These presentation is related to biliary disorders. it is simple and concise presentation and provide all information about the biliary disease. i hope this presentation fulfill your requirements and should be useful.
Premium Call Girls In Jaipur {8445551418} ❤️VVIP SEEMA Call Girl in Jaipur Ra...
Biliary disorders
1. PRACTICE TEACHING
BILIARY DISORDERS
SUMITTED TO: SUMITTED BY:
MRS. HIMANTA S. MAGANJI MR.KAPIL SHARMA
HOD MEDICAL SURGICAL NURSING M.Sc. NSG 1st YEAR
SAIMS COLLEGE OF NURSING SAIMS COLLEGE OF NSG
2. INTRODUCTION OF BILIARY DISORDERS
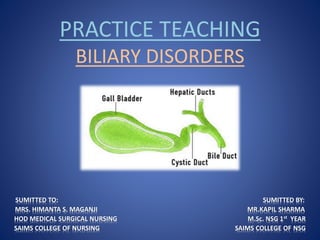
• The gallbladder and bile ducts comprise the Biliary
system and any abnormality (stones formation,
inflammation, etc) in these organs are called biliary
disorder.
• Disorders of the Biliary tract are common and
include gallbladder stones and interfere with the
normal drainage of bile into the duodenum.
3. DEFINATION OF BILIARY DISORDERS
Biliary disease is any pathology affecting the
gallbladder and its conduits; commonly
cholecystitis, cholelithiasis, cholesterolosis, etc
Any abnormality (stones formation, inflammation,
etc) of or relating to bile, to the ducts that convey
bile, or to the gall bladder.
8. DEFINITION OF CHOLECYSTITIS
• Cholecystitis is an inflammation of the gallbladder
wall and nearby abdominal lining. Cholecystitis is
usually caused by a gallstone in the cystic duct, the
duct that connects the gallbladder to the hepatic
duct.
9. TYPES OF CHOLECYSTITIS
• Acute cholecystitis, an acute inflammation of the
gallbladder, is most commonly caused by gallstone
obstruction.
• Acalculous cholecystitis is acute gallbladder
inflammation without obstruction by gallstones.
• Chronic cholecystitis occurs when the gallbladder
becomes thickened, rigid, and fibrotic and functions
poorly. Results from repeated attacks of
cholecystitis.
10.
11. ETIOLOGICAL FACTORS OF CHOLECYSTITS
• Secondary bacterial infection
• Bacteria:
o Escherichia coli
o Klebsiella species
o Streptococcus
• Major surgical procedures
• Severe trauma
• Burns
• Cystic duct obstruction
• Bile stasis & increased viscosity of the bile
• Gallbladder stones
13. CLINICAL MANIFESTATIONS OF
CHOLECYSTITIS
• Acute cholecystitis-
Biliary colic pain that persists more than 4 hours
and increases with movement, including
respirations.
Nausea and vomiting
Low grade fever
Jaundice.
Right upper quadrant guarding
Murphy’s sign (inability to take a deep inspiration
when examiner’s finger are pressed below the
hepatic margin)
17. MANAGEMENT OF CHOLECYSTITS
• Supportive management-
IV fluids
Nasogastric suction
Pain management
Antibiotics
• A cholecystostomy tube may be placed
percuteniously into the gallbladder to decompress
the organ in preparation for future surgery.
18. MANAGEMENT OF CHOLECYSTITS
Cont..
• Surgical management-
Cholecystectomy
Intraoperative cholengiography
Choledochoscopy for common bile duct exploration.
Placement of a T- tube in the common bile duct to
decompress the biliary tree postoperatively.
Direct contact therapy by which a local cholelitholytic
agent is infused by a catheter directly into the
gallbladder or through a percutaneous transhepatic
biliary catheter.
20. DEFINITION OF CHOLELITHIASIS
• Gallstones form when bile stored in the gallbladder
hardens into stone-like material. Too much
cholesterol, bile salts, or bilirubin (bile pigment) can
cause gallstones. When gallstones are present in the
gallbladder itself, it is called cholelithiasis.
21. DEFINITION OF CHOLEDOCHOLITHIASIS
• When gallstones are present in the bile ducts, it is
called choledocholithiasis.
o There are two types of gallstones:
Cholesterol stones (80%)
Pigment stones (20%)
o The size of gallstones varies from a grain of salt to
golf-ball size.
o A person can develop a single stone or several
hundred.
22. ETIOLOGICAL FACTORS OF CHOLELITHIASIS
& CHOLEDOCHOLITHIASIS
• Stones occur when cholesterol supersaturates the
bile in the gallbladder and precipitates out of the
bile. The cholesterol saturated bile predisposes to
the formation of gallstones and acts as an irritant,
producing inflammatory changes in the gallbladder.
• Pigment stones occur when free bilirubin combines
with calcium.
• Use of oral contraceptives and estrogens.
23. ETIOLOGICAL FACTORS OF CHOLELITHIASIS
& CHOLEDOCHOLITHIASIS
Cont..
• Stone formation increases with the age because of
increased hepatic secretion of cholesterol and
decreased bile acid synthesis.
• Some disease conditions like
• Cirrhosis
• Hemolysis
• Infection
25. CLINICAL MANIFESTATIONS OF
CHOLELITHIASIS &CHOLEDOCHOLITHIASIS
• Asymptomatic
• Biliary colic (steady, severe, aching pain or sensation of
pressure in epigastrium or right upper quadrant, which
may radiate to the right scapular area or right shoulder)
• Gallstone continue to obstruct the duct, abcess, necrosis
and perforation with generalized peritonitis may occur.
• Jaundice
• Changes in the urine and stool color
• Vitamin deficiency due to obstruction of the bile flow
interferes with absorption of the fat soluble vitamin A, D,
E, K.
28. MANAGEMENT OF CHOLELITHIASIS &
CHOLEDOCHOLITHIASIS
• Supportive management-
IV fluids
Nasogastric suction
Pain management
Antibiotics
Dietary management may be the major mode of
supportive management in patient who have had
only dietary intolerance to fatty foods and vague GI
system.
29. MANAGEMENT OF CHOLELITHIASIS &
CHOLEDOCHOLITHIASIS
Cont..
• Pharmacologic therapy-
Ursodeoxycholic acid (UDCA) and chenodeoxycholic
acid (chenodilol) have been used to dissolve small,
radiolucent gallstones composed primarily of
cholesterol by inhibiting the synthesis and
secretions of cholesterol.
30. MANAGEMENT OF CHOLELITHIASIS &
CHOLEDOCHOLITHIASIS
Cont..
• Non surgical removal of gallstones-
a. Dissolving Gallstones- gallstones dissolve by a
infusion of a solvent (mono octanoin or methyl
tertiary butyl ether [MTBE]) into the gallbladder.
31. MANAGEMENT OF CHOLELITHIASIS &
CHOLEDOCHOLITHIASIS
Cont..
b. Stone Removal by Instrumentation-
A catheter and instrument with a basket attached
are threaded through the T- tube tract or fistula
formed at the time of T-tube insertion; the basket is
used to retrieve and remove the stones lodged in
the common bile duct.
Secondly ERCP used to cut the submucosal fibers or
papilla of the sphincter of oddi, enlarging the
opening, which may allow the lodged stones to pass
spontaneously into the duodenum.
32. MANAGEMENT OF CHOLELITHIASIS &
CHOLEDOCHOLITHIASIS
Cont..
c. Intracorporeal lithotriopsy- stones in the
gallbladder or common bile duct may be
fragmented by means of laser pulse technology. The
laser pulse produces rapid expansion and
disintegration of plasma on the stone surface
resulting in a mechanical shock wave. This results in
pressure waves that cause stones to fragment.
33. MANAGEMENT OF CHOLELITHIASIS &
CHOLEDOCHOLITHIASIS
Cont..
• Surgical management-
o Laproscopic Cholecystectomy
o Cholecystectomy
o Choledochotomy
o Cholecystostomy
34. COMPLICATIONS OF CHOLELITHIASIS &
CHOLEDOCHOLITHIASIS
• Cholengitis
• Necrosis, empyema or perforation of gallbladder.
• Biliary fistula through the duodenum
• Gallstone ileus
• Adenocarcinoma of the gallbladder
• Bile peritonitis
35. NURSING MANAGEMENT OF
CHOLELITHIASIS & CHOLEDOCHOLITHIASIS
a) Preoperative Nursing Management:
Discuss with the patient to give full information about
the surgery
Allow the patient to ask question and clear all his
doubts
Explain what happens during anesthesia.
Obtain the consent from the patients / guardian for
each operation after explaining the nature of the
operation and anesthesia.
Assist the doctor to carry out a through physical
examination, assess the physical health of the patient.
36.
37. NURSING MANAGEMENT OF
CHOLELITHIASIS & CHOLEDOCHOLITHIASIS
Conti..
Ask the patient appropriate questions to obtain
past and present medical history in order to exclude
anaemia, jaundice , drug reaction , previous
operation etc.
Part preparation is done according to the surgery.
Administer the pre – medications to the patient one
hour before surgery. These are the drugs that
reduce anxiety of patient .
38. NURSING MANAGEMENT OF
CHOLELITHIASIS & CHOLEDOCHOLITHIASIS
Cont..
Before giving the Pre – medications. Check the vital
signs of the patient such as blood pressure,
temperature, pulse, respiration etc. Record the vital
signs in the patient chart as baseline data.
Provided the psychological support to the patient
and his family member.
Prepare the articles before surgical procedure.
39. NURSING MANAGEMENT OF
CHOLELITHIASIS & CHOLEDOCHOLITHIASIS
Cont..
b) Postoperative Nursing Management:
Preparation of post anesthetic bed and reception
the patient.
Assess any complication of surgery.
To prevent hypoxia, continue pulse oximetry after
surgery until an acceptable oxygen saturation level.
Maintain intact dressing of the site of the surgical
wound.
40. NURSING MANAGEMENT OF
CHOLELITHIASIS & CHOLEDOCHOLITHIASIS
Conti..
Assess pulse for rate rhythm and amplitude, weak,
absent or irregular pulse may reflect hypovolemia,
decreased cardiac output. A bounding pulse
indicate hypertension, fluid overload or excitement.
Assess level of consciousness by observing how the
person responds to verbal commands and touch,
pupil reaction to light and reflexes should be
observed.
Continuously check the drain for any abnormal
secretions or bile.
41. NURSING DIAGNOSIS OF CHOLELITHIASIS
& CHOLEDOCHOLITHIASIS
i. Acute pain and discomfort related to biliary colic
or stone obstruction, surgical incision.
ii. Impaired gas exchange related to the high
abdominal surgical incision.
iii. Deficient fluid volume related to nausea &
vomiting and decreased intake.
42. NURSING DIAGNOSIS OF CHOLELITHIASIS
& CHOLEDOCHOLITHIASIS
iv. Impaired skin integrity related to altered Biliary
drainage after surgical intervention.
v. Imbalance nutrition, less than body requirement,
related to inadequate bile secretion.
vi. Deficit knowledge about self care activities related
to incision care dietary modification.