-هوایی د وجه په افرازاتو داخلی او خونریزی داخلی د انتوبیشن تر وروسته دی ممکن بندش لیاری–شته ضرورت ته سکشن ییی قفه و لپاره دهمدی.
- 31. Breathing Pneumothorax Hemothorax Mediastina hematoma Usually in Zone I PNT can cause of respiratory Failure : Needle decompression is necessary sometime شود گرفته نظر در رابطه در باید که نقاط. 1 -زدن سوزن جهت درست موقیعت انتخاب 2-بزرگتر گیج با سوزن داشتن 3–بی و اسان زدن سوزن صدر جنب ناحیه در صدر نازک جدار داشتن به نسبت بود خواهد خطر.
- 32. Vascular management Bleeding should stop in Prehospital care : 1- Direct pressure 2 – Dressing with paraffin gauze which prevent air embolisms particularly when vien is involve . 3- Use folly catheter , it is most useful technique . انتقال د نباید او دی نه ضروری کی وخت دی په رسی الس ورته یا نیول ورید کو ضایع ورباندی وخت.وکوو کار دا لیاره پر کی وخت په انتقال د شی کیدای. ( prolong on scene time ) ( Scoop and run )
- 33. Cervical spine immobilization spine immobilization is controversial because : 1- incidence the cervical spines inj in PNT are rare 2 – Most of cervical spine inj are stable 3- It’s waste the time of transport about (2.5- 5 ) min کو تعقیب او ارزیابی توگه مستقیم په جرحه عنق د کوالی نشو. کوی مداخله کی کنترول او کی منجمنت په لیار هوایی د. کوی وروسته تشخیص. کوالی نشو ارزیابی هیماتوم د عنق د. شته استثنا یو–کو تثبیت فقرات باید وی موجود تشوشات نیورولوژیک چیری که. کی ضابع وخت انتقال د مجروح د نباید تثبت فقراتو رقبی د باالخره.
- 34. Emergency Department management 1-Follow the ATLS principles) A,B,C,D,E,) 2-باشد حیات کننده تهدید حاالت با توجه. 3–نمایید اجرا ضروری های کمک تروما تیم اعضا همه باید همزماه. 4–میگردد دوباره خونریزی باعث گردد تفتش عاجل اطاق در نباید جرحه. 5-باشد هوایی طرق کنترول و خونریزی کنترول در تمرکز باید ها کمک اجرا در. 6–باشد داشته خاص ضیعت و باید مریض هوایی امبولی از جلوگیری جهت. 7-شود گرفته مقابل طرف در باید مایعات تطبیق جهت ورید. 8-نگردد تطبیق است بهتر مری جروحات تشخیص تا انفی تیوب. 9-طرق باید ان از قبل باشد داشته نیاز عاجل جراحی به مریض که صورت در گردد کنترول کتیتر فولی یا مستقیم فشار توسط فعال خونریزی و کنترول هوایی. 10–در ولی است کم عنق جروحات در مرکزی موقیعت نسبت مری جروحات زیاد جروحات مس بنا ندارد تشخیصیه و بارز عالیم باشد داشته جرحه که صورت سیپس و منصف التهاب باعث از دارد درقبال زیاد میر مرگ که دارد...
- 35. speech stridor shortness of breath Bubbling wound Subsutaneus Empysema Surgical Crepitus Haemoptysis Pneumothorax Bleeding (مستقیم فشار توسط خونریزی توقف ) Hematoma (Expanding or pulsatile) Bruits Carotid inj ( Hornor syndrom) Unilateral absent radial pulse Arterial - brachial index(<90) Pain on Swallowing Heamatemesis Cranial nerve Hornors Syndrom Recurrent laryngeal Nerve Brachial plexus Phrenic Nerve Long Tract sign Air way Vascular Oesophageal Neurological ) Clinical assessment ( گردد معاینه روتین شکل به باید ذیل عالیم
- 36. Diagnostic imaging Direct laryngoscopy Video laryngoscopy Fiber optic laryngoscopy Bronchoscopy Oesophagoscopy Angiography CT
- 37. Surgeons Trauma surgeon Neurosurgeon vascular surgeon General surgeon ENT surgeon Anesthesia Experts
- 51. References 1- ATLS 2- Chapter 7 penetrating & blunt neck trauma Nathan L.Salinas, MD, captain,MC, USA Joseph A, BrennamMD, Colonel, MC,USAF 3-Penetrating neck traum (Royal college of surgeons) 4-WTA (critical decisionin in trauma: penetrating neck trauma) 5- RELIAS MEDIA penetrating neck trauma 6-VENTURA COUNTY MEDICLA CENTER TRAUM DEPARTMENT 7-REBELEM 2018 8- Teach me anatomy