Tracheostomy,Parathyroid and Pituitary
•
2 gefällt mir•706 views

Dr.Dinesh.M.G Professor of Surgery J.J.M.M.C Davangere

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Tracheostomy,Parathyroid and Pituitary
Ähnlich wie Tracheostomy,Parathyroid and Pituitary (20)
Mehr von J.J.M.Medical College,Davangere
Mehr von J.J.M.Medical College,Davangere (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Tracheostomy,Parathyroid and Pituitary
- 1. Dr. Dinesh. M.G Professor of Surgery J.J.M.M.C. Davangere
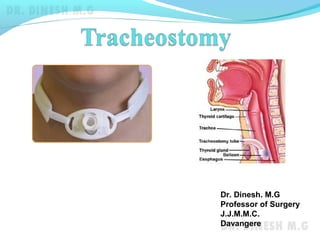
- 2. Tracheostomy A tracheostomy is a surgically created opening (stoma) through the front of neck into the windpipe (trachea). A tube is usually placed through this opening to provide an airway and to remove secretions from the lungs. This tube is called a tracheostomy tube Endotracheal tubeTracheostomy tube
- 3. Tracheostomy Indications 1.Upper airway obstruction Foreign body Infection(Diphtheria, Ludwig’s angina) Oedema of glottis(head and neck burns) Bilateral vocal cord palsy Trauma(faciomaxillary, larynx, trachea) Tumour(carcinoma larynx) Congenital lesions(web, atresia) Chronic stenosis(TB)
- 4. Tracheostomy Indications (cont’d) 2.Retained secretions Severe bronchopneumonia Chronic bronchitis Chest injury(flail chest) 2.Respiratory insufficiency Head injury Bulbar poliomyelitis Barbiturate poisoning Tetanus
- 5. Tracheostomy Objectives of tracheostomy To assist respiration Relief from airway obstruction Reduction of the anatomical dead space(150ml) Access for tracheobronchial toileting Cuffed tube prevents aspiration and allows positive pressure ventilation All these objectives can be met by endotracheal intubation initially. But the need for prolonged endotracheal intubation requires tracheostomy
- 7. Tracheostomy Steps of operation of emergency tracheostomy 1.Patient in supine position with neck extended 2.After local anaesthesia, 1.5” vertical skin incision is given below cricoid in the midline 3.Skin, platysma,deep fascia and pretracheal fascia are divided 4.Isthmus of thyroid is divided between ligatures 5.Cricoid hook is used to lift & stabilise trachea 6.The 2nd , 3rd & 4th tracheal rings are divided with a knife 7.Tracheal wound is dilated with tracheal dilator 8.Tracheostomy tube is inserted and cuff inflated 9.The tube is fixed around neck with tapes
- 8. Tracheostomy
- 9. Tracheostomy Elective tracheostomy Transverse skin incision is placed Inverted U shaped tracheal flap is raised and stitched to skin incision Aftercare of tracheostomy Humidification Intermittent suction of tracheobronchial secretions Clearance of thick mucus by nebulisation and washing of inner tube with sodabicarb and changing Care of cuff with low pressure Replacement of tube once in 3-4 days correctly
- 10. Tracheostomy Complications of tracheostomy Intraoperative Haemorrhage Recurrent laryngeal nerve injury Injury to oesophagus Postoperative Surgical emphysema Pneumothorax Pneumomediastinum Wound infection Aspiration pneumonia Tracheal stenosis Tracheoesophageal fistula Tracheo-innominate artery fistula
- 12. Parathyroid glands Surgical anatomy Four(2pairs) small, oval, yellowish brown glands located on the posterior surface of thyroid gland Superior parathyroids develop with the thyroid gland from the 4th branchial arch and are constant in position Inferior parathyroids develop with thymus from 3rd branchial arch descending lower along with thymus and are variable in position
- 13. Parathyroid glands Physiology Chief cells of parathyroid produce parathormone(PTH) PTH raises plasma calcium levels by Increasing calcium absorption from intestine Releasing calcium from bones by osteoclastic stimulation Increasing the renal resorption of calcium Calcitonin secreted by parafollicular cells of thyroid has opposite action on calcium i.e. it lowers the serum calcium levels.
- 14. Hypoparathyroidism Usually due to damage to parathyroid gland during thyroidectomy Due to decreased PTH hypocalcemia develops leading to tetany. Clinical features Circumoral tingling and numbness Chvostek’s sign Trousseau’s sign Carpopedal smasm Laryngeal stridor
- 16. Hypoparathyroidism-Tetany Diagnosis Serum calcium levels below normal(9-11mg%) Treatment 10 ml of intravenous calcium gluconate slowly in acute cases Oral calcium with Vit-D3 in permanent hypoparathyroidism
- 17. Hyperparathyroidism Increased secretion of PTH leading to hypercalcemia and its clinical manifestations Types Primary hyperparathyroidism Adenoma (solitary) Hyperplasia Carcinoma Secondary hyperparathyroidism Decreased calcium levels in CRF & Vit-D deficiency Tertiary hyperparathyroidism Prolonged stimulation by hypocalcemia
- 18. Hyperparathyroidism Clinical features Asymptomatic- detected by biochemical screening Symptomatic cases Renal stones Diseases of bones Bone pains Pathological fractures Cysts and pseudotumours of bones Osteoporosis and subperiosteal erosions in skull and phalanges Psychic moans Abdominal groans Peptic ulcers Pancreatitis
- 19. Hyperparathyroidism Diagnosis Biochemical investigations Raised calcium and PTH levels Decreased serum phosphorus levels Raised serum alkaline phosphatase levels Radiological investigations X-ray skull and phalanges Usg neck CT and MRI Thallium-Technetium subtraction isotope scan Selective angiography and venous sampling
- 20. Hyperparathyroidism Treatment Surgical removal of overactive glands Adenoma-Excision Hyperplasia –Excision of all 4 parathyroids and autotransplantation of one parathyroid in forearm muscles Carcinoma – radical excision along with thyroid
- 21. Thank you