Call Girls Tirupati Just Call 8250077686 Top Class Call Girl Service Available
Clinical Work Up Of A Patient With Lymph adenopathy
1. CLINICAL WORK UP OF A PATIENT WITH LYM
Dr.Anil Haripriya
The lymph nodes are major components of the lymphatic system placed in small
drain the lymphatic vessels of various anatomic regions. They are composed of dense
node is ovoid, round or bean shaped and vary in size from 2 mm to 20mm in longitudin
nodes in the mammalian body is relatively constant receiving lymph from a specific reg
on its convex border. The efferent lymphatic vessels along with blood vessels are situa
The drainage of lymph involves not only the mechanical filtration of the foreign P
lymph but also the recognition and processing of antigens. The lymph nodes exhibit a
populations are arranged in distinct interfacing compartments. This provides a favorab
components can process antigens, interact, and generate the immune response. Affer
and antigens, enters the lymph node via the subcapsular space and drains through par
that converge to form efferent lymphatic vessels through which lymph exits. B cells fro
lymph nodes from the circulation by binding to specific receptors on cells of post capilla
antigen and clonal expansion, sensitized T and B cells and antibody secreting plasma c
peripheral blood circulation via the thoracic duct.
Removal of macro molecules and excessive fluid from the interstitium also takes
escape into the tissue fluid have considerable difficulty in re-entering the vascular comp
fibrinogen that enter the interstitial fluid are usually returned to the plasma through the
where the foreign bodies are removed.
LYMPH NODE GROUPS:
2. It is estimated that 500 to 600 lymph nodes exist in humans. These nodes are lo
vessels, whose contents pass through the regional nodes to the main drainage system
good health lymph nodes are usually not palpable.
It is important to understand the basic functional anatomy of the lymphatic system
enlargement. Major lymph node groups of the body may be classified into superficial a
which are within the reach of an examiner without assistance of investigative radiograp
involvement of which is easy to diagnose and manage. It is the deep group which pose
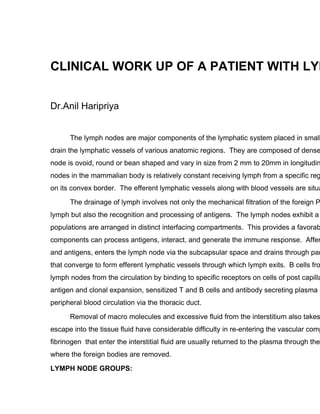
Fig. 1 : Functional architecture of the lymph node
MAJOR LYMPH NODE GROUPS:
3. SUPERFICIAL LYMPH NODE DEEP LYMPH NODE GROUPS
GROUPS
1.Superficial Cervical lymph 1. Deep Cervical lymph nodes
nodes:
2. Supra clavicular lymph nodes 2. Intra thoracic lymph nodes
(Mediastinal)
3. Extra thoracic lymph nodes 3. Para-aortic Lymph node
(axillary group)
4. Inguinal lymph nodes 4. Peri portal lymph nodes
5. Epitrochlear lymph nodes 5. Iliac lymph nodes
6. Mesenteric group of
nodes. (Lymph nodes along the
named vessels. eg. Superior and
inferior mesenteric)
Other unnamed lymph nodes
LYMPH NODES OF THE HEAD AND NECK
Approximately 75 nodes are present on each side of the neck, most of which ar
chains. Cervical group of lymph nodes are divided into superficial and deep group.
Superficial group of lymph nodes are arranged in circular chain and consist of
(a) Occipital - one or two nodes situated midway between the mastoid process and
back of the scalp.
(b) Post auricular nodes: Situated on the mastoid process behind the pinna. They dr
pinna, and external auditory meatus.
(c) Pre-auricular nodes: Situated immediately in front of the tragus, the situation is s
tragus cannot arise from this node. The node lies superficial to the parotid fascia.
scalp.
(d) Parotid nodes: These nodes are situated both in the substance of the parotid sal
4. side wall of the Pharynx. The deeper nodes drain (a) the nasopharynx (b) the back
from (a) the eyelids, (b) front of the scalp. (c) external auditary meatus (d) lymparic
(e) Submental nodes receives drainage from the skin of the chin, the midportion of t
cavity, and the nasal vestibule.
(f) Submandibular: nodes receive drainage from the submental area, the lower na
anterior oral cavity, and the skin of the midface. The submandibular nodes drain in
(g) Facial nodes: consists of superficial and deep groups.
Superficial group consists of
(a) Infraorbital: just below the orbit
(b) Buccinator: on the muscle of this name lateral to the angle of the mouth.
(c) Supramandibular: on the mandible in front of the masseter around the facial
These nodes receive lymph from conjunctiva and eyelids, nose and the neck.
Deep Group: These lie around the maxillary vessels in relation to the external ptery
infratemporal fossa (c) back of the nose (d) pharynx.
(h) Superficial Cervical nodes: These lie on the outer surface of the sternomastoid ar
parotid region and lower part of the ear.
(i) Anterior cervical nodes: These lie near the middle line of the neck in front of the l
deep set of nodes.
Superficial Set: Lie in relation to the anterior Jugular vein and drain the skin of the
Deep Set consists of:
(a) The infra hyoid nodes: These lie on the thyrohyoid membrane and drain th
(b) The prelaryngeal nodes: These lie on the cricothyroid ligament and drain th
foramen in the middle of the cricothyroid ligament. These nodes are often the
larynx. These nodes assist in the drainage of the thyroid.
5. (c) The pre tracheal nodes: These lie in relation to the inferior thyroid veins in
trachea.
Efferents of the circular chain: The deep cervical chain receives ultimately all the node
directly from all these node groups except the facial and sub mental. The efferents from
nodes.
CERVICAL LYMPH NODES.
Vertical chain of the deep cervical nodes:
This consists of a number of large nodes lying in relation to the carotid sheath. A
position behind the pharynx and are called the retropharyngeal nodes. They drain the
The vertical chain of deep cervical nodes, lies alongside the pharynx, trachea, an
the root of the neck. They are arbitrarily divided into superior deep cervical and inferior
the common carotid (or, alternatively, by the Omohyoid). The nodes of both groups are
vein. Some of the nodes of the inferior group project beyond the posterior border of the
neck (Supraclavicular). The Spinal accessory nodes are located along the spinal acces
and occipital regions of the scalp and the nape of the neck and from the upper retropha
nasopharynx, oropharynx and paranasal sinuses. The upper spinal accessory nodes d
spinal accessory nodes, which in turn drain into the supraclavicular nodes.
6. There are a few small nodes of deep cervical group which lie in the groove between the
nerve. They are called paratracheal nodes and assist in the drainage of the thyroid.
Two of the deep cervical group are named Jugulodigastric, which is the main nod
angle of mandible in the angle between the internal jugular and common fascial vein. J
common carotid just above the point where the anterior belly of the Omohyoid crosses
lymph drainage of the tongue, receiving some vessels from the apex which take a circu
(Virchow’s) nodes received drainage from the thoracic duct and are located at the junct
vein. They usually are the site of metastasis from Infraclavicular primary cancers. The
spinal accessory nodes and from infraclavicular primary cancers.
The deep cervical nodes receive the lymph from the entire head and neck either
chain. The lymph from the deep cervical chain i.e. all the lymph from that half of the he
lymph trunk, which leaves the inferior deep cervical nodes. On the right side this trunk
7. internal jugular vein. On the left side the trunk enters the thoracic duct.
Level of Nodes in Neck Dissection:
The terminology for the classification for neck dissections has been very confusin
results of treatment of neck disease because there are so many variations of neck diss
uniform. Suen and Goepert in 1987 proposed a classification of neck dissections base
recommended terminology for the nodal group was based on a modification of the Mem
This classification assigns five level of distribution to the different nodal groups.
Level I is subdivided into Level I-A (submental triangle nodes) and Level I-B (submandi
Level II includes two subgroups, Level II-A (Jugular nodes including the subdigastric ar
8. surrounding the spinal accessory nerve from the jugular foramen to the posterior borde
the (lymph nodes in the upper posterior cervical triangle above the entrance of the spin
Leve
bifurcation and the level of the carotid sheath where the omohyoid muscle crosses this
muscle.
Level IV includes sub group IV-A (Jugular nodes between the omohyoid muscle and th
the sterno cleidomastoid muscle) Level IV-B (the lymph nodes in the supra clavicular s
muscle and candal to the omohyoid muscle.
Level V includes the nodes in the posterior cervical triangle created by the posterior ed
the entrance of the spinal accessory nerve, the trapezius muscle, and the posterior bell
AXILLARY LYMPH NODES:
9. The major and primary route of drainage of lymphatics from the breast is by axilla
axilla namely the anterior, posterior, lateral, central and apical set. There are about 35
Anterior set situated along the lateral thoracic veins under the anterior axillary fold. Th
Spence is in actual contact with those nodes and therefore cancer involving this proces
Posterior set lie along the posterior axillary fold in relationship to the subscapular vesse
Lateral Set: lie along the upper part of the humerus in relation to the axillary vein.
Cent
axilla. The intercostobrachial nerve passes outwards amongst these nodes. Enlargeme
by pressure on the nerve, cause pain in the distribution of the nerve along the inner bor
is involved in carcinoma stomach via Perigastric and para oesophageal to mediastinal
as Irish node.
Apical Set: These are also called the infraclavicular nodes. They are very important an
10. first intercostal space, behind by the axillary vein, infront by the costocoracoid membran
by pushing the fingers of one hand into the axillary apex from below, and the fingers of
They are of great importance because they receive one vessel directly from the u
lymph from the breast. A single trunk leaves the apical group on each side of the subc
subclavian vein, or may join the thoracic duct on the left.
These nodes can conveniently be subdivided into three main groups according to
nodes at level 1 lie below the muscle, level 2 lymph glands lie behind it, and those of le
muscle. The majority of lymph drains from nodes at level 1 sequentially to those at leve
INGUINAL LYMPH NODES:
The lymph nodes of the lower limb are divided into superficial and deep group. The su
11. groin and are subdivided into proximal set just below and parallel to the inguinal ligame
along the upper end of long saphenous vein (vertical chain). Deep inguinal lymph node
of the femoral vein. One of these deep inguinal node lies in femoral canal called node
LYMPH NODE ENLARGEMENT:
Lymph node enlargement may occur because of proliferation of cells of the lymp
in response to antigenic stimulus or infiltration by inflammatory cells in infections involv
of malignant lymphocytes or macrophages, infiltration of nodes by metastatic malignan
laden macrophages in lipid storage diseases.
In normal immune responses, antigen stimulation of macrophages and lymphocy
lymphocytic traffic. One of the earliest effects of the antigen is to increase the blood flow
25 times of normal levels. Lymphocytes accumulate in antigen stimulated nodes by inc
of lymphocyte from antigen stimulated nodes, and proliferation of responding T and B
normal size 5 to 10 days after antigen stimulation.
DISEASES ASSOCIATED WITH LYMPHADENOPATHY:
In childhood, the lymphoid system grows rapidly. Possibly as a result of antigeni
parts of the body is an almost universal finding. Thus nearly all children under 12 years
nodes. In adults inguinal node enlargement is commonplace, presumably secondary to
generated by multiple minor injuries to the lower extremity. Enlargement of other super
the same reason, such as repeated hand injuries in manual labourers.
History and Examination:
Enlargement of lymph nodes require investigation when there are one or more n
diameter, and not known to arise from a previously recognised cause. However, this is
12. new multiple or single smaller lymph nodes may warrant investigation. While taking his
following points are particularly noted:
1. Age : Hodgkin’s disease, tuberculosis, syphilisare disease of the young, wher
old age
2. Duration: In acute lymphadenitis is short, whereas it is long in chronic lymphad
3. Which group was first affected? In case of generalised involvement of the lym
was first affected as it may give some clue to the diagnosis for example cervical
Hodgkin’s lymphoma.
4. Pain: lymph nodes are painful in both acute and chronic lymphadenitis but are
carcinoma etc.
5. Fever: evening rise in temperature is a characteristic feature of tuberculosis. In
disease intermittent bouts of recurrent fever is quite peculiar. So called Pel-Ebsta
6. Primary focus: whenever the lymph nodes are enlarged, it is usual practice to
lymph nodes for the reason of lymph node enlargement.
On examination : The following Important factors should be considered in assessing th
1. The Node location: The location of enlarged lymph nodes may suggest important clu
nodes are frequently present in scalp infections, Toxoplasmosis, and rubella, where
the eyelids and conjunctiva, Lymphomas commonly involve cervical lymph nodes an
occipital nodes as well. Enlarged suppurative cervical nodes are seen in mycobacte
lymph node enlargement suggests lymphoma or non lymphoid head and neck malig
enlargement is always significant and frequently results from metastasis from intrath
lymphoma. Virchow’s node is an enlarged left supraclavicular lymph node infiltrated
gastrointestinal tract. Unilateral axillary adenopathy can be seen with breast carcino
disease. Unilateral epitrochlear node enlargement is usually due to hand infections,
Sarcoidosis and secondary Syphillis. Bilateral inguinal adenopathy can be seen in v
13. lymphogranuloma venereum and syphilis are associated with unilateral inguinal ade
enlargement without obvious infection suggests malignant disease. Femoral node e
Pasteurella Pestis infection and lymphomas.
Enlargement of deeply situated lymph nodes may present by indirect evidence.
or mediastinal node enlargement. These patients may present with cough or wheez
nerve compression with hoarseness, paralysis of diaphragm, dysphagia with oesoph
arm due to superior vena cava or subclavian vein compression. Enlarged retroperit
limbs. Intra abdominal lymph nodes may sometimes be palpable in thin subjects.
2. The physical characteristics of the peripheral lymph nodes are important. Nodes o
discrete but occasionally they are matted. Tuberculous lymph node are matted and
are usually hard and may be fixed to underlying tissue. In acute infections, nodes a
and the overlying skin may be erythematous.
3. The clinical setting is also important in assessing lymphadenopathy. In a young c
node enlargement, infectious mono nucleosis syndromes are important to consider.
drug abusers with systemic lymphadenopathy, the acquired immunodeficiency synd
lymphadenopathy Liver and Spleen should be palpated for enlargement and nodula
Good physical examination techniques for palpation and assessment of lymph node
which diagnostic and therapeutic decisions can be based. For serial evaluation of n
size, location, consistency soft and mobility at each examination is critical. For cerv
of the seated patient to palpate the the neck and to examine in sequence the sites o
Central axillary nodes are located near the middle of the thoracic wall of the axilla
part of the humerus along the axillary vein and are best felt by having the patients a
the anterior edge of the latissmus dorsi muscle and pectoral nodes are beneath the
muscle. Infraclavicular nodes can be felt under the distal end of clavicle and may re
Epitrochlear nodes are located approximately 3 cm proximal to the medial h
14. is best accomplished by paplation of epitrochlear node area in an anterior to poster
Enlarged abdominal lymph nodes can be difficult to palpate and may be fe
nodes are best evaluated with deep palpation of the lower abdomen by rolling the ex
CAUSES OF LYMPH NODE ENLARGEMENT:
Infection:
Bacterial: Streptococci, staphylococci, anthrax, brucellosis, Pasteurella, Salmonella, H
infections: Tuberculosis, leprosy
Viral: Infectious mononucleosis syndrome (cytomegalovirus, EB Virus), Human Immuno
zoster.
Fungal: Coccidioidomycosis, histoplasmosis
Chlamydial infections: Lymphogranuloma veneram, trachoma.
Parasitic injections:Microfilariasis, trypanosomiasis.
Spirochetal-diseases: Syphillis, yaws, leptospirosis, toxoplasmosis
NEOPLASTIC
A. HEMATOLOGIC – Hodgkin’s disease, lymphomas, malignant histiocytosis & leu
B. METASTATIC TUMORS OF LYMPH NODES: Breast, Melanoma, Seminoma, tumo
gastrointestinal tract, Kapsoi’s sarcoma Neuroblastoma.
15. C. IMMUNOLOGICAL DISEASES
a) Rheumatoid arthritis
b) Systemic lypus erythematosis
c) Dermatomyositis
d) Serum Sickness
e) Drug reactions: Phenytoin, hydralazine, Allopurinol.
f) Angio immunoblastic lymphadenopathy.
D. ENDOCRINE DISEASE: hyperthyroidism
E. LIPID STORAGE DISEASE: Gaucher’s and Niemann-Pick diseases
F. MISCELLANEOUS
a) Giant follicular lymph node hyperplasia
b) Sinus histiocytosis
c) Dermatopathic lymphadenitis
d) Sarcoidosis
e) Amyloidosis
f) Muco cutaneous lymph node syndrome.
16. INVESTIGATION
The investigation of lymphadenopathy can be organised according to where nod
lymphadenopathy patients do not require a biopsy and atleast half require no labora
findings point to a benign cause for lymphadenopathy, then careful follow up at 2 to
should be instructed to return for re-evaluation if the node(s) increase in size.
Routine investigations should include a full blood count, erythrocyte sedimentatio
may be diagnostic in Leukemia, or point to a viral cause such as glandular fever. Ad
radiograph, biochemical profile, and antibody screening for an infective cause togeth
Chest Radiograph: Useful in assessment of the amount of medistinal disease, hilar
mediastinal gland enlargement is seen in Tuberculosis, sarcoidosis, lymphomas, me
histoplasmosis.
ULTRASONOGRAPHY: Is useful in screening patients suspected of abdominal lymph
or secondary to some malignancy. Its resolution is not as good as that obtained with C
response, but even then it is highly operator dependent.
COLOUR DOPPLER SONOGRAPHY : Colour Doppler Sonography is proving useful in
lymphadenopathy. On colour doppler the patterns of hilar vascularity, central nodal vas
assessed. The highest resistive index and pulsatility index are measured from special
disease 98% nodes with malignant disease and 100% of tuberculous nodes show abno
for the resistive and pulsatility indexes were highly specific for malignant lymphadenopa
CONTRAST ENHANCED CT (CECT): In recent year CT has become the main radiolo
enlargement in the mediastinum, abdomen and pelvis. It is non invasive and has the a
revealing enlargement of and can also detect enlarged nodes in the mediastinum that m
radiograph. It may also detect large deposits in the liver and spleen. In mediastinal tub
central low attenuation and peripheral rim enhancement suggests active disease, and f
17. suggested inactive disease. Low attenuation areas within the nodes had pathologic co
may be a reliable indicator for disease activity. In abdominal tuberculous lymphadenop
peripheral rim enhancement and of multilocular appearance. The enlarged lymph node
diameter. Lymphadenopathy caused by hematogenous dissemination often accompan
density foci in the spleen. The predominant sites of lymphadenopathy of disseminated
hepatogastric ligamentous, mesenteric and both upper and lower portions of the retrop
Tuberculosis all the above lymph nodes excluding the lower retroperitoneal lymph node
lymph nodes nor distinguish infiltration from reactive hymperplasia. In lymphomas it is
retroperitoneal, iliac and mesenteric lymph node groups and can also detect enlarged n
apparent on the plain chest radiograph.
M.R. EVALUATION : Magnetic resonance imaging (MRI) can help in distinguishing lym
Tuberculosis, Hodgkin’s lymphoma and metastatic lymph node enlargement Tuberculo
and T2W1, on contrast injectionmultiple hypointense foci can be seen. The metastatic
hypointense foci in T2W1, whereas the lymphomatous lymph nodes revealed heteroge
revealed mild to moderate type of enhancement, the metastatic nodes revealed dense
non contrast images.
FINE NEEDLE ASPIRATION CYTOLOGY/BIOPSY (FNAC/B): This is a simple proced
involved. However aspiration of deep central lymph nodes require the assistance of ra
endoscopy. Central lymph nodes are localized and aspirated under fluoroscopic, ultras
guidance. Fiberoptic bronchoscopy, thoracoscopy and medistianoscopy can aid in asp
to visualize abdominal lymph nodes and aspirate them by laproscopic procedures.
However the accuracy of FNAC deplends on the experience of the clinician taking th
reasonably competent cytologist certain diagnoses are relatively easy. Well differentiat
problems, nor does the confirmation of highly malignant cells. Malignant lymphoma ca
lymph node. Malignant lymphocytes in a neck node with a normal blood film confirm th
granulomatous lymph node enlargement Fine needle aspirations could be a valuable m
18. studies. The histopathological criteria used for diagnosis for tuberculosis is presence o
and presence of necrotic material with or without epitheloid cells. The entire smear is s
AFB under oil immersion and part of aspirated material should be cultured on a pair of
37 C for 8 weeks. The growth once evident is examined by Z-N staining for acid fast ba
Gaining experience in Fine needle aspiration cytology has considerably reduced the
a diagnosis in clinical enlargement of lymph nodes. When tissue is required by patholo
Needle biopsy may prove to be useful.
LYMPH NODE BIOPSY:
There are five main reasons for performing a lymph node biopsy. They are:
1. To make a diagnosis in a case of persistent unexplained lymph node enlarge
How long should one abserve an unexplained enlarged lymph node before
generally applicable answer to this question. So, much will depend on the circu
demands immediate exploration regardless of the length of history. Conversely,
children, should seldom be removed at all unless there are other indications.
2. To confirm a diagnosis suspected on other grounds. The clinical history or fin
suggestive of malignant disease, but even where the primary tumor is obvious, r
for example, to discover the histological type of a bronchial carcinoma, as a nec
the presence of multiple nodes in different groups may suggest a malignant lymp
confirm and elaborate on this diagnosis.
3. To make a diagnosis or assist in the investigation of a patient who has unexp
accompanied by lymphadenopathy.
4. To assess the extent of spread of known malignant disease.
5. To monitor the progress of disease in patients with malignant lymphoma. Tw
nodes persisting after therapy which would normally be effective in that particula
appear in a patient previously in remission after effective therapy.
19. Technique of lymph node biopsy:
It may be easy enough to remove a normal lymph node, but it often requires grea
node. For the interpretation of a difficult lymph node biopsy it is important not only that
should be subjected to the minimum of trauma in the process of removal. A badly traum
Choice of node for biopsy is also important. If there is only a single enlarged no
other hand, there is widespread lymphadenopathy, then other considerations apply. In
adults, because they so ofen show scarring or other evidence of past lymphadenitis wh
infrequently show fatty involution of their centres, so that from the histopathologist’s poi
preferred.
The most accessible node is not always the best one to remove and, generally, s
pathologist is the largest one available. All too often the surgeon is tempted to remove
representative and the diagnosis may consequently be missed. If there are multiple en
easily achieved and may give more information than can be obtained from a single nod
alike. However, there are occasions when it is necessary to obtain material from thorac
biopsied on mediastinoscopy, but it is often difficult to get a satisfactory (i.e. untraumati
to resort to open operation to make a diagnosis. Scalane node biopsy often provides u
disease eg. Sarcoidosis or Carcinoma. Abdominal nodes are commonly removed in
sites of removal of such nodes may be indicated by small metal clips to enable subsequ
preoperative/pretreatment lymphangiogram.
On receipts, the fresh node should be cleanly sliced in half with a new scalpel bla
suggest infection, one half of the node should be immediately placed in a dry sterile con
investigations. The other half of the node may then be placed in fixative. An excised l
where a diagnosis of HIV infection seems likely, and gloves should always be worn wh
Imprints are useful, not only for showing the appearance of the cells in a cytologi
Romamowsky method, for comparision with blood or bone marrow smears, but also fo
20. LYMPHANGIOGRAPHY:
Bilateral lower limb lymphangiography is an excellent method for defining abnorm
area lymph nodes, and is reportedly accurate in detecting abnormalities in these areas
technique does not help in defining abdominal nodes above the level of the kidneys or
10 to 25 percent of equivocal or false negative results. False positive results are quite
lymph nodes for some time, and can be used to follow the progress of disease during th
disordered architecture in normal sized lymph nodes.
The use of lymphangiography has declined significantly after introduction of CT s
complimentary, with similar individual sensivities and specificities. Lymphangiography
performed.
CT Lymphangiography
Mesentric and high para-aortic Internal node structu
Advantages
lymphnodes can be delineated. Images persist for mo
Of little value for dia
Needs fat for resolution thus not good in in normal size nodes
thin patients
Disadvantages
Does not image node
Cannot determine internal node structure and spleen or in mese
reaction to contrast d
LYMPHOMAS:
The lymphomas are malignant neoplastic proliferations of cells of the immune sy
involved and progressive lymphadenopathy is the most common presentation.
Historically the lymphomas have been separated on histological grounds into Ho
distinction is being partially eroded with better understanding of the biology of these con
lymphomas (of any histological sub type) are of B cell origin, with about 10 to 20 percen
Non-Hodgkin lymphoma accounts for more than three quarters of the cases of ly
21. presented in an extra nodal site such as the gut or skin, of which only four percent were
always be considered in a patient presenting with signs or symptoms affecting multiple
malaise, or unexpected weight loss.
The most common manifestation of lymphoma is lymphadenopathy. Most clinica
nodes in the neck or axillae, although involvement of internal lymph nodes (principally m
by further investigation. Involvement of lymphoid tissue in other sites (extranodal involv
lymphoma than in Hodgkin’s disease. Indeed, primary extra nodal lymphomas are virtu
sites most commonly involved are the submucosal tissues of the intestinal tract (includ
bone marrow, liver and bronchial mucosa, no site is immune.
Hodgkin’s disease appears to spread from node to contiguous mode via the lymp
widespread. Non-Hodgkin’s lymphoma spread via the blood stream, and often involve
so after malignant transformation, they are thus best considered as systemic disorder.
In general the incidence of lymphomas increase with age, and most patients that
principal exception is Hodgkin’s disease, which has in addition, a peak incidence early
The diagnosis of lymphoma is often strongly suggested by the history and clinica
affected tissue is required to establish the diagnosis and to distinguish between Hodgk
Surgical lymph node biopsy remains the ‘gold standard’ for determining the histo
aspiration of enlarged lymph nodes can be useful in distinguishing reactive from patho
frequently difficult to interpret and every effort should be made to obtain an adequate sa
knowledge can be obtained about the origin of the lymphoma from immuno-chemistry,
tissue. Biopsy samples should not, therefore, be placed automatically into formalin or o
before the biopsy is done to ensure prompt and correct handling.
PATHOLOGY:
Pathological diagnosis of Hodgkin’s disease is the presence of characteristic gia
22. histological setting.
Rye histological classification of Hodgkin’s disease:
Subgroup Major Histological features Approximate Frequency
Lymphocyte Abundant normal appearing lymphocytes 2-10%
Predominance with or without benign histiocytes,
rare RS.Cells
Nodular Sclerosis Nodules of lymphoid infiltrate of varying size,
separated by bands of collagen and containing 40-80%
numerous “lacunar cell” variants of R-S cells
Mixed cellularity Pleomorphic infiltrate of eosinophils,
Plasma cells, histiocytes and lymphocytes 20-40%
With numerous R-S cells
Lymphocytic Paucity of lymphocytes with numerous R-S cells
Depletion often bizarre in appearance, may have diffuse fibrosis 2-15%
or reticular fibres
NON-HODGKIN’S LYMPHOMA:
It has been said that nowhere in the field of pathology has there been more confu
classification of the Non-Hodgkin’s lymphoma. The most widely used classification is th
Modified Rappaport classification of Non-Hodgkin’s Lymphoma
Nodular Sub types
Lymphocytic poorly differentiated
23. Mixed lymphocytic and histiocytic
Histiocytic
Diffuse sub types
Lymphocytic well differentiated
Lymphocytic poorly differentiated
Mixed, lymphocytic and histiocytic
Lymphoblastic Lymphoma
Histiocytic
Undifferentiated (Burkitt’s or non-Burkitt’s types)
STAGING
It is important to determine as accurately as possible the full extent of involvemen
bearing on Prognosis and selection of treatment. Truly localized disease can be effecti
of cure. Chemotherapy is appropriate for more widespread disease. The staging class
Widespread use.
Ann Arbor staging classification
Stage I Involvement of a single lymph node region (I) or of a single extralymphatic orga
Sage II Involvement of two or more lymph node regions on the same side of diaphrag
or site and of one or more lymph node regions on the same side of the diaph
24. Stage III Involvement of lymph nodes on both sides of the diaphragm (III). There may
of extra lymphatic organ or site (IIIE).
Stage IV Involvement of extranodal sites, other than by direct invasion from an affecte
For each stage, qualifier ‘A’ or ‘B’ is used. ‘A’ denotes the absence and ‘B’ presence
sweats.
Staging Laparotomy: The use of staging laparotomy has markedly declined in recent
(a) advent of CECT, which is non invasive and delinerates the intra abdo
infiltrates.
(b) absence of clear survival advantage for groups of patients who have b
(c) success of chemotherapeutic regimens in controlling the disease and
stage of disease.
(d) Splenectomy carries a small but significant morbidity, risk of overwhel
Staging laparotomy should include detailed inspection of the abdomen. The rem
disease is identified in spleen total number of nodules should be enumerated. Ex
right lobe, three needle biopsies of the right and left lobes and a biopsy of any gr
palpation of the nodal groups, a biopsy should be taken from the right and left pa
removed from splenic hilar, porta, hepatic and mesenteric regions. Iliac bone ma
operation.
BIBLIOGRAPHY
1. LYMPH NODE PATHOLOGY, Second Edition, Harry L. loachim. J.B. Olippincott Company, Philadelph
2. Slevens A, Lowe J. Histology. London: Gower Medical Publishing 1992
3. Ehrich, W.E.: The role of the lymphocyte in the circulation of lymph . Ann. NY Acad Sci, 46:823, 1946
4. Arno J 91980) Atlas of lymph node Pathology M.T.P. Press, Lancaster.
5. GAG Decker, D.J. Dee Plessis: Lee Mc Gregor’s Synopsis of SURGICAL ANATOMY 12th Ed. (1986)
25. 6. Suen J.Y., Goeptent H: Editorial standerization of neck dissection nomenclature., Head Neck Surg 1
7. Shah J.P., Strong E, Spiro RH, Vikram B: Neck dissection: current status and future possibilities. Cl
8. Turner – warwick RT. The lymphatics of the breast Br J Surg. 1959, 46: 574-82
9. Butcher E., Weissman I, Lymphoid tissues and organs in WE Paul (ed). New York, Raven 1984 pp 109
10. Na DG, Lim HG, Byun HS, Kim HD, K.YH: Differential diagnosis of cervical lymphadenopathy. Usefuln
Mar, 170(3): 715-718
11. Yang 2, Sone S, Min P, etal. Distribution of contrast enhanced CT appearance of abdominal tuberculo
12. Bergsagel. D.E. etal (1982) Results of treating Hodgkin’s disease without a policy of laparotomy stag
13. Carbone P.B., Kaplan H.S. Musshof K. Smithers D.W. and Tubiana M. (1921). Report on the committe
31, 1860-1