Osteoradionecrosis
•Als PPTX, PDF herunterladen•
91 gefällt mir•26,768 views

Osteoradionecrosis

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Osteoradionecrosis
Ähnlich wie Osteoradionecrosis (20)
Mehr von Mohammed Haneef Farooq
Mehr von Mohammed Haneef Farooq (15)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Osteoradionecrosis
- 2. Introduction Most serious complication of radiation therapy for cancer Probably the first evidence of ORN related to radiotherapy was reported by Regaud in 1922 Its pathology was further described by Ewing in 1926, under the name ‘radiation osteitis’ Meyer classified ORN as one special type of osteomyelitis. Titterington also related ORN to osteomyelitis, providing one of its first definitions, and used the term ‘osteomyelitis of irradiated bone’ Marx defined it as ‘an area greater than 1 cm of exposed bone in a field of irradiation that had failed to show any evidence of healing for at least 6 months’. He also clarified that in ORN there is no intersticial infection, but only superficial contamination
- 3. 1. The affected site should have been previously irradiated; 2. There should be absence of recurrent tumour on the affected site; 3. Mucosal breakdown or failure to heal should occur, resulting in bone exposure (except in cases of bones that lie within thick soft tissue integument’s, such as the pelvis or femur, or rarely in cases of a pathological fracture of the mandible after irradiation); 4. The overlying bone should be ‘dead’, usually due to a hypoxic necrosis; 5. Cellulitis, fistulation, or pathologic fracture need not be present to be considered ORN
- 4. Classification of bone exposures Bone exposure resulting from tumor necrosis where tumor death results in a loss of soft tissue coverage. bone exposure at the site of tumor during or within a week of radiotherapy Bone exposure as a consequence of tumor recurrence. In all cases surgical resection was undertaken –tumor recurrence Bone exposure resultant from oral surgical or dental interventions. Extractions sites. Persistent bone necrosis due to denture irritation Bone exposure de novo. no obvious source of trauma
- 5. DEFINITION An exposure of irradiated bone which fails to heal with out intervention (Marx 1983) It is a chronic nonhealing wound caused by hypoxia, hypocellularity, and hypovascularity of irradiated tissue. Marx and Johnson (1987) Clinical definition by Van Merkesteyn (1995) Bone and soft tissue necrosis of 6 months duration excluding radiation induced periodontal breakdown
- 6. INCIDENCE Before 1960 orthovoltage -ORN ranging from 17%-37% megavoltage therapy is bone sparing. Incidence ranges from upto 10%. By Reuther et al the incidence was found to be 8.2% in population of 830 individuals investigated for over a period of 30 years Mandible is affected more commonly; because most oral tumors are peri mandibular. More extensive blood supply in maxilla
- 7. Int J Oral Maxillofac Surg. 2003 Jun;32(3):289-95 Osteoradionecrosis of the jaws as a side effect of radiotherapy of head and neck tumor patients--a report of a thirty year retrospective review Reuther T, Schuster T, Mende U, Kubler A.
- 8. Retrospective 830 pts Incidence 8.2% 3 fold higher in Men Body of mandible Extraction -50% Presurgical earlier ORN Combined radio and chemo
- 9. Bedwinek et.al T3 AND T4 lesions - more prone higher tissue destruction, larger treatment volume. No necrosis if 50- 60Gy used Low dosing brachytherapy higher ORN, secondary to decay profile of a combination of mix of alpha, beta and gamma particle spin off.
- 10. Etiology Radiation in excess of 50Gy- kills bone cells – osteoblasts & fibroblasts leading to hypocellularity Vessels -tunica intima endarteritis, periarteritis hyalinization and fibrosis Progressive obliterative arteritis.— hypovascularity Periosteal vessels and inferior alveolar artery involved Hypoxia
- 11. angiogenesis and stem cell mitogenisis -platelet derived growth factors third day -under macrophage Migrate - excess of 20 mm of Hg. Radiation shallow oxygen gradient macrophage chemotaxis angiogenic and fibroblast growth factors 3-H TISSUE wound healing
- 12. Radiation beam field effect greater -central beam tapers off -outward resemble a target center -most affected Healing -reduced or absent
- 13. Precipitating factors Triad Concept challenged by Gowgiel. Approximately one third of ORN occur spontaneously. RADIATION TRAUMA INFECTION
- 14. Modern concept - Marx biochemical and cellular pathology ORN is radiation induced, nonhealing hypoxic wound rather than true osteomyelitis or irradiated bone
- 15. Microbiology Cultures streptococci, Candida spp., and gram negative organisms. When skin is affected S. aureus and S.epidermidis. No organisms are found deep in bone. Radiation predisposes to actinomycotic infection; because is favorable environment for microorganism to flourish due to bone tissue alteration
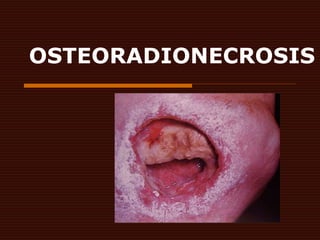
- 16. CLINICAL FEATURES Within two years Asymptomatic dehiscence of mucosa Glabrous skin As necrosis progresses site more erythematous and severe, deep burning pain Evidence of exposed bone
- 19. Tissue surrounding may be ulcerated from infection or recurrent tumor. Trismus Fetid breath Elevated temperature Exposed bone with a grey to yellow color Intraoral and extra oral fistula Pathological fracture
- 20. Radiographic changes Little-evident sequestra or involucra occur late radiolucent modeling -nonsclerotic Nuclear isotope technetium 99 methylene diphosphonate Bony algorithm high resolution CT
- 22. Histologically look like MICROANATOMIC DESERT Reduced vascularity, fibrosis
- 23. Diagnosis of osteoradionecrosis should focus primarily on ruling out recurrent or metastatic disease. Therefore is diagnosis of exclusion
- 24. MANAGEMENT
- 25. Protocol for preirradiation oral evaluation Osteoradionecrosis of jaws Marciani RD, Ownby H E J Oral Maxillofac Surg 44; 218-223; 1986
- 26. Post irradiation care Dentures should not be used for one year Good oral hygiene maintenance Fluoride therapy Saliva substitute to prevent dry mouth Pulpitis- endodontic therapy Atraumatic extractions –no flap or linear closure Local anesthetic without adrenaline should be used Antibiotic should be administered
- 27. Management of osteoradionecrosis Aim - To control frank infection Antibiotics Penicllin plus metronidazole or clindamycin Supportive therapy with fluids Pulsating irrigation device can be used. High pressure should not be used debris might be forced deeply into tissues Exposed bone can be mechanically debrided and smoothed with round burs and covered with a pack saturated with zinc peroxide and neomycin
- 28. Conservative management of osteoradionecrosis J K Wong, R E Wood, Mc Lean Triple O 1997; 84:16-21
- 29. local irrigation (saline solution, NaHCO3, or chlorhexidine), systemic antibiotics in acute infectious episodes, avoidance or irritants and oral hygiene instruction. Simple management refers to the gentle removal of sequestra in sequestrating lesions Had 48% success rates
- 30. Treatment of small areas with drilling multiple holes into vital bone is recommended by Hahn and Cargill (1967) to encourage sequestration. Daland (1949) advised electro coagulation of exposed bone to expedite sequestration and drainage of subcutaneous abscesses to prevent sloughing of skin.
- 31. Treatment of osteonecrotic wounds Rule out neoplastic disease Stabilize the patient medically especially nutritional status Preoperative hyperbaric oxygen Debridement of necrotic mass Postoperative hyperbaric oxygen Soft tissue vascular flap support Bony reconstruction
- 32. Ultra sound therapy Is non invasive and reportedly promotes neovascularity and neocellularity of ischemic tissues
- 33. Major healing of refractory mandible osteoradionecrosis after treatment combining pentoxifylline and tocopherol: a phase II trial. Head Neck. 2005 Feb;27(2):114-23. Delanian S, Depondt J, Lefaix JL
- 34. Effective in reversing fibronecrotic process Eighteen patients a daily oral combination of 800 mg of PTX and 1000 IU of vitamin E for 6 to 24 months In addition, the last eight patients who were the worst cases were given 1600 mg/day clodronate 5 days at 6 months, with 84% healing
- 36. DEFINITION Short term -100% oxygen inhalation therapy at a pressure greater than that of sea level. The pressure is usually about 2.4 absolute atmospheres or ATA.
- 37. Greenwood and Gilchrist (1973) were the first to report beneficial effects of HBO on wound healing in post RT. 1975 – Mainous and Hart – 14 cases of refractory ORN of mandible treated with HBO and hemimandibulectomy 1981 Mansfield reported complete healing with HBO 1993 McKenzie reported resolution of ORN following HBO in 69% patients
- 38. USES Decompression sickness Elective surgery to prevent clinical radiation necrosis Treatment of osteoradionecrosis Non healing diabetic ulcers
- 39. Mechanism Partial reversal of 3-H tissue physical mechanism dissolution of oxygen into blood 80-100 mm Hg range to 1000-1200 mm Hg HBO elevates the PAO2 irrespective of hemoglobin O2 gradients -radiated tissue from 50 to 250 mm Hg-macrophage activity
- 40. Angiogenic and fibroblastic effects- collagen synthesis crucially depends on the availability of molecular O2 that incorporates into a peptide chain to form hydroxyl propyl and hydroxyl lysyl residues.
- 41. HBO inhibits inflammation through direct bactericidal effects on anaerobes due to increased production of free radical and toxic products HBO enhances phagocytic killing by WBC (Parl 1994)
- 42. Stage I 30 x (100% O2 for 90 mins at 2.4 ATA) Examine exposed bone No surgery cutaneous fistula No antibiotics Rinsing only pathologic fracture resorption of Inferior border of mandible Response no response 10x (100% O2 for 90 mins at 2.4 ATA) Stage I responder Stage II Stage III
- 43. Stage II Surgery maintain inferior border 10x (100% O2 for 90 mins at 2.4 ATA) Response no response Stage II responder Healing with out exposed bone stage III Excision of nonviable bone Fixation of mandibular segments 10x (100% O2 for 90 mins at 2.4 ATA) Reconstruction after three monthsNo HBO Required
- 44. Protocol of hyperbaric oxygen for elective surgery. 20 sessions of hyperbaric oxygen prior to elective surgery, followed by 10 sessions after surgery 100% oxygen at 2.4 atmospheric pressure or ATA for 90 treatment minutes single person chambers 120 treatment minutes
- 45. The elective surgery protocol is used in all elective surgery in radiated tissue, which may range from tooth extraction, to bone graft reconstruction to vascularized pedicled and free anatomic transfers effects of hyperbaric oxygen are permanent,
- 46. Absolute contraindication Optic neuritis – exacerbation of retinal inflammation and hyperemia Immunosuppressive disorders- reports of viral encephalitis
- 47. Relative contraindication Chronic obstructive pulmonary disease Bullous lung change and significant CO2 retention Claustrophobia. Acute respiratory infections Surgery induced Eustachian tube dysfunction
- 48. Hyper baric oxygen in therapeutic management of osteoradionecrosis of facial bones S Vudiniabola, P J Williamson, A N Goss Int J Oral Maxillofac Surg 2000; 29:435-438
- 49. Have reviewed 17 cases of facial bone osteoradionecrosis treated according to Marx protocol plus or minus surgery Dental extraction was the cause in 9 cases. Three cases of temporal bone ORN were of spontaneous onset. All were stage I responded well to HBO
- 50. FREE OMENTAL TRANSFER FOR ORN OF MANDIBLE Int J Oral Maxillofac Surg 2000 :29:201-206 K.Wataru, K Makoto et.al
- 51. Omentum is an intra abdominal organ rich in vascular and lymphatic plexus. McLEAN &BUNCKE first to use greater omentum Moran and Panje use it for ORN of mandible. 4 cases treated with same no recurrence
- 52. Advantages The natural mandibular contour and continuity can be preserved Can be used regardless of size of defect No need for bone grafting Short procedure compared to osteocutaneous flaps
- 53. CONCLUSION ORN is best defined as a slow healing radiation induced ischemic necrosis of bone with associated soft tissue necrosis of variable extent occurring in absence of local primary, tumor necrosis, recurrence or metastatic disease that may or may not
- 54. Be super infected And companied by fistulation End in pathologic fracture Resolve with out surgery HBO or both
- 55. THANK YOU