2. z
Definition
Orthognathic surgery is
the art and science of
diagnosis, treatment
planning, and execution
of treatment by
combining orthodontics
and oral and
maxillofacial surgery to
correct musculoskeletal,
dento- osseous, and soft
tissue deformities of the
jaws and associated
structures
3. The history of orthognathic surgery of the mandible started with
Hullihen in 1846, who performed an osteotomy of the mandibular body
for the correction of prognathism.
Simon. P. Hullihen
HISTORY
4. z
• In 1849, Henry Blair developed
osteotomy of mandibular body
for the correction of mandibular
horizontal excess.
Henry Blair
5. The 1920s and 1930s
saw further
modifications by
Limberg, Wassmund,
and Kazanjian of
external approaches to
ramal osteotomies. All
of these had difficulties
with relapse.
The earliest description
of what would become
the modern BSSO and
the first intraoral
approach to a ramal
osteotomy was
described in the
German literature by
Schuchardt in 1942.
In 1954, Caldwell and
Letterman described a
vertical ramus
osteotomy technique,
which was shown to
preserve the inferior
alveolar neurovascular
bundle
13. z
• Medial and forward displacement of the mandibular
disk- by the upper head of the lateral pterygoid
muscle.
• After sectioning - the mandibular condyle is displaced
in the same direction as the disk - by the pull of the
lower head of the lateral pterygoid muscle.
14. z
Muscles
Contribution of suprahyoid muscles in relapse in mandibular
advancement
Ellis and Carlson study (in monkeys) – relieving the suprahyoid
muscles from the symphysis of the mandible decreased the
amount of relapse
Clinical studies – have failed to show a relation between
suprahyoid myotomies and relapse.
17. z
Determination of safe distance away from the apex of
teeth:
• The safer distance is 5 mm but studies have shown that
even 10 mm distance shows pulpal changes.
• Epker BN. Vascular considerations in orthognathic surgery: I. Mandibular osteotomies. Oral surgery, oral medicine, oral
pathology. 1984 May 1;57(5):467-72.
19. z
• The medial horizontal cut be at or just above the tip of the lingula because
a higher cut may be associated with an increased difficulty in splitting or
incidence of unfavorable fracture
7.5 to 13.3 mm above lingula
Buccal & lingual cortex fusion occurs at a rate of
:
• 20% in the anterior ramus
• 39% in the posterior ramus
22. z
Classification of the
topography of the
inferior alveolar nerve.
J Anat 1971;108:433-40
• I = the nerve has a
course near the apices of
the teeth,
• II = the main trunk is
low down in the body
• III = the main trunk is
low down in the body of
the mandible with several
smaller trunks to the
molar teeth
23. z
Revasculirasatio
n and healing
• Intermedullary circulation between the proximal and distal segments
• Margins of osteotomy- avascular
Immediate post-operatively
• Level of hypervascularity around surgical site
• No soft tissue re-attachment
• Isolated areas of sub- periosteal bone formation
One week post-op
• Avascular zone at the proximal osteotomy site
• Necrotic zone at the distal osteotomy site
• No soft tissue attachment at distal necrotic zone
2weeks post-op
• Soft tissue re-attachment
• Vascular anastamoses between proximal and distal segments
• Osteoid formation through out marrow formation
3 weeks post-op
• Circulation reconstituted across the osteotomy site
• Soft tissue re- attachment established
6 weeks post-op
• Circulation between the segments is continuous
12 weeks post- op
25. z
Timing of surgery
As a rule of thumb it is better to wait till the skeletal growth is
completed before doing orthognathic surgery.
Corrective surgical measure even during the growth period, specially if
there is compelling psychological need for such intervention in the
patient.
28
26. z
Role of pre-surgical orthodontics
To eliminate dental mal-relationships
which
prevent surgical repositioning of
fragments
To achieve decompensation by undoing
the natural compensating tooth
alignments.
To create interdental spacing to facilitate
segmental osteotomy and
To perform those tooth movements
which, if done post-surgically, will spoil the
result of surgery.
29
29. z
Evolution of BSSO
The focus of innovation in mandibular surgery migrated to
Europe where Trauner and Obwegeser in 1957 described
what would become today's BSSO.
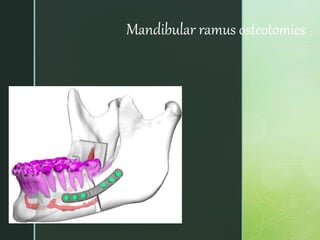
35. z
BILATERAL SAGITTAL SPLIT RAMUS
OSTEOTOMY
BSSO is similar for all 3 clinical situations , with subtle variations in the
osteotomy and fixation techniques.
INDICATIONS:
Horizontal
mandibular
excess
Horizontal
mandibular
deficiency
Asymmetry
Mandibular
advancement
Mandibular
setback(small-
moderate)
52. z
• 19. Stripping the medial pterygoid msucle and
stylomandibular ligament.
20. Removal of impacted third molars.
21. Smoothing contact areas of bone segments.
22. Placement of a holding wire.
23. Noting the position of IANB
24. Noting position of 3rd molar.
53. z
• 19. Stripping the medial pterygoid msucle and
stylomandibular ligament.
20. Removal of impacted third molars.
21. Smoothing contact areas of bone segments.
22. Placement of a holding wire.
23. Noting the position of IANB
24. Noting position of 3rd molar.
54. z
25. Mobilization of distal segment.
26. Selective odontoplasty and maxilla-mandibular fixation.
59. z
32. Removing MMF ad checking occlusion.
33. Intraop diagnosis of malocclusion.
34. Placement of intraoral and extraoral
sutures.
35. Placement of elastics.
36. Placement of a pressure bandage.
60. z
• With wire at upper and lower border
• Lag screws
• Bicortical screws – 2 or 3 screws are used
• Mini plates
• Bioresorbable plates and screws
Fujioka M, Fujii T,Hirano A. Comparative study of mandibular stability after sagittal split osteotomies:
bicortical versus monocortical osteosynthesis. Cleft palate craniofacial journal 2000; 37:551.
Fixation techniques
61. To define the separation better, a thick, finely
tapered osteotome-10mm wide is driven
between the proximal & distal segments of the
mandible through an anterior corticotomy.It
should not reach IAN
The Dunn dautrey osteotome is driven gently
with only manual force, b/w the buccal cortex &
medulla. The buccal & lingual cortices are
separated with only little resistance as a result
of the complete burring of the post.margin of
the medial osteotomy & inferior margin of
vertical osteotomy
Dunn dautrey osteotome is run carefully down
the inferior border of the mandible.
All contents of IAN is separated from the buccal
attachments , nerve & vessels should be
allowed to fall medial to the osteotome. The
Dunn dautrey osteotome is manually twisted
under visualization of IAN
MANUAL TWIST TECHNIQUE
62. The osteotome should be twisted in the
direction that the distal portion of the
proximal segment is opened & the distal
tips of both proximal segments are
rotated to the buccal side.
This prevents manual twisting force from
being transferred to the TMJ.
Twisting starts from anterior portion of
proximal segments just behind the
vertical buccal osteotome. Splitting by
manual twist force extends from the
mandibular angle to the post. Border of
ascending ramus.
63. z
Vertical ramus
osteotomy
• 1st described by Caldwell and
Letterman in 1954- extra oral
Indications:
Patient with horizontal mand excess.
Mandibular asymmetry.
Contraindications:
Advancement of distal tooth bearing
segment.
Recent condylar #
72. z
COMPARISON BETWEEN SSRO
ANDVRO
McKenna SJ, King EE. Intraoral Vertical Ramus Osteotomy Procedure and Technique. Atlas of the oral and
maxillofacial surgery clinics of North America. 2016 Mar 1;24(1):37-43.
SSRO VRO
OSTEOTOMY PASaggital split Latero medial cut
Open procedure Blind procedure
Along IAN Rear to IAN
Frequent exposure of IAN No exposure of IAN
BONE HEALING Contact on marrow to
marrow
Contact on cortex to
cortex
BONE FIXATION Rigid internal fixation No fixation
CONDYLAR HEAD Original position New equilibrated
position
POST OP IMF
prognosis
None or shorter period
Weakly dependent on pt
Required 7-10 day
Strongly dependent on pt
73. z
REFERENCES
Fonseca- Maxillofacial Surgery Vol. 2
Reyneke Essentials of Orthognathic Surgery Second Edition.
Peterson- Principles of Maxillofacial Surgery.
AOMSI textbook
Bell W, Schendel S: Biological basis for the saggital ramus
split operation J Oral Surg 1977;35;362
Epker BN: Modifications in the saggital split osteotomy of the
mandible. J Oral Surg 1977;35;157.